
Abstract
Skeletal muscle regeneration is the process that ensures tissue repair after damage by injury or in degenerative diseases such as muscular dystrophy. Satellite cells, the adult skeletal muscle progenitor cells, are commonly considered to be the main cell type involved in skeletal muscle regeneration. Their mechanism of action in this process is extensively characterized. However, evidence accumulated in the last decade suggests that other cell types may participate in skeletal muscle regeneration. Although their actual contribution to muscle formation and regeneration is still not clear; if properly manipulated, these cells may become new suitable and powerful sources for cell therapy of skeletal muscle degenerative diseases. Mesoangioblasts, vessel associated stem/progenitor cells with high proliferative, migratory and myogenic potential, are very good candidates for clinical applications and are already in clinical experimentation. In addition, pluripotent stem cells are very promising sources for regeneration of most tissues, including skeletal muscle. Conditions such as muscle cachexia or aging that severely alter homeostasis may be counteracted by transplantation of donor and/or recruitment and activation of resident muscle stem/progenitor cells. Advantages and limitations of different cell therapy approaches will be discussed.
Similar content being viewed by others


1 Introduction
Skeletal muscle regeneration only occurs upon damage or stress conditions (as intense physical exercise), when satellite cells (SCs) become activated and proliferate to eventually repair or replace the damaged or dead muscle fibers. However, if compared to other cell types, such as fibroblasts, SCs proliferation capability is relatively limited. In fact, if fiber degeneration is caused by a major trauma or by a chronic degenerative disease, SCs are not able to sustain regeneration of the damaged area and the lack of new fibers is eventually replaced by fibroblasts that form scar tissue. The inability of the skeletal muscle tissue to be properly repaired under severe degenerative conditions has led many laboratory groups to search for alternative cell sources for effective regeneration. Many cell types, other than SCs, and located in different compartments, show myogenic potential in vitro and upon transplantation [reviewed in 1, 2]. Their natural contribution to skeletal muscle regeneration is still questionable and when found in vivo [3] it was shown to occur at much lower frequency than SCs. Nevertheless, myogenic potential of some of these cells in certain experimental conditions is remarkable and makes them potentially useful for cell therapy of muscle degenerative diseases. These cell types include: mesoangioblasts (MABs), CD133+ (also known as AC133+) cells, muscle interstitial cells (PICs), endothelial progenitor cells, side population stem cells, hematopoietic stem cells, mesenchimal stem cells, multipotent adult progenitor cells, and adipose-derived stem cells.
A further possibility for production of cells for tissue repair is the use of pluripotent stem cells, which are, by definition, able to give rise to cell types of all the three germ layers (ectoderm, mesoderm, and endoderm), and could represent a virtual unlimited source of skeletal muscle cells as well as most of the other cell types of the body. Because of their remarkable properties, these cells could be potentially used to treat most of the degenerative diseases. In particular, studies of skeletal muscle derivation and transplantation gave encouraging results opening new therapeutic perspectives for muscle degenerative diseases [2, 4, 5].
There exist more than a hundred of skeletal muscle diseases and many of them involve fiber degeneration mechanisms. The majority is included in the category of muscular dystrophies, characterized by a primary genetic defect of skeletal muscle leading to different degrees of muscle wasting and consequent movement disability. In most of the cases, the disease is caused by a mutation affecting proteins directly involved in the maintenance of the myofiber architectural structure. The Duchenne muscular dystrophy (DMD), the most severe myopathy of its category, is caused by a particular mutation in the Dystrophin gene that results in the total lack of the protein, leading to alteration of the muscle integrity and increased susceptibility to contraction-induced damage. One major hurdle to the treatment of genetic muscle diseases (except than the few forms localized to certain muscles only) is represented by the abundance of skeletal muscle [6]. The correction of the genetic defect should occur in most muscle fibers to be beneficial. Any approach based on local treatment but in need to be extended to the whole body muscle mass would be clinically difficult to perform. Therefore, beside pharmacological and viral gene therapy, the use of cells that can reach the target tissue through the circulation appears a realistic approach for an effective treatment.
In aging and in conditions of muscle wasting associated to pathologies as cancer, AIDS and chronic heart failure, the damaged muscle is also not repaired and mechanisms of block of muscle regeneration and stem cell recruitment contributes to reduction in muscle fiber size. Chronic muscle atrophy is indeed caused by loss and dysfunction of muscle precursor cells that can be considered as targets for the treatment of cachexia.
In this review, we will discuss some of the most characterized muscle precursors, their use and potentiality in cell therapy approaches of neuromuscular degenerative diseases and muscle wasting conditions.
2 Muscle satellite cells
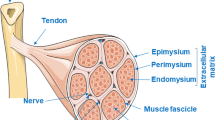
SCs of skeletal muscle were originally defined by their anatomical location, beneath the basal lamina and the sarcolemma, flanking each mature skeletal muscle fiber (Fig 1). In normal physiological conditions, SCs in adult skeletal muscle are in quiescent state. Upon damage or muscle exercise, they become activated, start proliferating and terminally differentiate to regenerate the damaged muscle. SCs are able to fuse with both the existing damaged fibers and with each other to form de novo fibers. Once activated, a subset of SCs returns to the original niche, the basal lamina, thus providing a constant source for their self-renewal [7, 8]. Electron microscopy, thymidine labeling, and, more recently, lineage tracing studies indicated that they also participate in skeletal muscle growth [9]. In normal healthy conditions, SCs are a small percentage of the total amount of nuclei within the neighboring fibers, although with certain variability in specific muscles [10, 11]. Despite severe skeletal muscle, degenerative myopathies lead to muscle wasting and inability to be naturally regenerated over time; SC proliferative and regenerative potential in response to damage in these conditions is extremely high [12]. Wide studies have been made on their capability to proliferate, differentiate, efficiently regenerate skeletal muscle, reviewed in [13, 14], and, very importantly, to self-renew, maintaining the SC compartment even under many cycles of regeneration [15, 16].

Skeletal muscle cross-section including haematoxylin-eosin stained muscle fibers and a blood capillary running longitudinally along the section (arrow). The image shows the localization of the main skeletal muscle precursor cells as satellite cells, mesoangioblasts (MABs), muscle interstitial cells (PICs), fibro-adipogenic precursors (FAPs) and hematopoietic stem cells (see the legend on the right)
Because of their natural function, SCs were the first candidate for a cell therapy approach. In the past, it was demonstrated that wild-type SCs injected into a mouse with dystrophic phenotype (mdx), are able to fuse with the recipient fibers and restore production of the lacking protein [17]. Unfortunately, clinical trials that followed this model failed, mostly because of inefficiency in different steps of the clinical procedure [reviewed in 18]. More recent studies showed that transplantation of single muscle fibers strongly increases the number of entire muscle fibers newly formed that also are able to regenerate upon de novo damage induction [19], although clinical translation of this experimental approach does not appear simple.
Quiescent and proliferating SCs express several specific markers that allow prospective isolation of partially purified populations for characterization and clinical application. These include transcription factors Myf-5, Pax7, or Pax3 [14] and surface markers such as CD34, M-cadherin, c-MET, CD56, although these last are not specific for SCs and show a certain rate of variability among different species [reviewed in 1]. In the last years, different groups have isolated SC populations using different surface marker combinations [20–22] and showed that these selected populations have much higher potency to regenerate skeletal muscle if transplanted after fresh isolation than after in vitro expansion, suggesting that important signals for maintenance of appropriate proliferation and regeneration potency are progressively lost when the cells are placed in culture. New approaches, that recapitulate bioengineered skeletal muscle niche, demonstrate that a substrate stiffness similar to muscle tissue dramatically improves the self-renewal and engraftment potential of SCs in comparison with plastic [23]. All these results are promising from a therapeutic perspective and a large amount of work has been addressed to solve most of the problems involved in the use of SCs in correction of dystrophy in DMD patients through intramuscular SCs injections, as immunoresponse and poor survival of SCs rapidly after the injection [reviewed in 18]. Nevertheless, a phase I clinical trial by intramuscular SCs transplantation has been completed with modest improvement in treated patients. The major limitation of this method is that even with different injections in different muscles, the transplantation does not achieve a general effect, due to the poor survival to transplantation and limited migratory capability of SCs. Importantly, they are not able to cross the vessel walls [24, 25]. This is a major hurdle to the possibility of use of SCs for an effective cell therapy treatment through systemic delivery [26].
