
Abstract
Background
The skeletal muscle mass is the largest organ in the healthy body, comprising 30–40 % of the body weight of an adult man. It confers protection from trauma, locomotion, ventilation, and it represents a “sink” in glucose metabolism and a reservoir of amino acids to other tissues such as the brain and blood cells. Naturally, loss of muscle has dire consequences for health as well as functionality. Muscle loss is a natural consequence of especially aging, inactivity, and their associated metabolic dysfunction, but it is strongly accelerated in critical illness such as organ failure, sepsis, or cancer. Whether this muscle loss is considered a primary or secondary condition, it is known that muscle loss is a symptom that predicts morbidity and mortality and one that is known to impact quality of life and independence. Therefore, monitoring of muscle mass is relevant in a number of pathologies as well as in clinical trials as measures of efficacy as well as safety.
Methods and results
Existing biomarkers of muscle mass or muscle loss have shown to be either too unreliable or too impractical in relation to the perceived clinical benefit to reach regular clinical research or use. We suggest serological neoepitope biomarkers as a possible technology to address some of these problems. Blood biomarkers of this kind have previously been shown to respond with high sensitivity and shorter time to minimum significant change than available biomarkers of muscle mass. We provide brief reviews of existing muscle mass or function biomarker technologies, muscle protein biology, and existing neoepitope biomarkers and proceed to present tentative recommendations on how to select and detect neoepitope biomarkers.
Conclusion
We suggest that serological peptide biomarkers whose tissue and pathology specificity are derived from post-translational modification of proteins in tissues of interest, presenting so-called neoepitopes, represents an exciting candidate technology to fill out an empty niche in biomarker technology.
Similar content being viewed by others


1 Introduction
The loss of muscle mass is known by many names: sarcopenia (literally “poverty of flesh”) describes the “physiological” muscle loss associated with aging that for some individuals reach a certain threshold of clinical significance, whereas cachexia (literally “bad condition”) or wasting syndrome describes the accelerated muscle loss associated with critical illness or serious trauma. The related condition, frailty syndrome, covers the condition, where lack of strength and functional capacity are considered primary. Very often, these conditions will coexist with other morbidities that may or may not be the cause of the loss of muscle mass or function [1, 2].
Muscle loss is an important and underestimated clinical problem in itself, as it is a primary consequence of virtually all kinds of poor lifestyle and also a very common comorbidity with a number of systemic pathologies, e.g., diabetes, inflammatory conditions, solid and nonsolid cancers, most organ failures, sepsis, immobilization, and some orthopedic conditions. The clinical relevance is obvious as a certain amount of muscle strength and thus by extension muscle size is required to sustain bodily function whether the task at hand is locomotion, respiration, or metabolic function. Thus, besides affecting softer endpoints, like functional capacity and quality of life, both muscle mass and strength have been shown to be independent predictors of mortality and morbidity in a range of populations [1, 2]. Loss of functional capacity strongly accelerates metabolic dysfunction and increases loss of bone minerals, making new biomarkers of muscle mass or function highly relevant [3, 4].
In this review paper, we provide brief reviews on the physiology of muscle protein turnover, neoepitope technology, and existing biomarkers. Furthermore, we suggest that developing post-translational modification (PTM)-derived blood sarcopenia biomarkers for diagnostic or research purposes is not only feasible, but would complement the current range of diagnostic tools available significantly and thus assist the drug development process. Furthermore, we present relevant parent proteins and muscle loss pathology-specific PTM that are candidates for neoepitope prospecting.
1.1 Ins and outs of skeletal muscle protein metabolism
There are several reasons why abnormal muscle metabolism resulting in muscle loss ought to result in measureable increases or decreases in discrete protein fragments in blood from extracellular matrix (ECM), myofibrils, costameres, or other myocellular compartments.
-
1.
Muscle tissue is very abundant, comprising 30–40 % of adult male body mass and 20–30 % of adult female body mass, making it the largest organ in normal healthy adults.
-
2.
Muscle tissue is fairly homogenous in structure and composition, meaning that the proteins of myocellular structures as the myofibrils and the costameres are among the most abundant in the human body.
-
3.
As described below, the resting turnover of muscle proteins is very high. In the normal healthy adult man, several hundred grams of muscle tissue is turned over every day in the resting state, making the protein turnover in skeletal muscle one of the most active protein metabolic processes in the body [5].
-
4.
The body has a remarkable ability to grow or shed muscle mass as per the external demands put on the body. With rigorous exercise and dieting, the muscle mass can be doubled and with pharmaceutical aid even tripled or more. On the other hand, during critical illness, muscle loss can exceed several percent per day [6]. This is in contrast to normophysiological muscle loss associated with normal aging, where a loss of 0.5–1.0 % muscle mass per year should be expected.
It is known that the resting turnover of muscle is fairly high (0.025–0.1 %/h, depending on method), with the turnover of intracellular protein being slightly higher than that of extracellular proteins [5]. For an average adult man with approximately 24 kg of skeletal muscle, this amounts to 144–576 g of muscle per day. Obviously, this means that changes in muscle mass can be driven by changes in gross protein synthesis as well as in gross protein degradation. In physiological aging, a rate of muscle loss of approximately 0.5–1.0 % per year should be expected. When sarcopenia manifests, this is a consequence of slightly accelerated muscle loss due to genetic or environmental factors or due to starting the decline of muscle loss at a lower maximal value. Nevertheless, with rates of muscle loss in this order of magnitude, net protein degradation is only very slightly increased, causing only a few (1–3) grams of muscle to be lost per day on average. It is still a matter of some controversy whether this is driven by an impairment of gross synthesis or an increase in gross degradation [7].
During cachexia, muscle loss occurs much faster, sometimes exceeding 1 % of total muscle mass per day. This degradation is most likely driven by increases in degradation as well as decreases in synthesis, although this is also a matter of debate [8–11].
This means that in all other cases than cachectic muscle loss, it is especially relevant to find novel biomarkers or panels thereof that reflect changes in net protein metabolism, rather than changes in gross synthesis or degradation, as the relative changes in net protein metabolism in most cases are orders of magnitude smaller than those of gross protein metabolism (Fig. 1).

Overview of net and gross protein synthesis and degradation rates in muscle during various conditions or states. The figure clearly shows that in all but the most critically ill, net protein metabolism (whether it is net synthesis or net degradation) is vastly smaller than gross degradation or synthesis. Hence, a good biomarker or panel of biomarkers should reflect net degradation or synthesis
Serological neoepitope biomarkers have previously been shown to manifest exactly that quality [12]. This is of particular interest as the only measures approaching net changes in protein synthesis available now are stable isotope techniques that are very operationally complex requiring stable isotope infusion, multiple tissue samplings, and arteriovenous blood samplings.
The total amount of protein turned over in muscle is thus one of the largest single contributors to whole-body protein metabolism, underscoring what a dynamic process this is. Furthermore, it highlights the remarkable adaptability of muscle protein metabolism. This huge protein turnover also increases the likelihood of peptide byproducts of protein synthesis or degradation escape to the circulation during synthesis or degradation, presenting possibly biomarker targets. Indeed, muscle proteins have been shown to appear in blood and urine, even in healthy individuals [13, 14].
