
Abstract
The cell of origin of ovarian cancer has been long debated. The current paradigm is that epithelial ovarian cancer (EOC) arises from the ovarian surface epithelium (OSE). OSE is composed of flat, nondescript cells more closely resembling the mesothelium lining the peritoneal cavity. In light of various histologic types of ovarian carcinoma (serous, endometrioid, and clear cell carcinoma), which have a Müllerian phenotype, it has been argued that the OSE undergoes a process termed “metaplasia” to account for this profound morphologic transformation. Recent molecular and clinicopathologic studies not only have failed to support this hypothesis but also have provided evidence that EOC stems from Müllerian-derived extraovarian cells that involve the ovary secondarily, thereby calling into question the very existence of primary EOC. This new model of ovarian carcinogenesis proposes that fallopian tube epithelium (benign or malignant) implants on the ovary to give rise to both high-grade and low-grade serous carcinomas, and that endometrial tissue implants on the ovary and produces endometriosis, which can undergo malignant transformation into endometrioid and clear cell carcinoma. Thus, ultimately EOC is not ovarian in origin but rather is secondary, and it is logical to conclude that the only true primary ovarian neoplasms are germ cell and gonadal stromal tumors analogous to tumors in the testis. If this new model is confirmed, it has profound implications for the early detection and treatment of “ovarian cancer”.
Similar content being viewed by others


Introduction
Advances in radical surgery and cytotoxic chemotherapy have extended survival but have not reduced the overall mortality in ovarian cancer patients, and there is currently no effective screening strategy [1•, 2], largely because of inadequate understanding of the early events of ovarian carcinogenesis. Unlike cancers arising in the colon, breast, cervix, endometrium, prostate, and pancreas, where the early events of carcinogenesis can be studied because their precursor lesions have been recognized, a precursor lesion of epithelial ovarian cancer (EOC) has not been identified despite diligent research over the past 30 years. As a result, efforts at early detection and screening, which have been highly successful for other cancers (notably cervical cancer), have not provided a survival benefit for women with EOC because the screening methods have been empirical instead of being grounded in a firm understanding of the mechanisms of ovarian carcinogenesis [1•]. In addition, confirmation that the screening test has, in fact, detected ovarian cancer requires laparoscopy at the minimum because the ovary lies deep in the pelvis; therefore the screening test must be highly specific. Also, ovarian cancer appears to evolve relatively rapidly, unlike cervical cancer, in which the transit time from a preinvasive to an invasive carcinoma may be 10 years or longer [3]. Finally, the goal of screening has been to detect EOC while it is still confined to the ovary (stage I), but recent studies strongly suggest that EOC frequently begins outside the ovary. Accordingly, it has been proposed that the goal of screening should shift from the detection of disease confined to the ovary to the detection of low-volume disease anywhere in the pelvis [4]. This review revisits the issue of the site of origin of ovarian carcinoma and its possible impact on future ovarian cancer research and management.
Ovarian Carcinoma is a Heterogenous Group of Diseases
The ovary has the largest number of tumor types in the body. Ovarian tumors can be divided into four main categories: EOC, germ cell tumors, gonadal stromal tumors, and metastatic neoplasms [5]. The most common ovarian malignancies are the EOCs, and this review is confined to this group.
EOCs comprise several different histologic types, which can be grouped into two broad categories, type I and type II [6]. This categorization not only has clinical utility but also sheds light on their pathogenesis. Type I tumors, which include low-grade serous, low-grade endometrioid, clear cell, and mucinous carcinoma, typically present as a large mass confined to one ovary (stage Ia), and they have a relatively good outcome. Type I tumors typically display a variety of somatic mutations that involve ARID1A, BRAF, CTNNB1, KRAS, PIK3CA, PPP2R1A, and PTEN; only rarely are BRCA1, BRCA2, or TP53 involved (Fig. 1) [6–9]. These tumors develop in a stepwise fashion from precursor lesions such as borderline tumors and endometriosis. In contrast, type II tumors include high-grade serous carcinoma, high-grade endometrioid carcinoma, malignant mixed mesodermal tumors (carcinosarcomas), and undifferentiated carcinomas, which are highly aggressive and almost always present in advanced stages (stages II–IV). High-grade serous carcinoma is the prototypic type II tumor. It harbors TP53 mutations in more than 95% of cases, mutations in BRCA1 and BRCA2 in approximately 10–20% and hypermethylation of the BRCA1 promoter in 10–40% of cases [10]. These tumors only rarely display the mutations typically found in the type I group. Based on DNA copy number alterations, the genome of type II cancers is much less stable than that of the type I tumors [11, 12].