3 Nonsatellite cell muscle precursors
3.1 Muscle interstitial cells
Other than under the basal lamina, cells with myogenic potential have been found in the interstitial space between the muscle fibers. These nonsatellite muscle resident progenitor cells are named PICs (Pw1+ interstitial cells), on the basis of their localization (Fig. 1) and the expression of the zinc finger protein Pw1, an early marker of the myogenic lineage [27]. Differently from the SCs, in a quiescent state they do not express any other marker of the myogenic lineage, such as Pax7. Upon isolation and differentiation, they express the myogenic markers and fuse into myotubes in vitro at the same extent of SCs. They contribute to muscle growth since their number diminishes with muscle maturation, similar to SCs, concur to regeneration and are a source of both SCs and PICs in vivo. Contrarily to SCs that need Pax7 to proliferate, PICs accumulate enormously in Pax7−/− mice. Nevertheless, they need Pax7 to differentiate since PICs derived from Pax7−/− mice are not able to become myogenic in vitro, indicating Pax7 as a myogenic determinant of PICs. Elegant studies aimed to the definition of the PICs’ lineage in embryos demonstrated that SCs and PICs have a distinct origin, and that PICs are not derived from SCs but they are able to originate SCs and PICs. This indicates a higher position of PICs respect to SCs in the muscle precursor lineage hierarchy [28]. PICs are not the only muscle precursor found in the interstitial space. Recently, a population of cells with a myogenic potential have been described in this compartment and is vessel associated. It still has to be assessed if they are different from the PICs population. They express the β4 integrin marker and no other myogenic marker in the quiescent state. When activated, they differentiate in myotubes in vitro and participate to regeneration of damaged muscle [29]. For their properties, including the ability of self-renewing, PICs and other interstitial cells are a new promising candidate for the cell therapy of muscular pathologies.
3.2 Hematopoietic stem cells
Almost 15 years ago, the presence of progenitors with myogenic potential was described in bone marrow [30], suggesting the exciting possibility that muscle degenerative diseases could be treated by bone marrow transplantation. Transplantation of bone marrow-derived cells and side population progenitor enriched fraction results in cell recruitment to an injured muscle and participation to muscle repair [31–33]. The limiting aspect of this approach is the low frequency of engraftment, even when a subpopulation of hematopoietic cells with myogenic potential, CD45+, was used for transplantation in a DMD patient with hematologic disease [33, 34].
Later, a subset of hematopoietic stem cells expressing the CD133 marker and early myogenic markers as Myf-5, Pax7, and M-cadherin, AC133+ cells, were isolated and injected into the circulation of scid/mdx mice, were concurred to muscle repair and also to a recovery of force compared to the normal mice [35]. CD133+ cells were also isolated both from blood and muscle compartments from dystrophic mice and were genetically corrected by lentiviral vectors expressing small nuclear RNA engineered to cause exon skipping in order to correct the dystrophin gene and have been found to be efficient in the functional recovery of the dystrophic phenotype of scid/mdx mice [36]. Muscle-derived cells showed an increased ability to restore skeletal muscle function in dystrophic murine model, compared to the blood-derived cells. For an efficient application of these cells in a transplantation strategy, it is crucial to explore why the blood-derived cells lack an efficient in vivo engraftment and try to improve it. In 2007, the first encouraging results of a double-blind phase I clinical trial with the use of the AC133+ cells in an 8-year-old dystrophic boy were published and demonstrated that the intramuscular transplantation of muscle-derived AC133+ cells in DMD patients was a safe and feasible procedure. Indeed, the patients showed an increased number of capillaries and a change in the ratio slow/fast myosin myofibers which likely reflected paracrine effects of transplanted cells [37].
3.3 Mesoangioblasts
The identification of myogenic progenitors in the embryonic dorsal aorta [38] and later quail chick and mouse chick transplantation experiments led to the identification and definition of MABs, multipotent vessel-associated progenitors located in the aorta–gonad–mesonephros region in mouse (Fig. 1). MABs can be propagated in vitro for several passages while retaining the ability to differentiate into several cell types of mesoderm when under specific experimental conditions [39, 40]. Gene expression analysis on early clonally expanded MABs before the first culture passage confirmed the expression of almost all the markers reported after long-term culture (Sirabella et al., unpublished observations), indicating consistency of their molecular signature over time and suggesting that artificial culture growth conditions do not alter their properties. MABs resemble mesenchymal stem cells for biological properties but differ from them for the expression of some antigens such as CD34. In addition, as for most but not all the typical MAB markers, CD34 expression is strongly maintained at any culture passage and consistently found in all the generations of MAB clonal lines (Sirabella et al., unpublished observations).
Cells suggested to be the progeny of embryonic MABs because of their position and biological properties, can be isolated from postnatal vessels [40, 41]. Adult MABs express pericyte markers such as NG2 and alkaline phosphatase [40].
Preclinical transplantation studies with postnatal MABs in animal models showed very encouraging results. These cells were able to partially recover muscle morphology and function in a mouse model of limb–girdle muscular dystrophy (α-sarcoglycan null), not only in local areas after intramuscular injection but, most importantly, after delivery through arterial circulation. When genetically corrected, similarly to their embryonic wild-type counterpart, MABs from juvenile α-sarcoglycan-null mice are able to restore skeletal muscle after autologous transplantation [41]. Further studies showed that MABs can also improve muscle activity of dystrophic dogs, which are the closest animal model to the human DMD genotype and phenotype. However, in dogs, recovery of muscular activity occurs upon transplantation of heterologous but not autologous genetically corrected cells [42].
Similar cells are present in the pericyte compartment of human postnatal vessels and typically express pericyte markers such as alkaline phosphatase and NG2 but do not express endothelial markers such as CD31 and CD34 [43]. They neither show the embryonic MAB marker profile nor the SCs one, but spontaneously differentiate into skeletal muscle fiber, representing a myogenic cell type distinct from SCs. Remarkably, these cells can be easily isolated from muscle biopsies, expanded in vitro with high efficiency and transplanted trough systemic delivery into recipient animals that model muscular dystrophy, where they efficiently participate in skeletal muscle regeneration. All these features make them an ideal candidate cell type for clinical applications of skeletal muscle myopathies. Currently, a phase I/II clinical trial with transplantation of these cells in DMD patients is in progress at the San Raffaele Hospital in Milan, Italy. Very recently, an amelioration of the dystrophic phenotype in mdx mice using MABs engineered with a human artificial chromosome carrying the entire human dystrophin genetic locus has been described and this fascinating approach has been proposed for future clinical translation [44].