1.2 Neoepitope biomarkers
1.2.1 What is a neoepitope biomarker?
Most regular protein biomarkers in blood relevant to skeletal or cardiac muscle, e.g., creatine kinase, myoglobin, or troponin I, are thought to be mostly intact proteins that for some reason (usually tissue damage-induced membrane leakiness) enter the circulation. Therefore, the amount of these proteins in the blood is a product of (1) the amount of donor tissue, (2) protein amounts in said tissue, and (3) the release/excretion kinetics (usually depending on membrane leakiness for the provided examples). With neoepitopes, another selection or specificity criteria is imposed through PTM.
A neoepitope is an epitope that is produced through modification of an existing molecule, e.g., proteolytic cleavage or addition of chemical groups. The specific site on the molecule that has been modified thus presents a novel non-self-epitope for which antibodies can be raised that will not recognize the intact protein. In the case of a cleavage site, even though the same residues exist in the intact molecule and the neoepitope in that part of the peptide, the very carboxy- or aminoterminal end that has been laid bare by the cleavage, represents a novel epitope not present in the intact peptide, therefore constituting a neoepitope.
Usually, pathology affects protein processing in some way or another, leading to production of different peptide species, e.g., if a particular pathology is associated with upregulation of the activity of a particular protease, this will result in cleavage product that are unique to this pathology or at least of higher abundance. Thus, the levels of this neoepitope peptide in blood is a product of (1) the amount of donor tissue, (2) the protein amounts in said tissue, (3) the activity of pathology-related protease, and (4) the release/excretion kinetics. Therefore, neoepitopes can in principle be biomarker of any pathology that causes pathology-specific PTMs, leading to production of unique neoepitopes. These pathology-specific PTMs can be protease cleavages, formation of crosslinks, covalent additions of organic groups, or any other PTM-producing novel epitopes.
Muscle is special in this regard as membrane leakiness is a consequence of muscle damage itself, and therefore intact proteins can be indicative of damage to skeletal or cardiac muscle, e.g., creatine kinase or myoglobin. But muscle atrophy or hypertrophy is not associated with changes in leakiness as such, which is where neoepitope technologies could play a new part as their production and abundancy is dictated by another selection criterion that is pathology-related PTM.
1.2.2 Potential benefits of neoepitopes in sarcopenia and cachexia
Reiterating, serological neoepitope biomarkers display tissue- and pathology-specificity through a unique combination of substrate protein and PTM. This produces peptide fragment antigens that can be recognized in high-sensitivity immunosorbent assays.
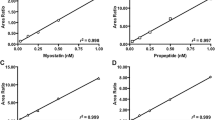
This class of biomarkers has already shown promise as a prognostic/diagnostic tool. As they are produced by a combination of tissue-specific parent proteins and tissue and pathology-specific PTMs, they do not reflect a condition or state, like creatinine presumably reflects muscle mass, but a process. This allows for early detection, especially in slow progressive diseases such as osteoporosis or arthritic conditions, because of a shorter time to minimal significant change than with existing biomarker technologies (Fig. 2) [12]. Sarcopenia or iatrogenic muscle loss, e.g., from statins or glucocorticoids, are both also accumulated fairly slowly and this represents a situation that would benefit from early-response biomarkers as existing technologies would require months to detect accelerated muscle loss. Likewise, several antisarcopenic treatments such as selective androgen receptor modulators are in clinical trial, and again early detection or quantification of efficacy could increase the economic efficiency of clinical trials of these antisarcopenic treatments, by identifying nonresponders.

The dynamics of responses of biomarkers with different sensitivities to change. Muscle mass or function in itself changes slowly and thus biomarkers of muscle mass or function (blue line) will take a long time to detect minimal significant change. A biomarker responsive to the process of muscle loss (red line), rather than muscle mass or function in itself will, if reliable enough, require a much shorter time to MSC
Thus, if a biomarker with the same sensitivity to muscle loss could be found, that has the same sensitivity that have previously been found for bone loss or arthritis, this would be highly useful in disease prognosis or in identifying disease progressors drug “responders”, or even adverse effect responders; thereby, helping pinpoint vulnerable individuals early and individualizing treatment options accordingly.
1.2.3 Extra- vs. intracellular parent proteins
As peptide fragments from processing of extracellular proteins escapes more readily into the blood than does fragments from intracellular or membrane proteins, they represent a more likely source of blood biomarkers. Neoepitopes thus produced from extracellular matrix proteins have been shown to work as serological biomarkers for a range of pathologies in connective tissue [15–17].
While research in the degradation and processing of intracellular and membrane proteins in muscle has accumulated a wealthy literature, particularly focusing on the canonical calcium-dependent, ubiquitin-dependent, and lysosomal proteolytic pathways, very little research has been directed at the destiny of peptides from processing of extra- or intracellular proteins from muscle, thus presenting a relatively unexplored scientific niche. Despite the aforementioned academic interest in proteolytic machinery in muscle, quite few of their proteolytic fragments have been characterized.
1.2.4 Neoepitopes in disease etiology
In some diseases, aberrant protein modification produces neoepitope peptide fragments that are not only markers of disease, but also contribute to the pathology in itself, as is seen in Alzheimer, where Tau fragments contribute to formation of neurofibrillar tangles, that ultimately cause neuron death [18]. In muscle pathology, this is seen in various forms of myositis and dermatomyositis, where a degree of autoimmunity against certain epitopes partly or fully explains and causes the muscle pathology [19, 20]. In these cases, development of sensitive antibodies may obviously not only represent a means with which to detect biomarkers of pathology, but possibly also an entry point for novel treatment technologies [21].
1.3 Existing biomarker technologies
1.3.1 Existing biomarker technologies
Several biomarker technologies are available that characterizes muscle mass, muscle function, or muscle loss; but so far, none are in regular clinical practice. This is in part due to inadequacies of the available technologies and in part due to the perceived clinical benefit obtained (summary in Table 1).
Most measures of strength or functional capacity has poor reliability and reproducibility and the ability to track changes in individuals is hampered by learning effects on testing, i.e., learning effects may improve scores, masking “true” losses of strength or functionality.
Imaging techniques used to assess muscle mass such as magnetic resonance imaging (MRI), computerized tomography (CT), or dual X-ray absorptiometry are sensitive to changes in electrolytes and edema, both of which are frequently present in sarcopenic or cachectic patient. Also, MRI and CT could be considered costly in comparison to the perceived clinical benefit. The more classic anthropometric measures, body fat calipers, BIA, or hydrostatic weighing, are also sensitive to edema and require either considerable skill (calipers) or are impractical in the clinical setting (hydrostatic weighing). What all of these classic measures share, however, is that with them, it will usually take quite a while to reach minimum significant change, as they are markers of muscle mass, and not change in muscle mass.
Twenty-four-hour creatinine excretion can, to some extent, be considered a marker of muscle mass, but this displays high variation and is sensitive to diet (meat intake) and 24-h urine sampling can be logistically challenging [22, 23].