Morphologic and molecular genetic features that characterize each major subtype of ovarian carcinoma. The top panels of photomicrographs illustrate their histologic features. The bottom table shows the frequency of sequence mutations of oncogenes and tumor suppressor genes in a heat map. The frequency of mutation is represented by the gradient of colors, from green (low frequency) to brown (high frequency). Of note, the case number is too small to be conclusive for PPP2R1A mutations in mucinous tumor. HG, high-grade serous carcinoma; LG, low-grade serous carcinoma; CC, clear cell carcinoma; EM, endometrioid carcinoma; MU, mucinous carcinoma
Conventional View of How Ovarian Cancer Develops
The ovary is composed of germ cells and stromal cells and is covered by a single layer of epithelium, which is termed the ovarian surface epithelium (OSE). The OSE is regarded as a specialized form of mesothelium that is continuous with the peritoneal lining of the pelvic cavity, with which it is morphologically and immunohistochemically identical [13]. In addition, small epithelium-lined cysts termed “cortical inclusion cysts” (CICs) can be present in the ovarian cortex. These cysts are thought to arise as a result of invagination of the OSE, and a number of investigators have proposed that, together with the OSE, they may be the site of origin of EOC.
A number of epidemiologic studies have concluded that ovarian cancer is linked to ovulation, based on a significant reduction in risk related to parity and oral contraceptive use [14], both of which are associated with a decrease in ovulation. Consequently the theory of “incessant ovulation” proposed by Fathalla [15] has gained widespread currency. According to this theory, ovulation, which involves rupture of the OSE to permit egress of the oocyte, is associated with repeated trauma and repair, which cause DNA damage and can lead to neoplastic transformation of the OSE, the CICs, or both [15]. To account for the Müllerian phenotype of EOCs from OSE, which is mesothelial in nature, it is argued that the OSE undergoes metaplastic changes resulting in a Müllerian phenotype prior to malignant transformation [16]. “Metaplasia” is defined as a benign cellular process that gives rise to different morphologically distinct cell types by reprogramming the cellular differentiation. For example, the presence of glands in the endometrium lined by ciliated epithelium is referred to as “tubal (ciliated) metaplasia.” This complex alteration from resting, nondescript mesothelium to cells resembling fallopian tube and endometrial tissue is difficult to comprehend, as has been pointed out by Dubeau [17], who dismisses the entire concept as a fable. Nonetheless, some argue that OSE is a specialized mesothelium, which adopts the Müllerian phenotype because of its anatomic location and unique microenvironment on the ovarian surface [13]. Convincing evidence for this proposal is lacking. Perhaps the most cogent evidence arguing against the origin of EOC from the OSE or CICs is that despite a diligent search for precursor lesions in the ovary for more than 30 years, no well-accepted precursor has been found, except in very rare instances. Thus, in rare cases, cytologic abnormalities in the epithelial lining of CICs classified as “dysplasia” has been reported in the ovaries of high-risk women [18–21], but other studies have failed to confirm these findings [16–19]. It is noteworthy that a significant pitfall in the studies describing precursor lesions involving the OSE immediately adjacent to high-grade serous carcinoma is that they have not taken into account that the “precursor” lesion is not a real precursor, but instead represents lateral spread of the carcinoma on the surface. As a result, an alternative hypothesis has proposed the “secondary Müllerian system” as the origin of EOCs, to account for the Müllerian phenotype expressed by ovarian cancers [17]. The secondary Müllerian system, in contrast to the primary Müllerian system (which gives rise to the upper part of the vagina, the endometrium, and the fallopian tubes), includes a variety of epithelial structures such as paraovarian and paratubal cysts, endometriosis, and endosalpingiosis. Although this system would explain the Müllerian appearance of EOCs, it is inconsistent with the fact that primary EOCs have almost never been reported in these locations.
Tubal Origin of High-Grade Serous Carcinomas
The term “serous” has been used to describe the tumor type with morphologic features resembling the epithelial cells in the fallopian tube. However, the possibility that tubal epithelium gives rise to ovarian serous carcinoma has only recently gained ground. In 2001, Piek et al. [22] described dysplastic lesions similar to high-grade serous carcinoma in the fallopian tube, but not in the ovary, of patients with a genetic predisposition to EOC who were undergoing prophylactic salpingo-oophorectomy. This finding prompted pathologists to carefully examine fallopian tubes using a new protocol (SEE-FIM), which involved sectioning and extensively examining the fimbriated end. In the past, only a few representative sections of the fallopian tubes were submitted for microscopic examination because it was presumed that precursors of ovarian carcinoma would logically be in the ovaries. As a result of the adoption of the SEE-FIM protocol, occult intraepithelial and invasive tubal carcinomas have been detected in association with EOCs.