Studies of human MABs in other muscle diseases, as inflammatory myopathies and facioscapulohumeral muscular dystrophy, are also ongoing [44, 45]. Postnatal MABs isolated from biopsies of inclusion body myositis (IBM) patients, differently from the ones isolated from patients with dermatomyositis and polymyositis, are deficient in myogenic differentiation while SC-derived myoblasts from the same patients display normal skeletal muscle differentiation in vitro [46]. This suggests that MABs may have a direct role in IBM pathogenesis. Transient exogenous induction of MyoD expression in MABs from IBM patients rescues their myogenic potency [47]. Gene expression analysis revealed that IBM MABs, with respect to healthy control cells, have increased expression of TGFβ (transforming growth factor beta), soluble frizzled receptor protein, and basic helix loop helix B3. All these molecules have been shown to be negative myogenesis regulators and therefore are likely to be responsible for this effect [46, 47]. More recently, it has been found that guanine nucleotide exchange factor, previously shown to play a role in skeletal muscle regeneration [48], is downregulated in IBM MABs and its overexpression partially rescues their myogenic differentiation capability both in vitro and in vivo [47]. Pharmacological treatments with drugs targeting the molecules directly implicated in the pathogenesis of the disease would be a much easier approach rather than cell transplantation [49].
Interestingly, MABs are also found in the juvenile vessel of cardiac ventricle in mouse [50]. They show high spontaneous cardiac differentiation and efficiently regenerate heart when injected into the ventricle of an infarcted heart. This is consistent with previous studies that showed the ability of embryonic MABs to repair infarcted myocardia [51]. Importantly, cardiac MABs are also present in human. Remarkably, cardiopathic conditions in human are mirrored by impaired activity of cardiac MABs isolated from the patients [52], suggesting that they may be a physiological player in heart homeostasis and repair. Some muscular dystrophies, including the most sever ones, beside skeletal muscle wasting, lead to impairment or eventually failure of the cardiac muscle. Therefore, cardiac MABs arise as a promising candidate for cell therapies directed towards both regeneration of infarcted hearts and primary skeletal myopathies.
4 Muscle from fat
Adipose tissue (AT) is composed of mature adipocytes embedded in a framework of collagene and is a source of adipose precursors of different rate of differentiation, included in the stromal vascular fraction (SVF). AT-derived vascular cells can differentiate in vitro in myogenic cells by an artificial inductive media and also in other nonmesenchymal lineages [53–55]. Subpopulations of AT–SVF derived from inguinal or visceral fat can differentiate in myotubes by a fusion-independent cell-autonomous mechanism when cultured in the presence of primary myoblasts. They require either a cell contact with myoblasts or need to be exposed to the soluble factors secreted by muscle cells. However, a rare subset spontaneously differentiates into skeletal muscle. Indeed, murine and human AT–SVF cells (referred as human mesenchymal adipose-derived stem cells) significantly participate in muscle regeneration in vivo and can restore dystrophin expression in mdx mice [56, 57]. More recently, it has been shown how under forced expression of MYOD their capability to repair dystrophic muscle was increased while their adipogenic differentiation was inhibited [58]. An expansion of AT cells within skeletal muscle observed in response to denervation [59], in sarcopenia [60] and in muscular dystrophy [18], with myogenic differentiation potential of adipogenic stem cell, demonstrated in vitro and in vivo, make them a potential alternative tool for repairing damaged muscle fibers. Moreover, the immunosuppressive properties of adipose stem cells [61, 62] increase the feasibility of transplantation procedures in damaged muscle, representing an important advantage in a clinical therapy perspective.
Interaction between muscle and adipose tissue are interestingly significant, especially in pathologic conditions as muscular dystrophy where regeneration is impaired and a fibrotic scar infiltrated with adipocytes occurs, known as fatty degeneration. It has been proposed that the damaged environment has influence on the myogenic fate of SCs that are forced to adopt a fat fate [63, 64]. Recently, two groups [65, 66] isolated a population of cells, fibro-adipogenic progenitors (FAPs), Sca1, CD34, and PDGFRa positive, abundant as SCs in muscle tissue, capable of generating both adipocytes and myofibroblasts in vitro, which do not differentiate in myoblasts in vitro or in vivo. FAPs are located in the interstitial space between the myofibers, lying adjacent to the external side of the blood vessel basement membrane (Fig 1). Via direct cell–cell contact, adipogenic progenitors are a source of prodifferentiation factors and have an accessory function for myogenic cells during muscle regeneration. Furthermore, FAP fate responds to the efficiency of regeneration in a way that when the muscle fibers are regenerating FAPs are ablated from the tissue. On the contrary, when a fatty degeneration occurs, FAPs differentiate in adipocytes with a consequent increase of FAP engraftment. Therefore, FAPs play a dual role in the contest of muscle damage, contributing to muscle degeneration by differentiating in fibroblasts and adipose cells and participating to muscle regeneration by production of prodifferentiation signals [65–67]. The discovery of this dual-function cell type in the muscle compartment highlights the importance of the stem cell niche and how it influences the regenerative fate of the muscle precursor cells.
5 Reprogramming for skeletal muscle derivation
Examples of noncanonical myogenic progenitors above reported reveal that mesoderm progenitor heterogeneity is higher than what believed in the past and involves a certain degree of plasticity. It is generally accepted now that cellular commitment of a specific cell type to a certain differentiation fate can be altered when specific regulatory mechanisms, as expression of certain transcription factors or chromatin remodeling processes, are modified to some extent. By environmental or genetic manipulation, many cell types can undergo switch of their commitment state or differentiation fate, hence can be reprogrammed. Skeletal muscle holds a very early example of cellular reprogramming: it has been demonstrated that primary fibroblasts can be converted to skeletal muscle cells simply by exogenous expression of the gene MyoD [68], later widely investigated and defined as a master regulator of the myogenic program. Recently, the use of novel technology as high throughput sequencing combined with chromatin immunoprecipitation revealed that MyoD has a high spectrum of interaction and the ability to widely modify the chromatin state [69]. Other observations reveal that even small molecules can deeply affect the commitment state of a cell type. For example, it has been recently shown that a synthesized molecule, named reversine is able to change the differentiation program of fibroblasts, reverting them to a multipotent state, hereby making them able to differentiate into different cell types under specific conditions [70]. Similarly, the ability of mesodermal stem/progenitor cells to undergo “unorthodox” differentiation is a process that can be activated under certain environmental natural or artificial conditions. However, it is not clearly defined if this process occurs because these cells are intrinsically multipotent or rather in a committed unipotent state yet reprogrammed under those conditions.
Embryonic stem cells (ESCs) are typically the most “uncommitted” stem cell type experimentally available, able to give rise to all the cell types of the body, hence defined as pluripotent. Along the last 30 years, starting from the first study on ESCs isolated from mouse [71], very extensive studies have been made. Human ESCs, although partially regulated by quite different molecular mechanisms respect to the mouse ESCs, equally display high proliferative potential and spectrum of differentiation, holding major promises for clinical applications. Important recent studies demonstrated controllable commitment and differentiation of ESCs into skeletal muscle [4, 5] (Table 1). Quite surprisingly, in vivo skeletal muscle differentiation upon ESC transplantation does not form teratomas [2], a very important advantage for therapeutic perspectives. In general, ESC robust capacity of both self renewal and differentiation in cell types of all tissues make them a major candidate for clinical therapies of a wide range of degenerative diseases. However, the use of ESCs is hindered by ethical concerns because human embryos are required for their derivation. In addition, autologous cell therapies are prevented and consequently any therapy with these cell types would require treatment with immunosuppressive drugs. These obstacles can be apparently overcome after a recent revolutionary discovery in the stem cell field: in 2006, the research group led by Yamanaka demonstrated that by the exogenous activation of four specific transcription factors, Oct3/4, Sox2, Klf4, and cMyc, a committed cell type can be fully reprogrammed to a pluripotent state [72], reaching the primordial stem state of ESCs. The stem cells generated are named induced pluripotent stem cells (iPSCs). The result, first obtained in mouse fibroblasts, was soon confirmed in humans [73]. From a therapeutic perspective, the use of iPSCs would resolve the ethical concerns and gives rise to the possibility of autologous cell transplantation. In addition, the derivation of patient-specific iPSCs opens the possibility of disease modeling with in vitro recapitulation of specific pathologies and the use of the same models for drug screening.