Serum or urine 3-methylhistidine has also been used as a marker of muscle protein degradation. Myosin and possibly actin is 3-methylated in muscle and the resulting amino acid 3-methylhistidine is not recycled for intermediary metabolism or protein synthesis, which in principle makes it an ideal biomarker, as it should represent gross protein degradation based on its biology. However, its validity has been questioned in recent years as it has been shown to not respond to interventions known by other measures to increase protein degradation, i.e., voluntary or involuntary supramaximal eccentric work [24]. Also, doubts have been raised about the validity of this as a marker of skeletal muscle protein degradation as the contribution from smooth muscle appears to be big enough to disturb results significantly [24, 25].
To summarize, there appears to be a gap in technologies that can detect muscle loss easily and in an early response manner, which are traits that neoepitope biomarkers have displayed with other degenerative connective tissue conditions.
1.3.2 BIPED classification of biomarker technologies
The Osteoarthritis Biomarkers Network has suggested a nomenclature for biomarker applications abbreviated BIPED (short for burden of disease, investigative, prognostic, efficacy, and diagnostic) [26]. As this nomenclature is practical and contains no inherent restrictions towards use in other pathologies, it can just as well be applied to biomarkers of muscle loss. Also, while the BIPED criteria are worded with measures of efficacy in mind, they can equally well be applied within safety assessment, measuring adverse effects on muscle, e.g., adverse muscle effects of glucocorticoid or statin treatment interventions. Each of the BIPED biomarker classifications presents individual demands on reliability, sensitivity, specificity, etc. (summarized in Table 2). Not only does this system provide a relevant nomenclature regarding biomarkers, it also clearly reveals the need of improved biomarkers of muscle mass and muscle loss as few markers have the sensitivity or the biological rationale to be able to function as prognostic tools.
Using the BIPED nomenclature in biomarker application is of particular relevance in clinical trials, where diagnostic and burden of disease markers can be used to select, deselect, or stratify subjects according to disease progressions or other pathophysiological variables. Good prognostic biomarkers can be used to identify vulnerable individuals, which is of help in selecting treatment groups and efficacy markers can be used to separate responders from nonresponder, which is useful, as treatment nonresponder can be deselected for treatment and therefore not exposed to possible adverse effects. All of these applications can thus help reduce the otherwise escalating costs of pharmaceutical clinical trials and thereby contribute to pharmaceutical development. This has been deemed necessary by the Food and Drug Administration in their “critical path” position stand from 2004, in order to maintain progress in global clinical development [27].
1.4 How can we isolate new muscle loss biomarkers?
Assuming that these neoepitope biomarkers for muscle loss are as sensitive as biomarkers of other degenerative connective tissue conditions, then how do we find them and measure them?
A proteomic screening approach, like quantitative mass spectrometry (MS), seems like the obvious choice, but as the blood protein matrix is very complex, this requires advanced mass spectrometry equipment and bioinformatics skills only available to few labs and even then it represents a herculean effort. A more “classic” approach could be selecting peptides excreted from muscle by doing gel-based proteomics comparing A/V blood or microdialysates from the tissue in question, but again the complexity of the blood protein matrix hampers this approach.
An easier, albeit more risky approach, would be to make qualified guesses based on in silico work as to which proteins and PTMs would combine during muscle loss pathology and subsequently be excreted into the circulation. When one or more such candidates have been pinpointed, recombinant or purified parent protein can be subjected to the PTM process in vitro, e.g., protease digestion of the parent protein, in order to identify or confirm if the post-translationally modified peptides are actually produced and not just predicted. If successful, antibodies can be raised against this PTM-generated epitope in the peptide, which could subsequently be used to detect it quantitatively in an ELISA assay or other antibody-based technique. If an MS-based technique would be used, knowing the identity of the candidate peptide can make the process easier by allowing for fractionation prior to mass MS, e.g., by chromatography, and by making the mass spectrometry analysis easier by narrowing down the peptide fragments in the MS which could be of interest.
Indeed, the former methods have previously produced several successful biomarkers, like the aforementioned CTX-I for bone loss. Also, the first true muscle pathology biomarker has also been discovered like this. It is a fragment produced by neurotrypsin cleavage of agrin, a protein enriched at costameres and neuromuscular junctions [28]. However, this fragment identifies a subset of “neurogenic sarcopenia” and cannot be considered a generic muscle loss biomarker based on the presently available results. Nevertheless, both of these beautifully illustrate the combination of specificity provided by parent protein and pathology, producing a marker of neurogenic sarcopenia in muscle.
Thus, irrespective of what experimental approach is used, one of the tasks in finding biomarker candidates is to isolate tissue- and pathology-specific molecular fragments. This specificity can arise from any combination of parent protein and PTM (Table 3). In this context, PTMs covers all protein modification that occurs during the life cycle of a protein—translation through maturation, wear and tear, and degradation (Table 4). PTMs applied during different stages of the life cycle of a protein can lead to different biomarker interpretations. For example, propeptides cleaved from the parent protein during synthesis/maturation are usually used as markers of synthesis of the parent protein, while glycosylation, oxidation, or nitrosylation of susceptible amino acid side chains in the mature, functional protein are used as markers of pathology in a range of conditions and fragments of caspase-, calpain-, or cathepsin-mediated proteolysis are considered markers of terminal protein degradation [29–32].
Of particular interest are the cleavage products generated during protein maturation and degradation, as these fragments have been shown to escape to the circulation and have been shown to be usable as disease biomarkers, as is the case with the CTX-I osteoporosis biomarker (which is a Cathepsin K cleaved fragment of collagen I, containing an isomerization and a cross-link between the two halves of the dipeptide) [12]. Thus, if a correct combination of tissue and pathology specificity can be achieved within the combination of target protein and PTMs, it will result in a tissue-specific pathology marker (Fig. 3). The ability to recognize this in immunoassays naturally depends on the quantity and quality of the antigen in the resulting protein fragment. Especially the cleavage sites themselves are promising in this regard as they represent novel epitopes (neoepitopes) more likely to display sufficient specific immunogenicity than the rest of the peptide (Fig. 4).

Pictogram showing how tissue and pathology specificity of parent proteins and PTMs combine to form neoepitope biomarkers that are indicative of ongoing processes rather than conditions or states

Figure showing how modifications to protein introduces another constraint to abundance, and produces new “tags” which eases detection by antibody or MS-based methods
1.5 Candidate parent proteins and PTMs
For the purpose of biomarker prospecting, we have provided a brief review of muscle proteins and PTMs that represents possible candidates to form neoepitope biomarkers. A lot of candidate proteins could combine with at lot of different candidate PTMs to form neoepitopes that could be biomarkers of muscle pathology; hence, we have set some of the obvious candidate parent proteins up against candidate PTMs in a matrix format (Table 3). This cross-indexed format does not mean to imply that every protein is necessarily subjected to every PTM listed, but that the possible interactions could produce neoepitope biomarkers of interest. It is worth noting that each of these interactions could, in principle, produce several different results, i.e., a protein could be cleaved, carbonylated, or nitrosylated at various different positions.