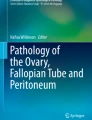
The tubal lesion that is related to high-grade serous carcinoma, termed “serous tubal intraepithelial carcinoma (STIC),” is morphologically characterized by stratified, disorganized, enlarged epithelial cells with highly atypical nuclei (Fig. 2). There are several lines of evidence supporting the tubal origin of high-grade serous carcinoma. First, STICs and early invasive tubal carcinomas occur not only in 10–15% of women with a germ-line mutation placing them at high risk for “ovarian” cancer but also in 50–60% of women with sporadic ovarian cancer (without either family history or known BRCA mutations) [23•, 24, 25]. Second, molecular genetic studies have demonstrated identical TP53 mutations in STICs and concurrent ovarian high-grade serous carcinomas, indicating a clonal relationship between them [26, 27•]. Third, a genome-wide gene expression profiling study further showed that the gene expression signature of high-grade serous carcinoma is more closely related to fallopian tube epithelium than to OSE or endometrial or colonic epithelium [28]. Consistent with this view, immunohistochemical studies demonstrate that high-grade serous carcinoma expresses PAX8, a Müllerian marker, but not calretinin, a mesothelial marker. This finding is important because if high-grade serous carcinoma arises from OSE, it should express calretinin but not PAX8, because OSE is embryonically and morphologically related to mesothelial cells rather than Müllerian epithelium. Fourth, besides co-expressing p53, STICs and concurrent ovarian high-grade serous carcinoma also express several tumor-associated oncoproteins, including fatty acid synthase, Rsf-1, and cyclin E1, whereas these proteins are rarely detected in the adjacent normal tubal epithelium [29]. Finally, analysis of telomere length using in situ hybridization reveals that, like many other precancerous lesions, STICs have shorter telomeres than the associated normal epithelium [30]. All these findings lend further support to the proposal that the tubal epithelium is the likely cell of origin of high-grade serous carcinoma, and STIC represents its precursor lesion. Table 1 summarizes the evidence for and against various ovarian and tubal lesions as precursors of high-grade serous carcinoma and lists the studies on each side.

The histology and expression of Ki-67, p53, and p16 in a serous tubal intraepithelial carcinoma (STIC). Hematoxylin and eosin (H&E) stained fallopian tube section shows a STIC, composed of enlarged and highly atypical tumor cells, forming a multilayered architecture. No evidence of invasion is noted. In contrast, the adjacent normal fallopian tube epithelium (FTE) contains single-layered, smaller and homogenous epithelial cells. The area was immunostained with antibodies reacting to Ki-67, p53, and p16. The percentage of Ki-67 labeled cells is greater in STIC than in normal fallopian tube epithelium, indicating a higher proliferative activity in STIC. p53 staining is undetectable in STIC because the lesion harbors a truncating mutation in TP53. STIC cells demonstrate diffuse p16 immunoreactivity, suggesting an Rb pathway aberration
Why the tubal epithelium is vulnerable to neoplastic transformation and how carcinogenesis proceeds remains speculative. As previously noted, epidemiologic studies have shown that the risk of ovarian cancer correlates directly with the number of ovulations during a woman’s life, as oral contraceptive use or pregnancy and lactation substantially reduce the risk of ovarian cancer. Women with more than two pregnancies have a 50% decrease in EOC risk, and oral contraceptive use for more than 5 years decreases EOC risk by about 50% [31–33]. Several explanations for these observations have been offered. It has been hypothesized that oxidative stress, directly related either to exposure of the fimbria (where most STICs are found) to follicular fluid containing reactive oxygen species or to other microenvironmental factors associated with rupture of the OSE at ovulation, results in DNA damage to epithelial cells [34–36]. Repeated DNA damage in response to multiple ovulations may facilitate the selection for TP53 mutations, telomere shortening, or both in tubal epithelial cells, resulting in chromosomal instability that leads to a repertoire of tumor subclones, some of which may acquire malignant phenotypes, including STICs (Fig. 3). These cells then detach and implant on the ovary and peritoneal surfaces. It is likely that the microenvironment in the ovary is more favorable for further tumor development than in the fallopian tube, so the tumor enlarges in the ovary and appears to be a primary ovarian cancer rather than a tubal cancer.