A major concern in the use of iPSCs for clinical transplantation purposes is that most of the methods for their generation require genetic modification that results in random integration of the exogenous sequences, with the added inconvenience that two of the four exogenous genes normally used are oncogenic: Klf4 and, more strongly, cMyc. Since the first technique using the pMx retroviral vector, intensive biotechnological studies led to modifications and improvements in the generation of iPSCs. For example, the use of retroviral delivery with the exclusion of cMyc resulted in significant decrease of tumor formation upon iPSC transplantation [74]. Other methods lately developed are the use of virus vector-free iPSC generation with repeated transfection of plasmids carrying the same original transcription factors [75] or direct delivery of recombinant proteins [76, 77]. A theoretically safer virus-mediated efficient alternative method established is the use of the Cre-recombinase excisable viral vector [78].
Remarkably, it has been shown that it is possible to generate iPSCs from many different cell types other than fibroblasts, as B lymphocytes [79], pancreatic cells [80], neural stem cells [81] from mouse and keratinocytes [82] and blood progenitor cells [83] from human, indicating that the barrier to reprogramming has very similar extent even in very different committed cell types. Interestingly, a recent study showed that generation of iPSCs from muscle satellite and stem cells can be obtained with high efficiency, comparable to the ones from mesenchymal stem cells and also much higher than from committed fibroblasts from the same niche [84].
Similarly to ESCs, skeletal muscle can be derived from iPSCs (Table 1). In pathological conditions where the muscle precursors are poor and inefficient, derivation of iPSCs from cell types of other compartments converted in muscle precursors can be a powerful strategy to generate muscle precursors for cell therapy.
Recently, two elegant studies showed the potential of iPSCs in therapeutic application for the cure of muscular dystrophies. Indeed, the group of Perlingeiro showed that hESCs or hiPSCs under a conditional expression of Pax7 produce a large amount of muscle precursors that engraft efficiently in dystrophic muscle and restore α-dystrophin expression and fiber functionality [85]. Furthermore, Cossu’s group showed that iPSCs derived from myoblasts and fibroblasts of patients affected by a limb–girdle muscular dystrophy 2D, caused by the loss of the α-sarcoglican protein, were reprogrammed to differentiate into MABs. After genetic correction with the α-sarcoglican human gene, the MABs obtained were transplanted in sarcoglican-null immunodeficient mice where they were able to ameliorate the muscle functionality and to supply the muscle progenitor cell pool [86].
Unexpectedly, we have observed that primary skeletal myoblasts reprogrammed to pluripotency can lead to spontaneous embryoid body-derived cardiac differentiation [Sirabella et al., unpublished data]. Our data were soon confirmed by another group that furthermore demonstrated the ability of those myoblast-derived cardiac cells to improve the function of a mouse infarcted heart after transplantation without tumor formation [87] indicating skeletal muscle cell source combined with the reprogramming technology as a possible novel therapeutic approach for myocardial repair.
6 Muscle progenitors in a therapeutic perspective for muscle wasting
Other than in repair of damaged muscle, muscle stem cells play a remarkable role in the postnatal growth and maintenance of the body muscle mass in the adult. As described above, in a normal physiological state, SCs reside quiescent on the myofibers. However, their proliferative and myogenic potency change in developing muscle. In fact, at birth, they are 30 % of myonuclei in the muscle and in the first weeks of life, they actively proliferate to fuse into the myofibers and contribute to muscle mass increase. Moreover, their properties are modified in conditions of hypertrophic and atrophic muscle and in old ages. On the role of activation/proliferation and fusion of SCs in hypertrophic muscle, there are several contrasting theories [reviewed in 88] that will not be discussed in this review. We will instead discuss the involvement of muscle progenitors in atrophy and aging.
Muscle atrophy is induced under different conditions as denervation, disuse, starvation, and unloading. It is also a complication of several pathologies ranging from cancer to cardiac failure, AIDS or rheumatoid arthritis (cachexia), and neuromuscular disorders; it also occurs in physiological processes such as aging (sarcopenia). Growth and repair of atrophied muscle mainly depends on muscle precursor cells. Several studies were accomplished on the effects of the atrophic stimuli on muscle precursors cells, in particular SCs. Apoptosis was considered the main cause of depletion of SCs after denervation [89], immobilization [90] and in a model of CHF [91]. Aging also causes a major susceptibility of SCs to apoptosis [92].
The hypothesis that muscle atrophy is accompanied by apoptotic loss of myonuclei and recovering would require recruiting of muscle precursor cells is currently debated. By time-lapse microscopy in vivo, the group of Gundersen demonstrated that after denervation or mechanical unloading, no loss of myonuclei was observed while myofiber cross-sectional area was reduced of 50 %. Nevertheless, apoptosis was confirmed in muscle of old mice and in SCs [93, 94].
Many evidences link muscle wasting induced by cachexia and failure in regeneration mediated by muscle precursors. Muscle regeneration is indeed affected by inflammatory signals induced locally by damage and systemically in cachexia. TNF-a, IL-6, and other cytochines, which induce cachexia, inhibit myogenic differentiation in vitro and muscle regeneration [95–99]. Moreover, muscle precursor cells are reduced and nonfunctional in prolonged atrophied muscle after limb suspension and these effects are reversed after reloading [100]. It is possible that the prolonged blockage of muscle differentiation or stem cell recruitment lead to muscle atrophy.
Aging is a physiological condition accompanied by a muscle mass loss (sarcopenia), widely considered also dependent by the modified properties of muscle precursors which lead to reduced capacity of proliferation, regeneration, and generation of reserve population [101–103]. However, studies of heterochronic tissue transplants and parabiosis demonstrated that the environment is crucial for determining the efficiency in SC activation. Indeed, muscle autografted in young host regenerate better than when autografted in an old host [104] and heterochronic parabioses, young and old mice sharing the circulatory system, restore the regenerative capacity of old SCs [105]. A molecular mechanism has been proposed to explain the stem cell aging in old mice and the restoration of muscle precursor regenerative capacity by young mice circulating factors: satellite cell activation and determination are controlled by the Notch signaling pathway, which is initiated by the increased expression level of the Notch ligand, Delta; in old mice, Delta expression is impaired and satellite cell activation is reduced. When in heterochronic parabioses, the aged SCs are exposed to factors from young mice, their response is reactivated [106]. Decline of regenerative potential of SCs with age is also caused by their conversion from a myogenic to a fibrogenic lineage. Activation of the canonical Wnt pathway is responsible of this conversion and in aged mice serum factors bind the frizzled family of protein that are Wnt receptors, accounting for the activation of the Wnt pathway in aged muscle [107]. Further investigation on the molecular mechanisms responsible for the decreased regenerative potential of SCs in old mice have proposed that elevated levels of TGFβ-1 and pSmad-3 in the serum affect regenerative competence through activation of cyclin-dependent kinases. Inhibition of this pathway restores the regenerative potential of SCs in old mice [108, 109]. Overall, these results show that the muscle precursors do not lose their capacity to repair muscle during aging and the environmental factors are crucial for maintaining an efficient regenerative response [107, 110]. Aged muscle stem cell niche also influences the quiescent state and self-renewing capacity of SC. It has been newly shown that in aged muscle fibers the increased FGF signaling leads to loss of SC quiescence and regenerative function. Indeed, the modulation of Sprouty, an inhibitor of the FGF signaling, alters SC quiescence, self-renewal, and regenerative capacity [111]. Even the negative regulators of muscle mass, such as myostatin, which exert a role in inhibiting SC activation and muscle regeneration in postnatal life, affect regenerative potential of muscle precursors in aging. In mice lacking myostatin, it has been observed a reduction of the age-related sarcopenia and an increase of muscle regenerative capacity [112]. Moreover, blockade of myostatin by antagonist restore the regenerative capacity of SCs in sarcopenia [113]. More recently, an increase of myostatin positive SCs associated to type II fiber has been observed in human old males, which suggest a role of myostatin for the impaired myogenic capacity of aged muscle [114].