1.6 Candidate muscle proteins
1.6.1 Muscle-specific proteins
Skeletal muscle is a huge organ, comprising as much of 40–50 % of the body mass in trained, healthy adults. The vast majority of this is occupied by muscle fibers that are characterized by an expansion of the cytoskeleton forming the bundles of contractile protein, the myofibrils, that occupies almost all of these cells [33]. Most of these myofibrillar proteins display specificity to striated muscle, i.e., skeletal and cardiac, and some even to skeletal muscle. In biomarker prospecting, specificity to striated muscle, meaning that cardiac muscle proteins are included as, is not necessarily a problem though, as loss of skeletal muscle probably coexists with decrease in myocardial mass and because the total skeletal muscle mass is so much larger than the cardiac muscle.
The majority of the serological neoepitope biomarkers developed so far are derived from PTM processing of ECM proteins, either during synthesis, maturation, or degradation. This is primarily a consequence of the ease with which degradation fragments from extracellular matrix proteins can enter the circulation. Extracellular proteins are already in the extracellular domain and thus their degradation fragments have a shorter route to the circulation. This is also the case with the newly proposed biomarker of neurogenic sarcopenia, produced by neurotrypsin cleavage of agrin, supposedly from the neuromuscular junction [28]. Most intracellular proteins are degraded exclusively inside the cell through ubiquitin- or calcium-dependent proteolysis, and most membrane proteins are degraded through lysosomal pathways.
Thus, one should not expect intracellular and membrane proteins to release recognizable fragments into the circulation. However, several findings indicate that intracellular proteins as well as proteases may leak into the extracellular compartment with greater ease than we expect. For example, in cachexia, myoglobin from muscle has been shown to appear in the circulation, suggesting that the membrane integrity of cachectic muscle becomes compromised, effectively making the muscle fiber cell membrane “leaky”, creating the possibility that fairly large (myoglobin is approximately 17 kDa) peptides can be observed in blood [13]. Another group have successfully detected intracellular proteins as biomarkers of skeletal muscle or myocardial damage in an animal model [14], again suggesting that a significant degree of “leakiness” is present in muscle. Therefore, protein fragments from all the cellular compartments of muscle may represent biomarker candidates.
1.6.2 Intracellular domain
The myofibrils that occupy the majority of striated muscle cells are composed end-to-end by sarcomeres, the fundamental contractile unit of the myofibril (Fig. 5). The vast majority of sarcomeric protein in the body (>90 %) exists in skeletal muscle, meaning that development of biomarkers against sarcomeric proteins should be fairly muscle-specific, assuming that they are released into circulation. The most abundant muscle proteins by far are the actins and myosins, but the abundance of sarcomeric proteins is very high relative to most other proteins, so most of these could represent possible targets for biomarker development, e.g., myosin, actin, troponin, tropomyosin, α-actinin, titin, and tropomyosin [33].

Overview of the sarcomere structure and some of the most abundant structural proteins therein. The myosin thick filaments are seen protruding from the M-disk, whereas the actin filaments are seen protruding from the Z-disks. The sarcomere structure is shared between skeletal and cardiac muscle, but some of the genes present are different isoforms. Reprinted from [81]. PubMed Central was the original publisher and the reprint is used in accordance with PubMed Central’s open access charter
Skeletal muscle fibers can be divided into slow or fast types and this can be used to yield some specificity to skeletal muscle as fast fiber type-specific proteins are not expressed in myocardium, thus representing “true” skeletal muscle specific proteins. Furthermore, it is of particular interest that the initial stages of muscle loss are characterized by selective loss of myosin, especially the fast type IIX myosin [34]. This could possibly be used as a means to discern gradual atrophy, i.e., sarcopenia, from rapid muscle loss, i.e., cachexia/wasting in biomarker assays.
1.6.3 Membrane domain
A majority of the force generated within muscle fibers appear to be transmitted through the sides of the fibers, and into the ECM rather than through the ends [35]. This is accomplished through the costameres (Fig. 6), structures composed of dystroglycan protein complexes (DGC) and integrin focal adhesions (FA), lining muscle fibers like ribs [36–38]. These protein complexes essentially anchor the Z-disks of sarcomeres to the collagen matrix of the muscle ECM and transmit forces from inside the muscle fibers into the ECM that in turn transmit forces to the myotendinous junction [35]. A large number of dystrophies are associated with defects of this mechanical connection between the sarcomeres and the ECM, most notably the dystroglycan complexes [39]. They are composed of a number of membrane-embedded dystroglycans and sarcoglycans that on the inside are attached to the Z-disks through desmin, dystrophin, dystrobrevin, and syncoilin and on the outside adhere to the basal lamina. The integrin focal adhesions consists of integrin α7β1 complexes, attached to the internal cytoskeleton through vinculin and talin.

This figure shows the structure of the costamere and known molecular interactions. Below the membrane bilayer shown is the intracellular space and above it is the extracellular space. In the intracellular space, the costamere is attached to the contractile proteins through dystrophins (for the dystrophin glycoprotein complex, DGC), vinculin, talin, and paxilin (for the integrin complexes; not shown). In the extracellular space, both DGCs and integrin complexes bind to components of the basal lamina that is attached to the rest of the extracellular matrix that consists mostly of fibrillar collagens. Reprinted from [82] with permission from Elsevier
The costameres are highly abundant along the perimeter of the muscle fibers and their abundance should thus be coregulated with muscle fiber diameter and by extension muscle mass. Therefore, costameric proteins represent good candidates for biomarker production.
1.6.4 Extracellular domain
A majority of the literature on muscle loss completely omits the relevance of the extracellular matrix, despite muscle fibers being fully mechanically and biochemically dependent on being embedded in the muscle ECM. In the literature, a view of muscle as a viscoelastic balloon between two tendons is, however, receding in favor of viewing the muscle essentially as a tendon with thousands of muscle fiber “inserts”, promoting the importance of the ECM in muscle.
The costameres bind to the basal lamina, through the DGC and FA binding to the laminin and DGC-associated biglycan binding to collagen VI. But a large number of other proteins have been described in the basal lamina, e.g., laminins, perlecan, nidogen/entactin, and collagens. The endomysium is primarily composed of collagens I and III. None of these display full muscle specificity, but collagen VI and laminin 211 (formerly known as merosin or laminin-2) seem to be expressed with partial specificity in skeletal muscle and congenital defects of these genes manifest primarily as skeletal muscle abnormalities [40, 41]. No other defects of these two collagen or basement membrane constituents’ results in phenotype restricted to skeletal muscle tissue, suggesting a degree of skeletal muscle specificity.
To summarize, the most obvious parent proteins for muscle loss biomarker candidates are sarcomeric proteins, components of the dystrophin-associated glycoprotein complex, and selected components of the ECM, most notably laminin 211 and collagen VI.
1.7 Muscle specific proteolytic PTMS
The intracellular proteolytic function is maintained by three branches: (1) the ubiquitin–proteasome system (UPS), (2) the calcium-dependent system (calpains and caspases), and (3) the lysosomal system [42–44].