Hypothesis for the tubal origin of ovarian high-grade serous carcinoma (HGSC). We hypothesize that normal fallopian tube epithelium (FTE) is the cell of origin of many “ovarian” HGSCs. Rupture of the dominant follicle at ovulation exposes the underlying ovarian stroma to fimbrial epithelium, which can implant on the ruptured ovarian surface. Inflammation and repair occur in the presence of follicular fluid, which contains a high concentration of reactive oxygen species (ROS, red dots). The increased genotoxic effects may facilitate the selection of TP53 mutations in epithelial cells, which clonally expand. As a result, telomere shortening occurs and enhances underlying chromosomal instability (CIN), creating a repertoire of tumor subclones in serous tubal intraepithelial lesions (STIL), some of which may acquire malignant phenotypes (serous tubal intraepithelial carcinoma, STIC) and exfoliate onto the ovarian and peritoneal surfaces. In summary, FTE may lead to ovarian HGSC by two different mechanisms: (1) normal FTE implants on the ruptured ovarian surface at ovulation, which invaginates to form an inclusion cyst that subsequently undergoes malignant transformation (possibly after a TP53 mutation), or (2) STIC cells implant on the ovary and then form a tumor mass. In both instances, the ovarian HGSC is of tubal origin
Tubal Origin of Low-Grade Serous Carcinomas
It has been well established that ovarian low-grade serous carcinoma is distinct from high-grade serous carcinoma [9, 10]. Unlike high-grade serous carcinoma, invasive low-grade serous carcinoma develops through multiple intermediate stages, mimicking the adenoma-carcinoma sequence in colorectal carcinoma, in which carcinoma evolves through a continuum of histologically recognizable precursor lesions [37]. Recent findings based on clinicopathologic and immunohistochemical studies have provided new evidence that low-grade serous neoplasms of the ovary are more closely related to tubal epithelium than to OSE, leading to a proposal that low-grade serous carcinoma also develops from tubal epithelium [38]. The putative precursor lesion has been designated “papillary tubal hyperplasia” (PTH), in which hyperplastic tubal epithelium forms small intraluminal buds (micropapillae) often associated with psammoma bodies that are pinched off, float into the tubal lumen, and then implant on ovarian and peritoneal surfaces. These implanted lesions can result in endosalpingiosis, atypical proliferative serous tumors, and noninvasive implants. We speculate that the mechanism by which tubal epithelium implants on the ovary (either in the form of normal tubal epithelium or PTH) is related to ovulation. At the time of ovulation, the fimbriated end of the fallopian tubes is closely applied to the ovarian surface in order to facilitate the transfer of the oocyte from the ruptured ovarian follicle to the fallopian tube. At the rupture site, the fallopian tube epithelium is exposed directly to the ovarian stroma, as well as to antrum fluid. We hypothesize that the ovarian microenvironment facilitates tumor progression of the implanted tubal epithelium (presumably the tubal stem cells) to form a CIC, followed by clonal expansion into an ovarian serous cystadenoma. A number of events associated with ovulation and retrograde passage of menstrual blood may play a role in malignant transformation: at the follicle rupture site, an inflammatory reaction with the release of cytokines, growth factors, and free oxygen radicals is present in follicular fluid; hemolyzed blood from the rupture site or retrograde menstruation can release iron and free radicals; or stimulation by the hormone-rich ovarian stroma may induce neoplastic transformation. Histopathologic analysis demonstrates that serous cystadenomas may undergo proliferation to form a tumor termed “atypical proliferative serous tumor” and an intraepithelial (in situ) carcinoma termed “noninvasive micropapillary serous carcinoma” (collectively known as “serous borderline tumors”), which are thought to be the immediate precursors of invasive low-grade serous carcinoma [39].
Endometrial Origin of Ovarian Clear Cell and Endometrioid Carcinoma
There is evidence to support the endometrial origin of both ovarian endometrioid and clear cell carcinoma. The thought that endometriosis could represent the precursor lesion of some EOCs dates as far back as 1927 [40]. Since then, numerous clinical, histopathologic, and (more recently) molecular studies have supported this concept. Both ovarian endometrioid and clear cell carcinomas are frequently associated with ovarian endometriotic cysts, as approximately 40% of ovarian endometrioid carcinomas and 50–90% of clear cell carcinomas are associated with endometriosis [41]. Moreover, a morphologic continuum of tumor progression is evident in many cases [42, 43]. Patients with endometriosis have an increased risk (about 2–4 times) of developing ovarian endometrioid and clear cell carcinoma [44]. Tubal ligation, which prevents retrograde flow of menstrual endometrium to adnexal tissues, has been found to reduce the incidence of ovarian endometrioid and clear cell carcinoma [45]. A clonality study has demonstrated that endometriosis is related to concurrent ovarian endometrioid and clear cell carcinomas in the same patient [46]. Moreover, somatic mutations of ARID1A, a gene involved in chromatin remodeling [47], have recently been reported in a large proportion of endometrium-related neoplasms, including 46–57% of ovarian clear cell carcinomas [7, 8], 40% of uterine endometrioid carcinomas [48], and 30% of ovarian endometrioid carcinomas [8], but these mutations are rarely reported (≤ 10%) in other types of carcinomas [49]. The vast majority of ARID1A mutations are either non-sense or frameshift mutations, resulting in loss of protein expression [8, 48]. Using ARID1A as a marker, we and others have shown the same ARID1A mutations in endometriosis and adjacent clear cell carcinoma [8], and in most cases ARID1A immunoreactivity has been lost in both ovarian endometriotic cysts and associated endometrioid and/or clear cell carcinomas (Ayhan et al., unpublished data). These findings support the role of endometriosis as a precursor of ovarian endometrioid and clear cell carcinoma and suggest that loss of ARID1A expression (presumably due to a mutation) is an early molecular event in the development of ovarian endometrioid and clear cell carcinomas, mostly occurring before malignant transformation.