7 Conclusions
Skeletal muscle tissue repair in physiologic and pathologic conditions, such as aging and diseases, is exerted by muscle precursor cells. For this reason and because of the successful attempts to treat diverse diseases through the adult stem cell therapy, the field of muscle stem cells is lately expanding more and more. While SCs are the canonical and the most characterized muscle stem cells, their properties do not allow considering them as the best candidate for cell therapy of muscle tissue disorders. Other populations of muscle stem cells, instead, have several characteristics suggesting successful perspectives for cell-therapy based approaches to contrast muscular diseases. On the other hand, the role of the other muscle progenitors in postnatal myogenesis and regeneration has not been completely assessed. In fact, recent studies demonstrated that when in murine models the SC compartment is selectively ablated, muscle regeneration following injury is compromised, indicating that other muscle progenitors can’t account for muscle repair in physiological conditions. These limitations can be explained by the intriguing hypothesis that SCs recruit and activate the other muscle progenitors by physical and molecular interactions and commit them to the myogenic lineage [115–117 and reviewed in 118], suggesting that dissecting the mechanisms of those interactions may be important for cell therapy approaches that involve more than one muscle stem cell population.
It is possible to imagine future therapies for atrophy related pathologies and conditions based on transplantation of autologous SCs or induced muscle stem cells. Understanding the molecular mechanisms that regulate muscle precursor efficiency in regeneration and repair may be crucial for the development of strategies to ameliorate atrophy in conditions of aging and disease.
However, the decline of activity of muscle precursor cells in cachexia and aging could depend on the systemic environment, which makes the cell transplantation approach not a suitable system. Further studies on the interactions that lead to create adverse environment could help to find the pharmaceutical targets that can ameliorate the conditions for a stem cell mediated therapy of muscle wasting.
No studies have been conducted so far on the effects of atrophy and aging on muscle precursors other than SCs. This may become an extremely interesting field considering different properties that would make them more effective in a cell-based therapy of muscle wasting conditions.
In principle, the possibility to reprogram all the cells of the body to muscle represents a revolutionary concept, tremendously widening the range of muscle sources for the treatment of muscle dysfunctions. To date, different studies of skeletal muscle derivation from pluripotent stem cells have been done (Table 1). The interest in this field is growing exponentially and very likely many new studies will follow in the near future. Since the discovery of the iPSCs, the network of pathways implicated in the reprogramming and maintenance of pluripotency has been extensively studied. Despite not yet completely unraveled at molecular level, the biological properties of iPSCs result to be extremely similar to the ones of ESCs. The propelling results obtained with the latter in regeneration models can apparently be confirmed with the former. This makes iPSCs a very promising candidate in autologous transplantation for tissue repair or replacement including genetic disease therapy after correction of the genetic defects. We predict that in the near future clinical trials with iPSCs or iPSC-derived cells will be started and very likely in vitro drug screening on specific disease-derived iPSCs will have a significant impact on pharmacological therapy.
References
Tedesco FS, Dellavalle A, Diaz-Manera J, Messina G, Cossu G. Repairing skeletal muscle: regenerative potential of skeletal muscle cells. J Clin Invest. 2012;120:11–9.
Bhagavati S, Xu W. Generation of skeletal muscle from transplanted embryonic stem cells in dystrophic mice. Biochem Biophys Res Commun. 2005;333:644–9.
Dellavalle A, Maroli G, Covarello D, Azzoni E, Innocenzi A, Perani L, et al. Pericytes resident in postnatal skeletal muscle differentiate into muscle fibres and generate satellite cells. Nat Commun. 2011;2:499.
Barberi T, Bradbury M, Dincer Z, Panagiotakos G, Socci ND, Studer L. Derivation of engraftable skeletal myoblasts from human embryonic stem cells. Nat Med. 2007;13:642–8.
Sakurai H, Inami Y, Tamamura Y, Yoshikai T, Sehara-Fujisawa A, Isobe K. Bidirectional induction toward paraxial mesodermal derivatives from mouse ES cells in chemically defined medium. Stem Cell Res. 2009;3:157–69.
Cossu G, Sampaolesi M. New therapies for muscular dystrophy cautions optimism. Trends Mol Med. 2004;10:516–20.
Mauro A. Satellite cells of skeletal muscle fibers. J Biophys Biochem Cytol. 1961;9:493–5.
Reznik M. Origin of myoblast during skeletal muscle regeneration. Electron microscopic observations. Lab Invest. 1969;20:353–63.
Holterman CE, Rudnicki MA. Molecular regulation of satellite cell function. Semin Cell Dev Biol. 2005;16:575–84.
Allbrook DB, Han MF, Hellmuth AE. Population of muscle satellite cells in relation to age and mitotic activity. Pathology. 1971;3:223–43.
Schultz E. A quantitative study of the satellite cell population in postnatal mouse lumbrical muscle. Anat Rec. 1974;180:589–95.
Zammit PS, Heslop L, Hudon V, Rosenblatt JD, Tajbakhsh S, Buckingham ME, et al. Kinetics of myoblast proliferation show that resident cells are competent to fully regenerate skeletal muscle fibers. Exp Cell Res. 2002;281:39–49.
Shadrach JL, Wagers AJ. Stem cells for skeletal muscle repair. Philos Trans R Soc Lond B Biol Sci. 2011;366:2297–306.
Biressi S, Rando TA. Heterogeneity in the muscle satellite cell population. Semin Cell Dev Biol. 2010;21:845–54.
Moss FP, Leblond CP. Satellite cells as the source of nuclei in muscles of growing rats. Anat Rec. 1971;170:421–35.
Zammit PS, Relaix F, Nagata Y, Ruiz AP, Collins CA, Partridge TA, et al. Pax 7 and myogenin progression in skeletal muscle satellite cells. J Cell Sci. 2006;119:1824–32.
Partridge TA, Morgan JE, Coulton GR, Hoffman EP, Kunkel LM. Conversion of mdx myofibres from dystrophin-negative to positive by injection of normal myoblasts. Nature. 1989;337:176–9.
Cossu G, Sampaolesi M. New therapies for Duchenne muscular dystrophy: challenges, prospects and clinical trials. Trends Mol Med. 2007;13:520–6.
Collins CA, Olsen I, Zammit PS, Heslop L, Petrie A, Partridge TA, et al. Stem cell function, self-renewal, and behavioral heterogeneity of cells from the adult muscle cell niche. Cell. 2005;122:289–301.
Cerletti M, Jurga S, Witczak CA, Hirshman MF, Shadrac JL, Goodyear LJ, et al. Highly efficient, functional engraftment of skeletal muscle stem cells in dystrophic muscles. Cell. 2008;134:37–47.
Sacco A, Doyonnas R, Kraft P, Vitotovic S, Blau HM. Self-renewal and expansion of single transplanted muscle stem cells. Nature. 2008;456:502–6.
Tanaka KK, Hall JK, Troy AA, Cornelison DD, Majka SM, Olwin BB. Syndecan-4-expressing muscle progenitor cells in the SP engraft as satellite during muscle regeneration. Cell Stem Cell. 2009;4:217–25.
Gilbert PM, Havenstrite KL, Magnuson KE, Sacco A, Leonardi NA, Kraft P, et al. Substrate elasticity regulates skeletal muscle stem cell self-renewal in culture. Science. 2010;329:1078–81.
Skuk D, Tremblay JP. Intramuscular cell transplantation as a potential treatment of myopathies: clinical and preclinical relevant data. Expert Opin Biol. 2011;11:359–74.