1.7.1 Ubiquitin-dependent proteolysis
Through ubiqination, the UPS targets proteins for degradation in the proteasomes whose proteolytic activity degrades proteins. However, the fragments generated in this system are generally eight amino acids or less, making these fragments too small for routine detection in immunosorbent assays. Therefore, we do not consider proteasomal degradation fragments likely biomarker candidates.
1.7.2 Calcium-dependent proteolysis
The calcium-dependent proteolytic system is comprised by the calpain and caspase families. The calpain family is a large familiy of nonlysosomal calcium-activated cysteine proteases and their endogenous inhibitor calpastatin. Calpain 1 (μ), 2 (m) and 3 (p94) are all expressed in muscle and Calpain 3 is known to be at least partially muscle specific. Defects in this particular calpain manifests primarily in muscle (as limb-girdle muscle dystrophy type 2A), indicating a muscle specific function. Capain 3 is different from calpains 1 and 2 in that it is not inhibited by calpastatin and that it is hypothesized to have regulatory role rather then one of bulk proteolysis of structural proteins [45].
However, the exact function of individual calpains and caspases during accelerated muscle loss is poorly characterized. It is known however that preventing calcium release in muscle in various disease models imparts some resistance to muscle loss [46], as do overexpression of calpastatin, the endogenous calpain inhibitor [47].
Furthermore, degradation of myofibrillar proteins has been hypothesized to be dependent on initial digestion by calpain to release the them from myofibrils and subsequent UPS-dependent degradation [48], but this hypothesis has been challenged in the more recent literature, ascribing lysosomal degradation a more important role [49, 50].
Besides being canonical activators of the apoptosis cascade, several members of the caspase family also functions as regular proteases degrading structural protein, as have been shown with caspase-3 cleavage of actin during cachexia [51]. This is further supported by another study that reports increases in proteolytic activity of most caspases during selected cancer cachexia models, especially caspase-3, -6, and -9, interestingly in the absence of indices of apoptosis [51], again supporting their non-apoptotic proteolytic activity.
With aging and in metabolically compromised muscle, intracellular calcium levels rise, thereby possibly causing aberrant calpain/caspase activity, as has been shown in other tissues [52]. This has been hypothesized to be a generic contributing or even initiating factor in muscle loss. Therefore, we consider proteolytic processing by calpains, especially 1 and 2, or caspases, especially -3, -6, and -9, to be likely to generate specific protein fragments useful in biomarker design.
1.7.3 Lysosomal proteases
Lysosomal proteolysis is performed by cathepsins. Most of these operate within the lysosome organelles, but some are secreted to the extracellular space and some are active in the cytoplasm [44].
Several of these have been shown to be associated with accelerated muscle loss, but especially cathepsin L seem to be consistently involved in muscle loss across a range of models [53–56]. Interestingly, cathepsin L have been shown to be situated downstream of FOXO1 signaling, further implicating it in negative regulation of protein metabolism [57] and suggesting coregulation with UPS proteolysis. cathepsin B and D have also been shown to increase in some muscle loss models [58–60]. Of particular notice, cathepsin L has been shown to degrade most myofibrillar proteins in vitro, and cathepsin B has been shown to display selectivity for myosin heavy chain, making these obvious biomarker PTM protease candidates [61, 62].
1.7.4 Extramyocellular proteases
The primary extracelllar proteases associated with muscle loss are the matrix metalloproteinases (MMP) MMP-2 and MMP-9. Both of these have been shown to be upregulated in a number of models of muscle loss [63–65]. MMP-2 is constitutively expressed (but not active), whereas MMP-9 expression is induced. Following catabolic stimuli, MMP-9 activity increases rapidly, whereas MMP-2 increases days later [64]. Inhibitors of MMPs have been shown to alleviate the muscle phenotype in mdx mice (animal Duchenne muscle dystrophy model) [66, 67] but this route has not been expanded to generalized nondystrophic muscle loss.
1.8 Nonproteolytic PTMs
As in most other tissues, a large number of nonproteolytic PTMs are produced in muscle; but so far, none have been reliably associated with pathological muscle loss in itself. Several are related to oxidative stress or hyperglycemia, which are both in themselves indirectly related to muscle loss. But still, most of these are not specific to muscle or loss of muscle or muscle functions per se. We provide a very brief review of some of the most common nonproteolytic PTMs present in muscle.
1.8.1 Actomyosin histidine methylation
As previously mentioned, histidine in muscle actomyosin is 3-methylated, but it is poorly characterized at what histidine positions this methylation is present and only a few of these loci have been described [68]. As this methylation appears to be specific to muscle tissues, it could potentially contribute greatly to the epitope specificity of putative biomarkers, making this a useful PTM to consider when looking for supposedly muscle-specific biomarkers.
1.8.2 Crosslinks
A wide range of crosslinks, especially in collagens, is known to manifest in connective tissue, including the endomysium of muscle. As connective tissue plays an indispensable role in muscle, ensheathing all muscle fibers while being more exposed to the circulation than, e.g., tendon collagen, crosslinks also manifest in muscle connective tissue. Of these, particularly advanced glycation endproduct, especially pentosidine crosslinks are well documented. Unfortunately, none of these are directly related to muscle loss.
But also myosin has been shown to undergo peroxidative crosslinking through an oxidized myoglobin intermediate [69] during oxidative stress. This modification is of particular relevance in immunosorbent assays at it increases effective concentration of antigens in these.
1.8.3 Oxidative chemical modifications
Unchecked oxidative stress causes a range of protein modifications through partially reduced oxygen radicals with high reactivity. This leads to chemical modifications to amino acid side chains like oxidation, nitrosylation, carbonylation, citrullination, etc. Of these PTMs, carbonylation and nitrosylation are the ones whose presence is best documented in muscle proteins.
Nitrosylation is a part of normal modulation as well as a consequence of aberrant oxidative stress. Thus, it is known that “physiological” nitrosylation of skeletal muscle myosin modulates the force–velocity relationship of the actomyosin interaction [70], but oxidative nitrosylation, especially on tyrosine side chains occur as a consequence of oxidative stress. These have even been shown to correlate inversely with muscle mass, although in a very unspecific and cross-sectional model (high/low age x high/low energy intake) and unfortunately only in mitochondrial proteins [71].
In a similar way, carbonylation is a consequence of oxidative stress under physiological as well as pathological conditions and has been shown to manifest in muscle with training as well as with metabolic or inflammatory dysfunction [72, 73]. With diaphragm unloading, muscle oxidative stress and subsequent carbonylation have been shown to increase dramatically [74, 75] and some studies even attribute aberrant oxidative dysfunction a more central role in muscle atrophy as administration of strong antioxidants even prevents muscle loss in some muscle atrophy models [76–79].
To summarize, histidine mythylation in actin and myosin, and oxidative myosin crosslinking as well as tyrosine nitrosylation and carbonylation at all reactive amino acid side chains should be considered when prospecting for biomarkers.