Impact and Future Perspectives
The purported extraovarian origin of EOCs has profound biological and clinical implications, especially in the early detection and prevention of high-grade serous carcinomas. As STIC cells may disseminate not only to ovarian but also to peritoneal surfaces early in tumor development, one can argue that the majority of ovarian high-grade serous carcinomas are at an advanced stage even though there are no grossly detectable tumor nodules outside the ovary. Therefore, the tubal origin of high-grade serous carcinomas, if validated, may explain why methods of early detection such as CA125 and transvaginal ultrasound have neither improved the detection of stage I high-grade serous carcinoma nor reduced mortality [1•, 3, 50]. In addition, the current approach to prophylaxis needs to be re-evaluated not only for women at high risk of developing ovarian cancer but also for the general female population. Currently, the standard approach for reducing risk for women with BRCA1/2 mutations or with a family history of ovarian carcinoma has been bilateral salpingo-oophorectomy with or without hysterectomy. For women at high risk, an argument could be made to remove only the fallopian tubes and conserve the ovaries before menopause, because high-grade serous carcinoma develops from the fallopian tubes and involves the ovaries secondarily. Oophorectomy could be delayed until after menopause [51]. This approach would preserve fertility and hormonal function in premenopausal women. Similarly, for women who are not considered to be at high risk but who undergo a hysterectomy for benign uterine causes, bilateral salpingectomy with sparing of the ovaries may be considered in order to improve quality of life and overall survival while still reducing the risk of ovarian carcinoma. A recent prospective study of nearly 30,000 women showed that bilateral oophorectomy at the time of hysterectomy, compared with ovarian preservation, was associated with increased mortality from all causes and an increased risk of nonfatal coronary heart disease. Similarly, salpingectomy rather than tubal ligation would be effective in reducing ovarian cancer risk for women considering a more permanent type of contraception. Future clinical studies are necessary to confirm the efficacy of these approaches before they are introduced into clinical practice [51].
The new paradigm of ovarian carcinogenesis, in which it is recognized that EOC consists of multiple tumor types with different clinicopathologic and molecular genetic features and most carcinomas arise from cells outside the ovary and involve it secondarily, has refocused research in the field and has opened up potential new avenues in clinical management. Studying the early molecular changes associated with STICs not only will allow the discovery of reliable biomarkers for detection of low-volume disease but also may ultimately lead to the identification of molecular targets that may prove useful for targeted therapy using small molecule inhibitors, neutralizing antibodies, and novel cell-based immunotherapy. Accordingly, new approaches to management should focus on prevention and detection of very early lesions such as STICs, as chemotherapy of established carcinomas is not nearly as effective. To this end, a previous report demonstrated that STICs overexpress fatty acid synthase, for which a small molecule inhibitor has been available [29]. In addition, STICs upregulate several cancer-associated genes such as cyclin E1 and Rsf-1, which may serve as candidate molecules in developing prophylactic immunotherapy to eradicate STICs [29].
Conclusions
The failure of radical surgery and chemotherapy to reduce the overall mortality of ovarian cancer, in contrast to the improvement of outcome for many other major cancer types, can be attributed to a lack of understanding of its pathogenesis. Accumulated evidence from recent clinicopathological, immunohistochemical, and molecular genetic studies strongly suggests that the cell of origin of most EOCs resides in extraovarian organs. In particular, it appears that both high-grade and low-grade serous carcinomas are probably derived from fallopian tubal epithelium. The high-grade serous carcinomas develop from dissemination of STIC cells or from CICs in the ovary that are derived from tubal epithelium, whereas low-grade serous carcinoma progresses from an ovarian borderline tumor, which developed from tubal epithelium shed from “papillary tubal hyperplasia” or tubal epithelium that had formed an ovarian CIC. Finally, ovarian endometrioid and clear cell carcinomas arise from ectopic endometrium implanted on the ovary (endometrioma). Therefore, it now appears that most EOCs develop from implanted tumor precursors imported from either the fallopian tube or the endometrium rather than from the OSE itself. If this hypothesis of the extraovarian origin of “ovarian” cancer is validated, the true primary ovarian neoplasms would include only germ cell and gonadal stromal tumors, analogous to testicular neoplasms. Although several critical experiments are still needed to confirm this model, the new paradigm of the extraovarian origin of EOCs will have profound implications for research and clinical management.
References
Recently published papers of interest have been highlighted as: • Of importance
• Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA 2011;305:2295–2303. This population-based study analyzed the PLCO cases in an attempt to determine whether CA125 and an imaging study can save the lives of ovarian cancer patients. The study result provides cogent evidence of a lack of effective screening to reduce ovarian cancer deaths.
Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90.
Fishman DA, Cohen L, Blank SV, et al. The role of ultrasound evaluation in the detection of early-stage epithelial ovarian cancer. Am J Obstet Gynecol. 2005;192:1214–21. discussion 1221–1212.
Kurman RJ, Visvanathan K, Roden R, et al. Early detection and treatment of ovarian cancer: shifting from early stage to minimal volume of disease based on a new model of carcinogenesis. Am J Obstet Gynecol. 2008;198:351–6.
Seidman JD, Cho K, Ronnett BM, et al. Surface epithelial tumors of the ovary. In: Kurman RJ, Ellenson LH, Ronnett BM, editors. Blaustein’s Pathology of the Female Genital Tract. New York: Springer Verlag; 2011. p. 679–784.
Shih IM, Kurman RJ. Ovarian tumorigenesis: a proposed model based on morphological and molecular genetic analysis. Am J Pathol. 2004;164:1511–8.
Jones S, Wang TL, Shih IM, et al. Frequent mutations of chromatin remodeling gene ARID1A in ovarian clear cell carcinoma. Science. 2010;330:228–31.
Wiegand KC, Shah SP, Al-Agha OM, et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med. 2010;363:1532–43.
Jones S, Wang TL, Kurman RJ, et al. Low-grade serous carcinomas of the ovary contain very few point mutations. J Pathol 2011 Nov 21 (Epub ahead of print).
Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature. 2011;474:609–15.
Kuo K, Mao T, Feng Y, et al. DNA copy number profiles in affinity-purified ovarian clear cell carcinoma. Clin Cancer Res. 2010;16:1997–2008.
Kuo KT, Guan B, Feng Y, et al. Analysis of DNA copy number alterations in ovarian serous tumors identifies new molecular genetic changes in low-grade and high-grade carcinomas. Cancer Res. 2009;69:4036–42.
Auersperg N. The origin of ovarian carcinomas: a unifying hypothesis. Int J Gynecol Pathol. 2011;30:12–21.
McLaughlin JR, Risch HA, Lubinski J, et al. Reproductive risk factors for ovarian cancer in carriers of BRCA1 or BRCA2 mutations: a case–control study. Lancet Oncol. 2007;8:26–34.
Fathalla MF. Incessant ovulation–a factor in ovarian neoplasia? Lancet. 1971;2:163.
Auersperg N, Wong AS, Choi KC, et al. Ovarian surface epithelium: biology, endocrinology, and pathology. Endocr Rev. 2001;22:255–88.
Dubeau L. The cell of origin of ovarian epithelial tumors and the ovarian surface epithelium dogma: Does the emperor have no clothes? Gynecol Oncol. 1999;72:437–42.
Cai KQ, Wu H, Klein-Szanto AJ, et al. Acquisition of a second mutation of the Tp53 alleles immediately precedes epithelial morphological transformation in ovarian tumorigenicity. Gynecol Oncol. 2009;114:18–25.
Deligdisch L. Ovarian dysplasia: a review. Int J Gynecol Cancer. 1997;7:89–94.
Deligdisch L, Gil J, Kerner H, et al. Ovarian dysplasia in prophylactic oophorectomy specimens: cytogenetic and morphometric correlations. Cancer. 1999;86:1544–50.
Yang DH, Smith ER, Cohen C, et al. Molecular events associated with dysplastic morphologic transformation and initiation of ovarian tumorigenicity. Cancer. 2002;94:2380–92.
Piek JM, van Diest PJ, Zweemer RP, et al. Dysplastic changes in prophylactically removed Fallopian tubes of women predisposed to developing ovarian cancer. J Pathol. 2001;195:451–6.
• Przybycin CG, Kurman RJ, Ronnett BM, et al. Are all pelvic (nonuterine) serous carcinomas of tubal origin? Am J Surg Pathol 2010;34:1407–1416. This study was based on a relatively large retrospective cohort to demonstrate the percentage of ovarian cancer that is associated with serous tubal intraepithelial carcinoma. The results provide evidence that most so-called ovarian cancers are associated with concurrent serous tubal intraepithelial carcinoma.
Finch A, Shaw P, Rosen B, et al. Clinical and pathologic findings of prophylactic salpingo-oophorectomies in 159 BRCA1 and BRCA2 carriers. Gynecol Oncol. 2006;100:58–64.
Callahan MJ, Crum CP, Medeiros F, et al. Primary fallopian tube malignancies in BRCA-positive women undergoing surgery for ovarian cancer risk reduction. J Clin Oncol. 2007;25:3985–90.
Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am J Surg Pathol. 2007;31:161–9.