Palmieri B, Tremblay JP, Daniele L. Past, present and future of myoblast transplantation in the treatment of Duchenne muscular dystrophy. Pediatr Transplant. 2010;14:813–9.
Price FD, Kuroda K, Rudnicki MA. Stem cell based teraphies to treat muscular dystrophy. Biochim Biophys Acta. 2007;1772:272–83.
Relaix F, Weng X, Marazzi G, Yang E, Copeland N, Jenkins N, et al. Pw1, a novel zinc finger gene implicated in the myogenic nd neuronal lineages. Dev Biol. 1996;177:383–96.
Mitchell KJ, Pannérec A, Cadot B, Parlakian A, Besson V, Gomes ER, et al. Identification and characterization of a non-satellite cell muscle resident progenitor during muscle postnatal development. Nat Cell Biol. 2010;12:257–66.
Liadaki K, Casar JC, Wessen M, Luth ES, Jun S, Gussoni E, et al. β4 integrin marks interstitial myogenic progenitor cells in adult murine skeletal muscle. J Histochem Cytochem. 2012;60:31–44.
Ferrari G, Cusella-De Angelis G, Coletta M, Paolucci E, Stornaiuolo A, Cossu G, et al. Muscle regeneration by bone marrow-derived myogenic progenitors. Science. 1998;279:1528–30.
Gussoni E, Soneoka Y, Strickland CD, Buznev EA, Khan MK, Flint AF, et al. Dystrophin expression in the mdx mouse restored by stem cell transplantation. Nature. 1999;401:390–4.
Ferrari G, Stornaiuolo A, Mavilio F. Failure to correct muscular dystrophy. Nature. 2001;411:1014–5.
Gussoni E, Bennett RR, Muskiewicz KR, Meyerrose T, Nolta JA, Gilgoff I, et al. Long-term persistence of donor nuclei in a Duchenne muscular dystrophy patient receiving bone marrow transplantation. J Clin Invest. 2002;110:807–14.
Corbel SY, Lee A, Yi L, Duenas J, Brazelton TR, Blau HM, et al. Contribution of hematopoietic stem cells to skeletal muscle. Nat Med. 2003;9:1528–32.
Torrente Y, Belicchi M, Sampaolesi M, Pisati F, Meregalli M, D'Antona G, et al. Human circulating AC133(+) stem cells restore dystrophin expression and ameliorate function in dystrophic skeletal muscle. J Clin Invest. 2004;114:182–95.
Bencahouir R, Meregalli M, Farini A, D’Antona G, Belicchi M, Goyenvalle A, et al. Restoration of human dystrophin following transplantation of exon-skipped engineered DMD patient stem cells into dystrophic mice. Cell Stem Cell. 2007;1:646–57.
Torrente Y, Belicchi M, Marchesi C, Dantona G, Cogiamanian F, Pisati F, et al. Autologous transplantation of muscle-derived CD133+ stem cells in Duchenne muscle patients. Cell Transpant. 2007;16:563–77.
De Angelis L, Berghella L, Coletta M, Lattanzi L, Zanchi M, Cusella-De Angelis MG, et al. Skeletal myogenic progenitors originating from embryonic dorsal aorta coexpress endothelial and myogenic markers and contribute to postnatal muscle growth and regeneration. J Cell Biol. 1999;147:869–78.
Minasi MG, Riminucci M, De Angelis L, Borello U, Berarducci B, Innocenzi A, et al. The meso-angioblast: a multipotent, self-renewing cell that originates from the dorsal aorta and differentiate into most mesodermal tissue. Development. 2002;129:2773–83.
Tonlorenzi R, Dellavalle A, Schnapp E, Cossu G, Sampaolesi M. Isolation and characterization of mesoangioblasts from mouse, dog, and human tissues. Curr Protoc Stem Cell Biol. 2007; Chapter 2: Unit 2B.1.
Sampaolesi M, Torrente Y, Innocenzi A, Tonlorenzi R, D’Antona G, Pellegrino MA, et al. Cell therapy of alpha-sarcoglycan null dystrophic mice through intra-arterial delivery of mesoangioblasts. Science. 2003;301:487–92.
Sampaolesi M, Blot S, D'Antona G, Granger N, Tonlorenzi R, Innocenzi A, et al. Mesoangioblast stem cells ameliorate muscle function in dystrophic dogs. Nature. 2006;444:574–9.
Dellavalle A, Sampaolesi M, Tonlorenzi R, Tagliafico E, Sacchetti B, Perani L, et al. Pericytes of human skeletal muscle are myogenic precursors distinct from satellite cells. Nat Cell Biol. 2007;9:255–67.
Tedesco FS, Hoshiya H, D’Antona G, Gerli MF, Messina G, Antonini S, et al. Stem cell-mediated transfer of a human artificial chromosome ameliorates muscular dystrophy. Sci Transl Med;3:96ra78.
Morosetti R, Gliubizzi C, Broccolini A, Sancricca C, Mirabella M. Mesoangioblasts of inclusion-body myositis: a twofold tool to study pathogenic mechanisms and enhance defective muscle regeneration. Acta Myol. 2011;30:24–8.
Morosetti R, Gidaro T, Broccolini A, Gliubizzi C, Sancricca C, Tonali PA, et al. Mesoangioblasts from facioscapulohumeral muscular dystrophy display in vivo a variable myogenic ability predictable by their in vitro behavior. Cell Transplant. 2011;20:1299–313.
Morosetti R, Mirabella M, Gliubizzi C, Broccolini A, De Angelis L, Tagliafico E, et al. MyoD expression restores defective myogenic differentiation of human mesoangioblasts from inclusion-body myositis muscle. Proc Natl Acad Sci USA. 2006;103:16995–7000.
Charrasse S, Comunale F, Grumbach Y, Poulat F, Blangy A, Gauthier-Rouvière C. RhoA GTPase regulates M-cadherin activity and myoblast fusion. Mol Cell Biol. 2006;17:749–59.
Sancricca C, Mirabella M, Gliubizzi C, Broccolini A, Gidaro T, Morosetti R. Vessel-associated stem cells from skeletal muscle:from biology to future uses in cell therapy. World J Stem Cells. 2010;2:39–49.
Galvez BG, Sampaolesi M, Barbuti A, Crespi A, Covarello D, Brunelli S, et al. Cardiac mesoangioblasts are committed, self-renewable progenitors, associated with small vessels of juvenile mouse ventricle. Cell Death Differ. 2008;15:1417–28.
Galli D, Innocenzi A, Staszewsky L, Zanetta L, Sampaolesi M, Bai A, et al. Mesoangioblasts, vessel-associated multipotent stem cells, repair the infarcted heart by multiple cellular mechanisms: a comparison with bone marrow progenitors, fibroblasts, and endothelial cells. Arterioscler Thromb Vasc Biol. 2005;25:692–7.
Gálvez BG, Covarello D, Tolorenzi R, Brunelli S, Dellavalle A, Crippa S, et al. Human cardiac mesoangioblasts isolated from hyperthrophic cardiomyopathies are greatly reduced in proliferation and differentiation potency. Cardiovasc Res. 2009;83:707–16.
Zuk PA, Zhu M, Mizuno H, Huang J, Futrell JW, Katz AJ, et al. Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng. 2001;7:211–28.
Planat-Benard V, Silvestre JS, Cousin B, André M, Nibbelink M, Tamarat R, et al. Plasticity of human adipose lineage cells toward endothelial cells: physiological and therapeutic perspectives. Circulation. 2004;109:656–63.
Safford KM, Safford SD, Gimble JM, Shetty AK, Rice HE. Characterization of neuronal/glial differentiation of murine adipose-derived stromal cells. Exp Neurol. 2004;187:319–28.
Di Rocco G, Iachininoto MG, Tritarelli A, Straino S, Zacheo A, Germani A, et al. Myogenic potential of adipose-tissue-derived cells. J Cell Sci. 2006;119:2945–52.