1.9 Candidate parent protein and PTM candidate summary
Skeletal muscle contains several high-abundance proteins from all three compartments, i.e., extracellular, membrane, and intracellular, that could represent candidate parent proteins. As high a degree of specificity to skeletal muscle as possibly is preferable in a muscle loss biomarker candidate, but not necessarily indispensable, as a low degree of tissue specificity of parent protein can be countered by a higher tissue specificity of the PTM in question.
The neoepitope in most existing neoepitope biomarkers is created through proteolysis and because the type of PTM most frequently associated with muscle pathology in the literature is protease activity in a number of proteases, we believe that proteolytic cleavages produced by pathology-associated proteases like calpains, caspases, cathepsins, or MMPs are the most likely PTM candidates. Nonproteolytic PTMs have been less well associated with muscle loss pathology but should not necessarily be excluded. Especially methylation of actin or myosin or some of the various biochemical modifications associated with unchecked oxidative stress could be of interest in finding biomarker candidates. However, these are as of yet less well described than the proteolytic PTMs and we have thus prioritized them accordingly. We have listed what we consider the most likely parent protein and PTM candidates in Table 3 in the top row and left columns, respectively.
2 Conclusion
Muscle tissue seems to display properties that would allow for finding serological biomarkers as a byproduct of changes in muscle quantity and quality, i.e., high abundance, proteome homogeneity and specificity, high resting state turnover, and huge turnover in muscle loss conditions.
We fully acknowledge that there are as of yet no fully developed serological muscle loss biomarkers, but we believe that the success of neoepitope biomarkers in other connective tissue pathologies is both promising in terms of the potential of this technology in muscle loss and have shown the methodological framework with which to approach the scientific hunt for these markers. Indeed, the work done on the neurotrypsin-cleaved agrin fragment is showing that this is a route that the biomarker science community is showing interest.
We therefore propose that further developing immunosorbent assays targeted at peptides from high-abundance muscle proteins, like costameric or sarcomeric protein with PTMs associated with muscle loss, like calpain, caspase, cathepsin, or MMP cleavage, is a viable route to take in order to discover novel serological muscle loss biomarkers.
References
Evans W. Skeletal muscle loss: cachexia, sarcopenia, and inactivity. Am J Clin Nutr. 2010;91:1123S–7S.
Fearon K, Evans WJ, Anker SD. Myopenia—a new universal term for muscle wasting. J Cachexia Sarcopenia Muscle. 2011;2:1–3.
Narici MV, Maffulli N. Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull. 2010;95:139–59.
Evans W. Functional and metabolic consequences of sarcopenia. J Nutr. 1997;127:998S–1003S.
Miller BF, Olesen JL, Hansen M, et al. Coordinated collagen and muscle protein synthesis in human patella tendon and quadriceps muscle after exercise. J Physiol (Lond). 2005;567:1021–33.
White JP, Baynes JW, Welle SL, et al. The regulation of skeletal muscle protein turnover during the progression of cancer cachexia in the Apc(Min/+) mouse. PLoS One. 2011;6:e24650.
Rennie MJ, Selby A, Atherton P, et al. Facts, noise and wishful thinking: muscle protein turnover in aging and human disuse atrophy. ScandJ MedSciSports. 2010;20:5–9.
Rennie MJ, Edwards RH, Emery PW, et al. Depressed protein synthesis is the dominant characteristic of muscle wasting and cachexia. ClinPhysiol. 1983;3:387–98.
Emery PW, Edwards RH, Rennie MJ, et al. Protein synthesis in muscle measured in vivo in cachectic patients with cancer. Br MedJ (ClinResEd). 1984;289:584–6.
Morrison WL, Gibson JN, Rennie MJ. Skeletal muscle and whole body protein turnover in cardiac cachexia: influence of branched-chain amino acid administration. Eur J Clin Invest. 1988;18:648–54.
Rutten EPA, Franssen FME, Engelen MPKJ, et al. Greater whole-body myofibrillar protein breakdown in cachectic patients with chronic obstructive pulmonary disease. Am J Clin Nutr. 2006;83:829–34.
Bonde M, Garnero P, Fledelius C, et al. Measurement of bone degradation products in serum using antibodies reactive with an isomerized form of an 8 amino acid sequence of the C-telopeptide of type I collagen. J Bone Miner Res. 1997;12:1028–34.
Weber M-A, Kinscherf R, Krakowski-Roosen H, et al. Myoglobin plasma level related to muscle mass and fiber composition: a clinical marker of muscle wasting? J Mol Med. 2007;85:887–96.
Tonomura Y, Mori Y, Torii M, et al. Evaluation of the usefulness of biomarkers for cardiac and skeletal myotoxicity in rats. Toxicology. 2009;266:48–54.
Bay-Jensen AC, Leeming DJ, Kleyer A, et al. Ankylosing spondylitis is characterized by an increased turnover of several different metalloproteinase-derived collagen species: a cross-sectional study. Rheumatol Int. doi:10.1007/s00296-011-2237-8. Published Online First: 16 November 2011.
Bay-Jensen A-C, Liu Q, Byrjalsen I, et al. Enzyme-linked immunosorbent assay (ELISAs) for metalloproteinase derived type II collagen neoepitope, CIIM–increased serum CIIM in subjects with severe radiographic osteoarthritis. Clin Biochem. 2011;44:423–9.
Henrotin Y, Deberg M, Dubuc J-E, et al. Type II collagen peptides for measuring cartilage degradation. Biorheology. 2004;41:543–7.
Rissman RA, Poon WW, Blurton-Jones M, et al. Caspase-cleavage of tau is an early event in Alzheimer disease tangle pathology. J ClinInvest. 2004;114:121–30.
Mehndiratta P, Mehta S, Manjila SV, et al. Isolated necrotizing myopathy associated with ANTI-PL12 antibody. Muscle Nerve. 2012;46:282–6.
Nakajima A, Yoshino K, Soejima M, et al. High frequencies and co-existing of myositis-specific autoantibodies in patients with idiopathic inflammatory myopathies overlapped to rheumatoid arthritis. Rheumatol Int. 2012;32:2057–61.
Karsdal MA, Henriksen K, Leeming DJ, et al. Novel combinations of post-translational modification (PTM) neo-epitopes provide tissue-specific biochemical markers—are they the cause or the consequence of the disease? Clin Biochem. 2010;43:793–804.
Heymsfield SB, Arteaga C, McManus C, et al. Measurement of muscle mass in humans: validity of the 24-hour urinary creatinine method. Am J Clin Nutr. 1983;37:478–94.
Wang ZM, Gallagher D, Nelson ME, et al. Total-body skeletal muscle mass: evaluation of 24-h urinary creatinine excretion by computerized axial tomography. Am J Clin Nutr. 1996;63:863–9.
Hansen M, Trappe T, Crameri RM, et al. Myofibrillar proteolysis in response to voluntary or electrically stimulated muscle contractions in humans. ScandJ MedSciSports. 2009;19:75–82.