• Kuhn E, Kurman RJ, Vang R, et al. TP53 mutations in serous tubal intraepithelial carcinoma and concurrent pelvic high-grade serous carcinoma—evidence supporting the clonal relationship of the two lesions. J Pathol 2011 Oct 12. doi:10.1002/path.3023. This recent study shows the mutational profiles of TP53 in high-grade ovarian serous carcinoma and concurrent serous tubal intraepithelial carcinoma. The results from this report demonstrate that both lesions share identical TP53 mutations, suggesting their clonal relationship and supporting the idea that serous tubal intraepithelial carcinoma may be the precursor of high-grade ovarian serous carcinoma.
Marquez RT, Baggerly KA, Patterson AP, et al. Patterns of gene expression in different histotypes of epithelial ovarian cancer correlate with those in normal fallopian tube, endometrium, and colon. Clin Cancer Res. 2005;11:6116–26.
Sehdev AS, Kurman RJ, Kuhn E, et al. Serous tubal intraepithelial carcinoma upregulates markers associated with high-grade serous carcinomas including Rsf-1 (HBXAP), cyclin E and fatty acid synthase. Mod Pathol. 2010;23:844–55.
Kuhn E, Meeker A, Wang TL, et al. Shortened telomeres in serous tubal intraepithelial carcinoma: an early event in ovarian high-grade serous carcinogenesis. Am J Surg Pathol. 2010;34:829–36.
Fleming JS, Beaugie CR, Haviv I, et al. Incessant ovulation, inflammation and epithelial ovarian carcinogenesis: revisiting old hypotheses. Mol Cell Endocrinol. 2006;247:4–21.
Purdie DM, Bain CJ, Siskind V, et al. Ovulation and risk of epithelial ovarian cancer. Int J Cancer. 2003;104:228–32.
La Vecchia C. Oral contraceptives and ovarian cancer: an update, 1998–2004. Eur J Cancer Prev. 2006;15:117–24.
von Zglinicki T. Oxidative stress shortens telomeres. Trends Biochem Sci. 2002;27:339–44.
Murdoch WJ, Martinchick JF. Oxidative damage to DNA of ovarian surface epithelial cells affected by ovulation: carcinogenic implication and chemoprevention. Exp Biol Med (Maywood). 2004;229:546–52.
Murdoch WJ. Carcinogenic potential of ovulatory genotoxicity. Biol Reprod. 2005;73:586–90.
Ho CL, Kurman RJ, Dehari R, et al. Mutations of BRAF and KRAS precede the development of ovarian serous borderline tumors. Cancer Res. 2004;64:6915–8.
Kurman RJ, Vang R, Junge J, et al. Papillary tubal hyperplasia: the putative precursor of ovarian atypical proliferative (borderline) serous tumors, noninvasive implants, and endosalpingiosis. Am J Surg Pathol. 2011;35:1605–14.
Shih IM, Kurman RJ. Molecular pathogenesis of ovarian borderline tumors: new insights and old challenges. Clin Cancer Res. 2005;11:7273–9.
Sampson JA. Metastatic or embolic endometriosis, due to the menstrual dissemination of endometrial tissue into the venous circulation. Am J Pathol. 1927;3:93–110.43.
Veras E, Mao TL, Ayhan A, et al. Cystic and adenofibromatous clear cell carcinomas of the ovary: distinctive tumors that differ in their pathogenesis and behavior: a clinicopathologic analysis of 122 cases. Am J Surg Pathol. 2009;33:844–53.
Fukunaga M, Nomura K, Ishikawa E, et al. Ovarian atypical endometriosis: its close association with malignant epithelial tumours. Histopathology. 1997;30:249–55.
Russell P. The pathological assessment of ovarian neoplasms. I: Introduction to the common ‘epithelial’ tumours and analysis of benign ‘epithelial’ tumours. Pathology. 1979;11:5–26.
Kokcu A. Relationship between endometriosis and cancer from current perspective. Arch Gynecol Obstet. 2011;284:1473–9.
Rosenblatt KA, Thomas DB. Reduced risk of ovarian cancer in women with a tubal ligation or hysterectomy. The World Health Organization Collaborative Study of Neoplasia and Steroid Contraceptives. Cancer Epidemiol Biomarkers Prev. 1996;5:933–5.
Thomas EJ, Campbell IG. Molecular genetic defects in endometriosis. Gynecol Obstet Invest. 2000;50 Suppl 1:44–50.
Guan B, Wang TL, Shih IM. ARID1A, a factor that promotes formation of SWI/SNF-mediated chromatin remodeling, is a tumor suppressor in gynecologic cancers. Cancer Res. 2011;71:6718–27.
Guan B, Mao TL, Panuganti PK, et al. Mutation and loss of expression of ARID1A in uterine low-grade endometrioid carcinoma. Am J Surg Pathol. 2011;35:625–32.
Jones S, Li M, Parsons DW, et al. Somatic mutations in the chromatin remodeling gene ARID1A occur in several tumor types. Hum Mutat. 2011;33:100–3.