Rodriguez AM, Pisani D, Dechesne CA, Turc-Carel C, Kurzenne JY, Wdziekonski B, et al. Transplantation of a multipotent cell population from human adipose tissue induces dystrophin expression in the immunocompetent mdx mouse. J Exp Med. 2005;201:1397–405.
Goudenege S, Pisani DF, Wdziekonski B, Di Santo JP, Bagnis C, Dani C, et al. Enhancement of myogenic and muscle repair capacities of human-adipose derived stem cells with forced expression of MyoD. Mol Ther. 2009;17:1064–72.
Dulor JP, Cambon B, Vigneron P, Reyne Y, Nouguès J, Casteilla L, et al. Expression of specific white adipose tissue genes in denervation-induced skeletal muscle fatty degeneration. FEBS Lett. 1998;439:89–92.
Marcus RL, Addison O, Dibble LE, Foreman KB, Morrell G, Lastayo P. Intramuscular adipose tissue, sarcopenia, and mobility function in older individuals. J Aging Res. 2012;2012:629637.
Yañez R, Lamana ML, García-Castro J, Colmenero I, Ramírez M, Bueren JA. Adipose tissue-derived mesenchymal stem cells have in vivo immunosuppressive properties applicable for the control of the graft-versus-host disease. Stem Cells. 2006;24:2582–91.
Bochev I, Elmadjian G, Kyurkchiev D, Tzvetanov L, Altankova I, Tivchev P, et al. Mesenchymal stem cells from human bone marrow or adipose tissue differently modulate mitogen-stimulated B-cell immunoglobulin production in vitro. Cell Biol Int. 2008;32:384–93.
Brack AS, Conboy MJ, Roy S, Lee M, Kuo CJ, Keller C, et al. Increased Wnt signaling during aging alters muscle stem cell fate and increases fibrosis. Science. 2007;317:807–10.
Shefer G, Wleklinski-Lee M, Yablonka-Reuveni Z. Skeletal muscle satellite cells can spontaneously enter an alternative mesenchymal pathway. J Cell Sci. 2004;117:5393–404.
Joe AW, Yi L, Natarajan A, Le Grand F, So L, Wang J, et al. Muscle injury activates resident fibro/adipogenic progenitors that facilitate myogenesis. Nat Cell Biol. 2010;12:153–63.
Uezumi A, Fukada S, Yamamoto N, Takeda S, Tsuchida K. Mesenchymal progenitors distinct from satellite cells contribute to ectopic fat cell formation in skeletal muscle. Nat Cell Biol. 2010;12:143–52.
Paylor B, Natarajan A, Zhang RH, Rossi F. Nonmyogenic cells in skeletal muscle regeneration. Curr Top Dev Biol. 2011;96:139–65.
Davis RL, Weintraub H, Lassar AB. Expression of a single transfected cDNA converts fibroblasts to myoblasts. Cell. 1987;51:987–1000.
Cao Y, Yao Z, Sarkar D, Lawrence M, Sanchez GJ, Parker MH, et al. Genome-wide MyoD binding in skeletal muscle cells: a potential for broad cellular reprogramming. Dev Cell. 2012;18:662–74.
Anastasia L, Sampaolesi M, Papini N, Oleari D, Lamorte G, Tringali C, et al. Reversine-treated fibroblasts acquire myogenic competence in vitro and in regenerating skeletal muscle. Cell Death Differ. 2006;13:2042–50.
Evans MJ, Kaufman MH. Establishment in culture of pluripotential cells from mouse embryos. Nature. 1981;292:154–6.
Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126:663–76.
Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, Tomoda K, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell. 2007;131:861–72.
Nakagawa M, Koyanagi M, Tanabe K, Takahashi K, Ichisaka T, Aoi T, et al. Generation of induced pluripotent stem cells without Myc from mouse and human fibroblasts. Nat Biotechnol. 2008;26:101–6.
Okita K, Nakagawa M, Hyenjong H, Ichisaka T, Yamanaka S. Generation of mouse induced pluripotent stem cells without viral vectors. Science. 2008;322:949–53.
Zhou H, Wu S, Joo JY, Zhu S, Han DW, Lin T, et al. Generation of induced pluripotent stem cells using recombinant proteins. Cell Stem Cell. 2011;4:381–4.
Kim D, Kim CH, Moon JI, Chung YG, Chang MY, Han BS, et al. Generation of human induced pluripotent stem cells by direct delivery of reprogramming proteins. Cell Stem Cell. 2009;4:472–6.
Soldner F, Hockemeyer D, Beard C, Gao Q, Bell GW, Cook EG, et al. Parkinson's disease patient-derived induced pluripotent stem cells free of viral reprogramming factors. Cell. 2009;136:964–77.
Hanna J, Markoulaki S, Schorderet P, Carey BW, Beard C, Wernig M, et al. Direct reprogramming of terminally differentiated mature B lymphocytes to pluripotency. Cell. 2008;4:513–24.
Stadtfeld M, Brennand K, Hochedlinger K. Reprogramming of pancreatic beta cells into induced pluripotent stem cells. Curr Biol. 2008;18:890–4.
Kim JB, Zaehres H, Wu G, Gentile L, Ko K, Sebastiano V, et al. Pluripotent stem cells induced from adult neural stem cells by reprogramming with two factors. Nature. 2008;454:646–50.
Aasen T, Raya A, Barrero MJ, Garreta E, Consiglio A, Gonzalez F, et al. Efficient and rapid generation of induced pluripotent stem cells from human keratinocytes. Nat Biotechnol. 2008;26:1276–84.
Loh YH, Agarwal S, Park IH, Urbach A, Huo H, Heffner GC, et al. Generation of induced pluripotent stem cells from human blood. Blood. 2009;113:5476–9.
Tan KY, Eminli S, Hettmer S, Hochedlinger K, Wagers AJ. Efficient generation of iPS cells from skeletal muscle stem cells. PLoS One. 2011;6:e26406.
Darabi R, Arpke RW, Irion S, Dimos JT, Grskovic M, Kyba M, et al. Human ES- and iPS-derived myogenic progenitors restore dystrophin and improve contractility upon transplantation in dystrophic mice. Cell Stem Cell. 2012;10:610–9.
Tedesco FS, Gerli MF, Perani L, Benedetti S, Ungaro F, Cassano M, et al. Transplantation of genetically corrected human iPSC-derived progenitors in mice with Limb Girdle Muscular Dystrophy. Sci Transl Med. 2012;4:140ra89.
Ahmed RP, Haider HK, Buccini S, Li L, Jiang S, Ashraf M. Reprogramming of skeletal myoblasts for induction of pluripotency for tumor-free cardiomyogenesis in the infarcted heart. Circ Res. 2011;109:60–70.
Palafacchina G, Blaauw B, Schiaffino S. Role of satellite cells in muscle growth and mantainance of muscle mass. Nutrit Metab Cardio Dis. 2012. doi:10.1016/j.numecd.2012.02.002.
Jejurikar SS, Kuzon Jr WM. Satellite cell depletion in degenerative skeletal muscle. Apoptosis. 2003;8:573–8.
Allen DL, Linderman JK, Roy RR, Bigbee AJ, Grindeland RE, Mukku V, et al. Apoptosis: a mechanism contributing to remodeling of skeletal muscle in response to hindlimb unweighting. Am J Physiol. 1997;273:C579–87.
Vescovo G, Zennaro R, Sandri M, Carraro U, Leprotti C, Ceconi C, et al. Apoptosis of skeletal muscle myofibers and interstitial cells in experimental heart failure. J Mol Cell Cardiol. 1998;30:2449–59.