Millward DJ. PCB. 3-Methylhistidine turnover in the whole body, and the contribution of skeletal muscle and intestine to urinary 3-methylhistidine excretion in the adult rat. Biochem J. 1983;214:607.
Bauer DC, Hunter DJ, Abramson SB, et al. Classification of osteoarthritis biomarkers: a proposed approach. Osteoarthr Cartil. 2006;14:723–7.
FAD Administration. Challenge and opportunity on the critical path to new medical products. 2nd ed. U.S. Department of Health and Human Services; 2004. http://www.fda.gov/downloads/ScienceResearch/SpecialTopics/CriticalPathInitiative/CriticalPathOpportunitiesReports/ucm113411.pdf
Hettwer S, Dahinden P, Kucsera S, et al. Elevated levels of a C-terminal agrin fragment identifies a new subset of sarcopenia patients. Exp Gerontol. doi:10.1016/j.exger.2012.03.002. Published Online First: 11 March 2012.
Huang J, Forsberg NE. Role of calpain in skeletal-muscle protein degradation. Proc Natl Acad Sci USA. 1998;95:12100–5.
Du J, Hu Z, Mitch WE. Molecular mechanisms activating muscle protein degradation in chronic kidney disease and other catabolic conditions. Eur J Clin Invest. 2005;35:157–63.
Lee SW, Dai G, Hu Z, et al. Regulation of muscle protein degradation: coordinated control of apoptotic and ubiquitin–proteasome systems by phosphatidylinositol 3 kinase. J Am Soc Nephrol. 2004;15:1537–45.
Zhao J, Brault JJ, Schild A, et al. FoxO3 coordinately activates protein degradation by the autophagic/lysosomal and proteasomal pathways in atrophying muscle cells. Cell Metabolism. 2007;6:472–83.
Clark KA, McElhinny AS, Beckerle MC, et al. Striated muscle cytoarchitecture: an intricate web of form and function. Annu Rev Cell Dev Biol. 2002;18:637–706.
Gosker HR, Engelen MPKJ, van Mameren H, et al. Muscle fiber type IIX atrophy is involved in the loss of fat-free mass in chronic obstructive pulmonary disease. Am J Clin Nutr. 2002;76:113–9.
Bloch RJ, Gonzalez-Serratos H. Lateral force transmission across costameres in skeletal muscle. Exerc Sport Sci Rev. 2003;31:73–8.
Anastasi G, Amato A, Tarone G, et al. Distribution and localization of vinculin–talin–integrin system and dystrophin–glycoprotein complex in human skeletal muscle. Immunohistochemical study using confocal laser scanning microscopy. Cells TissuesOrgans. 2003;175:151–64.
Acharyya S, Butchbach MER, Sahenk Z, et al. Dystrophin glycoprotein complex dysfunction: a regulatory link between muscular dystrophy and cancer cachexia. Cancer Cell. 2005;8:421–32.
Oak SA, Zhou YW, Jarrett HW. Skeletal muscle signaling pathway through the dystrophin glycoprotein complex and Rac1. J Biol Chem. 2003;278:39287–95.
Rando TA. The dystrophin–glycoprotein complex, cellular signaling, and the regulation of cell survival in the muscular dystrophies. Muscle Nerve. 2001;24:1575–94.
Bönnemann CG. The collagen VI-related myopathies: muscle meets its matrix. Nat Rev Neurol. 2011;7:379–90.
Pegoraro E, Mancias P, Swerdlow SH, et al. Congenital muscular dystrophy with primary laminin alpha2 (merosin) deficiency presenting as inflammatory myopathy. Ann Neurol. 1996;40:782–91.
Taillandier D, Combaret L, Pouch M-N, et al. The role of ubiquitin-proteasome-dependent proteolysis in the remodelling of skeletal muscle. Proc Nutr Soc. 2004;63:357–61.
Costelli P, Tullio RD, Baccino FM, et al. Activation of Ca(2+)-dependent proteolysis in skeletal muscle and heart in cancer cachexia. Br J Cancer. 2001;84:946–50.
Bechet D, Tassa A, Taillandier D, et al. Lysosomal proteolysis in skeletal muscle. Int J Biochem Cell Biol. 2005;37:2098–114.
Kramerova I, Kudryashova E, Venkatraman G, et al. Calpain 3 participates in sarcomere remodeling by acting upstream of the ubiquitin–proteasome pathway. Hum Mol Genet. 2005;14:2125–34.
Williams AB, Decourten-Myers GM, Fischer JE, et al. Sepsis stimulates release of myofilaments in skeletal muscle by a calcium-dependent mechanism. FASEB J. 1999;13:1435–43.
Tidball JG, Spencer MJ. Expression of a calpastatin transgene slows muscle wasting and obviates changes in myosin isoform expression during murine muscle disuse. J Physiol (Lond). 2002;545:819–28.
Belcastro AN, Shewchuk LD, Raj DA. Exercise-induced muscle injury: a calpain hypothesis. Mol Cell Biochem. 1998;179:135–45.
Zhao J, Brault JJ, Schild A, et al. FoxO3 coordinately activates protein degradation by the autophagic/lysosomal and proteasomal pathways in atrophying muscle cells. Cell Metab. 2007;6:472–83.
Capel F, Prod’homme M, Bechet D, et al. Lysosomal and proteasome-dependent proteolysis are differentially regulated by insulin and/or amino acids following feeding in young, mature and old rats. J Nutr Biochem. 2009;20:570–6.
Belizario JE, Lorite MJ, Tisdale MJ. Cleavage of caspases-1, -3, -6, -8 and -9 substrates by proteases in skeletal muscles from mice undergoing cancer cachexia. Br J Cancer. 2001;84:1135–40.
Dargelos E, Poussard S, Brulé C, et al. Calcium-dependent proteolytic system and muscle dysfunctions: a possible role of calpains in sarcopenia. Biochimie. 2008;90:359–68.
Deval C, Mordier S, Obled C, et al. Identification of cathepsin L as a differentially expressed message associated with skeletal muscle wasting. Biochem J. 2001;360:143–50.
Taillandier D, Aurousseau E, Meynial-Denis D, et al. Coordinate activation of lysosomal, Ca 2+-activated and ATP-ubiquitin-dependent proteinases in the unweighted rat soleus muscle. Biochem J. 1996;316:65–72.
Tsujinaka T, Ebisui C, Fujita J, et al. Muscle undergoes atrophy in association with increase of lysosomal cathepsin activity in interleukin-6 transgenic mouse. Biochem Biophys Res Commun. 1995;207:168–74.
Lecker SH, Jagoe RT, Gilbert A, et al. Multiple types of skeletal muscle atrophy involve a common program of changes in gene expression. FASEB J. 2004;18:39–51.
Yamazaki Y, Kamei Y, Sugita S, et al. The cathepsin L gene is a direct target of FOXO1 in skeletal muscle. Biochem J. 2010;427:171–8.
Jagoe RT, Redfern CP, Roberts RG, et al. Skeletal muscle mRNA levels for cathepsin B, but not components of the ubiquitin–proteasome pathway, are increased in patients with lung cancer referred for thoracotomy. ClinSci(Lond). 2002;102:353–61.