Karlan BY, Baldwin RL, Lopez-Luevanos E, et al. Peritoneal serous papillary carcinoma, a phenotypic variant of familial ovarian cancer: implications for ovarian cancer screening. Am J Obstet Gynecol. 1999;180:917–28.
Collins IM, Domchek SM, Huntsman DG, et al. The tubal hypothesis of ovarian cancer: caution needed. Lancet Oncol;12:1089–1091.
Shaw PA, Rouzbahman M, Pizer ES, et al. Candidate serous cancer precursors in fallopian tube epithelium of BRCA1/2 mutation carriers. Mod Pathol. 2009;22:1133–8.
Piek JM, van Diest PJ, Verheijen RH, et al. Cell cycle-related proteins p21 and bcl-2: markers of differentiation in the human fallopian tube. Histopathology. 2001;38:481–2.
Piek JM, van Diest PJ, Zweemer RP, et al. Tubal ligation and risk of ovarian cancer. Lancet. 2001;358:844.
Piek JM, Verheijen RH, Kenemans P, et al. BRCA1/2-related ovarian cancers are of tubal origin: a hypothesis. Gynecol Oncol. 2003;90:491.
Paley PJ, Swisher EM, Garcia RL, et al. Occult cancer of the fallopian tube in BRCA-1 germline mutation carriers at prophylactic oophorectomy: a case for recommending hysterectomy at surgical prophylaxis. Gynecol Oncol. 2001;80:176–80.
Folkins AK, Saleemuddin A, Garrett LA, et al. Epidemiologic correlates of ovarian cortical inclusion cysts (CICs) support a dual precursor pathway to pelvic epithelial cancer. Gynecol Oncol. 2009;115:108–11.
Salvador S, Gilks B, Kobel M, et al. The fallopian tube: primary site of most pelvic high-grade serous carcinomas. Int J Gynecol Cancer. 2009;19:58–64.
Jarboe EA, Folkins AK, Drapkin R, et al. Tubal and ovarian pathways to pelvic epithelial cancer: a pathological perspective. Histopathology. 2008;53:127–38.
Bell DA, Scully RE. Early de novo ovarian carcinoma. A study of fourteen cases. Cancer. 1994;73:1859–64.
Werness BA, Afify AM, Bielat KL, et al. Altered surface and cyst epithelium of ovaries removed prophylactically from women with a family history of ovarian cancer. Hum Pathol. 1999;30:151–7.
Okamura H, Katabuchi H. Detailed morphology of human ovarian surface epithelium focusing on its metaplastic and neoplastic capability. Ital J Anat Embryol. 2001;106:263–76.
Okamura H, Katabuchi H. Pathophysiological dynamics of human ovarian surface epithelial cells in epithelial ovarian carcinogenesis. Int Rev Cytol. 2005;242:1–54.
Barakat RR, Federici MG, Saigo PE, et al. Absence of premalignant histologic, molecular, or cell biologic alterations in prophylactic oophorectomy specimens from BRCA1 heterozygotes. Cancer. 2000;89:383–90.
Seidman JD, Wang BG. Evaluation of normal-sized ovaries associated with primary peritoneal serous carcinoma for possible precursors of ovarian serous carcinoma. Gynecol Oncol. 2007;106:201–6.
Sherman ME, Lee JS, Burks RT, et al. Histopathologic features of ovaries at increased risk for carcinoma. A case–control analysis. Int J Gynecol Pathol. 1999;18:151–7.
Stratton JF, Buckley CH, Lowe D, et al. Comparison of prophylactic oophorectomy specimens from carriers and noncarriers of a BRCA1 or BRCA2 gene mutation. United Kingdom Coordinating Committee on Cancer Research (UKCCCR) Familial Ovarian Cancer Study Group. J Natl Cancer Inst. 1999;91:626–8.
Chene G, Penault-Llorca F, Le Bouedec G, et al. Ovarian epithelial dysplasia after ovulation induction: time and dose effects. Hum Reprod. 2009;24:132–8.
Deligdisch L, Einstein AJ, Guera D, et al. Ovarian dysplasia in epithelial inclusion cysts A morphometric approach using neural networks. Cancer. 1995;76:1027–34.
Pothuri B, Leitao MM, Levine DA et al. Genetic analysis of the early natural history of epithelial ovarian carcinoma. PLoS One;5:e10358.
Acknowledgments
This study is supported by the US Department of Defense CDMRP Ovarian Consortium grant OC100517.
Disclosure
No potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kuhn, E., Kurman, R.J. & Shih, IM. Ovarian Cancer is an Imported Disease: Fact or Fiction?. Curr Obstet Gynecol Rep 1, 1–9 (2012). https://doi.org/10.1007/s13669-011-0004-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13669-011-0004-1