Jejurikar SS, Henkelman EA, Cederna PS, Marcelo CL, Urbanchek MG, Kuzon Jr WM. Aging increases the susceptibility of skeletal muscle derived satellite cells to apoptosis. Exp Gerontol. 2006;41:828–36.
Bruusgaard JC, Gundersen K. In vivo time-lapse microscopy reveals no loss of murine myonuclei during weeks of muscle atrophy. J Clin Invest. 2008;1184:1450–7.
Van der Meer SF, Jaspers RT, Jones DA, Degens H. Time-course of changes in the myonuclear domain during denervation in young-adult and old rat gastrocnemius muscle. Muscle Nerve. 2011;43:212e22.
Miller SC, Ito H, Blau HM, Torti FM. Tumor necrosis factor inhibit human myogenesis in vitro. Mol Cell Biol. 1988;8:2295–301.
Szalay K, Rázga Z, Duda E. TNF inhibits myogenesis and downregulates the expression of myogenic regulatory factors myoD and myogenin. Eur J Cell Biol. 1997;74:391–8.
Guttridge DC, Mayo MW, Madrid LV, Wang CY, Baldwin Jr AS. NF-kappaB-induced loss of MyoD messenger RNA: possible role in muscle decay and cachexia. Science. 2000;289:2363–6.
Coletti D, Yang E, Marazzi G, Sassoon D. TNFalpha inhibits skeletal myogenesis through a PW1-dependent pathway by recruitment of caspase pathways. EMBO J. 2002;21:631–42.
Coletti D, Moresi V, Adamo S, Molinaro M, Sassoon D. Tumor necrosis factor-alpha gene transfer induces cachexia and inhibits muscle regeneration. Genesis. 2005;43:120–8.
Mitchell PO, Pavlath GK. Skeletal muscle atrophy leads to loss and dysfunction of muscle precursor cells. Am J Physiol Cell Physiol. 2004;287:C1753–62.
Collins CA, Zammit PS, Ruiz AP, Morgan JE, Partridge TA. A population of myogenic stem cells that survives skeletal muscle aging. Stem Cells. 2007;25:885e94.
Day K, Shefer G, Shearer A, Yablonka-Reuveni Z. The depletion of skeletal muscle satellite cells with age is concomitant with reduced capacity of single progenitors to produce reserve progeny. Dev Biol. 2010;340:330–43.
Carlson BM, Faulkner JA. Muscle transplantation between young and old rats: age of host determines recovery. Am J Physiol. 1989;256:C1262e6.
Conboy IM, Conboy MJ, Wagers AJ, Girma ER, Weissman IL, Rando TA. Rejuvenation of aged progenitor cells by exposure to a young systemic environment. Nature. 2005;433:760e4.
Brack AS, Conboy IM, Conboy MJ, Shen J, Rando TA. A temporal switch from notch to Wnt signaling in muscle stem cells is necessary for normal adult myogenesis. Cell Stem Cell. 2008;2:50e9.
Brack AS, Conboy MJ, Roy S, Lee M, Kuo CJ, Keller C, et al. Increased Wnt signaling during aging alters muscle stem cell fate and increases fibrosis. Science. 2007;317:807e10.
Conboy IM, Rando TA. Heterochronic parabiosis for the study of the effects of aging on stem cells and their niches. Cell Cycle. 2012;11:2260–7.
Carlson ME, Hsu M, Conboy IM. Imbalance between pSmad3 and Notch induces CDK inhibitors in old muscle stem cells. Nature. 2008;454:528–32.
Carlson ME, Conboy MJ, Hsu M, Barchas L, Jeong J, Agraval A, et al. Relative roles of TGF-beta1 and Wnt in the sistemic regulation and aging of satellite cell responses. Aging Cell. 2009;8:676–89.
Carlson ME, Suetta C, Conboy MJ, Aagard P, Mackey A, Kjaer M, et al. Molecular aging and rejuvenation of human muscle stem cells. EMBO Mol Med. 2009;1:381–91.
Chakkalakal JV, Jones KM, Basson MA, Brack AS. The aged niche disrupts muscle stem cell quiescence. Nature. 2012;490:355–60.
Siriett V, Platt L, Salerno MS, Ling N, Kambadur R, Sharma M. Prolonged absence of myostatin reduces sarcopenia. J Cell Physiol. 2006;209:866–73.
Siriett V, Salerno MS, Berry C, Nicholas G, Bower R, Kambadur R, et al. Antagonism of myostatin enhances muscle regeneration during sarcopenia. Mol Ther. 2007;15:1463–70.
McKay BR, Ogborn DI, Bellamy LM, Tarnopolsky MA, Parise G. Myostatin is associated with age-related human muscle stem cell dysfunction. FASEB J. 2012;26:2509–21.
Murphy MM, Lawson JA, Mathew SJ, Hutcheson DA, Kardon G. Satellite cells, connective tissue fibroblasts and their interactions are crucial for muscle regeneration. Development. 2011;138:3625–37.
Lepper C, Pertridge TA, Fan CM. An absolute requirement for Pax7-positive satellite cells in acute injury-induced skeletal muscle regeneration. Development. 2011;138:3639–46.
Sambasivan R, Yao R, Kissenpfennig A, Van Wittenberghe L, Paldi A, Gayraud-Morel B, et al. An absolute requirement for Pax7-positive satellite cells in acute injury-induced skeletal muscle regeneration. Development. 2011;138:3647–56.
Relaix F, Zammit SP. Satellite cells are essential for skeletal muscle regeneration: the cell on the edge returns centre stage. Development. 2012;139:2845–56.
Darabi R, Gehlbach K, Bachoo RM, Kamath S, Osawa M, Kamm KE, et al. Functional skeletal muscle regeneration from differentiating embryonic stem cells. Nat Med. 2008;14:134–43.
Darabi R, Pan W, Bosnakovski D, Baik J, Kyba M, Perlingeiro RC. Functional myogenic engraftment from mouse iPS cells. Stem Cell Rev. 2011;7:948–57.
Darabi R, Santos FN, Filareto A, Pan W, Koene R, Rudnicki MA, et al. Assessment of the myogenic stem cell compartment following transplantation of Pax3/Pax7-induced embryonic stem cell-derived progenitors. Stem Cells. 2011;29:777–90.
Kamochi H, Kurokawa MS, Yoshikawa H, Ueda Y, Masuda C, Takada E, et al. Transplantation of myocyte precursors derived from embryonic stem cells transfected with IGFII gene in a mouse model of muscle injury. Transplantation. 2006;82:516–26.
Mizuno Y, Chang H, Umeda K, Niwa A, Iwasa T, Awaya T, et al. Generation of skeletal muscle stem/progenitor cells from murine induced pluripotent stem cells. FASEB J. 2010;24:2245–53.
Chang H, Yoshimoto M, Umeda K, Iwasa T, Mizuno Y, Fukada S, et al. Generation of transplantable, functional satellite-like cells from mouse embryonic stem cells. FASEB J. 2009;23:1907–19.
Quattrocelli M, Palazzolo G, Floris G, Schöffski P, Anastasia L, Orlacchio A, et al. Intrinsic cell memory reinforces myogenic commitment of pericyte-derived iPSCs. J Pathol. 2011;223:593–603.
Acknowledgments
The authors certify that they comply with the ethical guidelines for authorship and publishing of the Journal of Cachexia, Sarcopenia and Muscle (von Haehling S, Morley JE, Coats AJS, Anker SD. Ethical guidelines for authorship and publishing in the Journal of Cachexia, Sarcopenia and Muscle. J Cachexia Sarcopenia Muscle. 2010; 1:7–8).
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Sirabella, D., De Angelis, L. & Berghella, L. Sources for skeletal muscle repair: from satellite cells to reprogramming. J Cachexia Sarcopenia Muscle 4, 125–136 (2013). https://doi.org/10.1007/s13539-012-0098-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13539-012-0098-y