Bosutti A, Toigo G, Ciocchi B, et al. Regulation of muscle cathepsin B proteolytic activity in protein-depleted patients with chronic diseases. Clinical nutrition (Edinburgh, Scotland). 2002;21:373–8.
Temparis S, Asensi M, Taillandier D, et al. Increased ATP-ubiquitin-dependent proteolysis in skeletal muscles of tumor-bearing rats. Cancer Res. 1994;54:5568–73.
Matsukura U, Okitani A, Nishimuro T, et al. Mode of degradation of myofibrillar proteins by an endogenous protease, cathepsin L. Biochim Biophys Acta. 1981;662:41–7.
Schwartz W, Bird JW. Degradation of myofibrillar proteins by cathepsins B and D. Biochem J. 1977;167:811–20.
Giannelli G, De Marzo A, Marinosci F, et al. Matrix metalloproteinase imbalance in muscle disuse atrophy. Histol Histopathol. 2005;20:99–106.
Carmeli E, Moas M, Reznick AZ, et al. Matrix metalloproteinases and skeletal muscle: a brief review. Muscle Nerve. 2004;29:191–7.
Reznick AZ, Menashe O, Bar-Shai M, et al. Expression of matrix metalloproteinases, inhibitor, and acid phosphatase in muscles of immobilized hindlimbs of rats. Muscle Nerve. 2003;27:51–9.
Li H, Mittal A, Makonchuk DY, et al. Matrix metalloproteinase-9 inhibition ameliorates pathogenesis and improves skeletal muscle regeneration in muscular dystrophy. Hum Mol Genet. 2009;18:2584–98.
Kumar A, Bhatnagar S, Kumar A. Matrix metalloproteinase inhibitor batimastat alleviates pathology and improves skeletal muscle function in dystrophin-deficient mdx mice. Am J Pathol. 2010;177:248–60.
Flink IL, Morkin E. Sequence of the 20-kilodalton heavy chain peptide from the carboxyl-terminus of bovine cardiac myosin subfragment-1. J ClinInvest. 1984;74:639–46.
Hanan T, Shaklai N. The role of H2O2-generated myoglobin radical in crosslinking of myosin. Free Radic Res. 1995;22:215–27.
Evangelista AM, Rao VS, Filo AR, et al. Direct regulation of striated muscle myosins by nitric oxide and endogenous nitrosothiols. PLoS One. 2010;5:e11209.
Murakami H, Guillet C, Tardif N, et al. Cumulative 3-nitrotyrosine in specific muscle proteins is associated with muscle loss during aging. Exp Gerontol. 2012;47:129–35.
Barreiro E, Hussain SNA. Protein carbonylation in skeletal muscles: impact on function. Antioxid Redox Signal. 2010;12:417–29.
Magherini F, Abruzzo PM, Puglia M, et al. Proteomic analysis and protein carbonylation profile in trained and untrained rat muscles. J Proteomics. 2012;75:978–92.
Shanely RA, Zergeroglu MA, Lennon SL, et al. Mechanical ventilation-induced diaphragmatic atrophy is associated with oxidative injury and increased proteolytic activity. Am J Respir Crit Care Med. 2002;166:1369–74.
Zergeroglu MA, McKenzie MJ, Shanely RA, et al. Mechanical ventilation-induced oxidative stress in the diaphragm. J Appl Physiol. 2003;95:1116–24.
Betters JL, Criswell DS, Shanely RA, et al. Trolox attenuates mechanical ventilation-induced diaphragmatic dysfunction and proteolysis. Am J Respir Crit Care Med. 2004;170:1179–84.
McClung JM, Kavazis AN, Whidden MA, et al. Antioxidant administration attenuates mechanical ventilation-induced rat diaphragm muscle atrophy independent of protein kinase B (PKB Akt) signalling. J Physiol (Lond). 2007;585:203–15.
McClung JM, Whidden MA, Kavazis AN, et al. Redox regulation of diaphragm proteolysis during mechanical ventilation. Am J Physiol Regul Integr Comp Physiol. 2008;294:R1608–17.
Whidden MA, McClung JM, Falk DJ, et al. Xanthine oxidase contributes to mechanical ventilation-induced diaphragmatic oxidative stress and contractile dysfunction. J Appl Physiol. 2009;106:385–94.
Haehling S, Morley JE, Coats AJS, et al. Ethical guidelines for authorship and publishing in the Journal of Cachexia, Sarcopenia and Muscle. J Cachexia Sarcopenia Muscle. 2010;1:7–8.
Ottenheijm CAC, Heunks LMA, Dekhuijzen RPN. Diaphragm adaptations in patients with COPD. Respir Res. 2008;9:12.
Voermans NC, Bönnemann CG, Huijing PA, et al. Clinical and molecular overlap between myopathies and inherited connective tissue diseases. Neuromuscul Disord. 2008;18:843–56.
Ruiz JR, Sui X, Lobelo F, et al. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008;337:a439.
Gale C, Martyn C, Cooper C. Grip strength, body composition, and mortality. International Journal of Epidemiology. 2007;36(1):228–35.
Sui X, Laditka JN, Hardin JW, et al. Estimated functional capacity predicts mortality in older adults. J Am Geriatr Soc. 2007;55:1940–7.
Wind H, Gouttebarge V, Kuijer PPFM, et al. Assessment of functional capacity of the musculoskeletal system in the context of work, daily living, and sport: a systematic review. J Occup Rehabil. 2005;15:253–72.
Cesari M, Leeuwenburgh C, Lauretani F, et al. Frailty syndrome and skeletal muscle: results from the Invecchiare in Chianti study. Am J Clin Nutr. 2006;83:1142–8.
Goodpaster BH, Kelley DE, Thaete FL, et al. Skeletal muscle attenuation determined by computed tomography is associated with skeletal muscle lipid content. J Appl Physiol. 2000;89:104–10.
Pahor M, Manini T, Cesari M. Sarcopenia: clinical evaluation, biological markers and other evaluation tools. The Journal of Nutrition Health and Aging. 2009;13(8):724–8.
Brozek J, Grande F, Anderson JT, et al. Densitometric analysis of body composition: revision of some quantitative assumptions. Ann N Y Acad Sci. 1963;110:113–40.
St-Onge M-P, Wang Z, Horlick M, et al. Dual-energy X-ray absorptiometry lean soft tissue hydration: independent contributions of intra- and extracellular water. Am J Physiol Endocrinol Metab. 2004;287:E842–7.
Kim J, Wang Z, Heymsfield SB, et al. Total-body skeletal muscle mass: estimation by a new dual-energy X-ray absorptiometry method. Am J Clin Nutr. 2002;76:378–83.
Proctor DN, O’Brien PC, Atkinson EJ, et al. Comparison of techniques to estimate total body skeletal muscle mass in people of different age groups. Am J Physiol. 1999;277:E489–95.
Kyle UG, Bosaeus I, De Lorenzo AD, et al. Bioelectrical impedance analysis—part I: review of principles and methods. Clinical nutrition (Edinburgh, Scotland). 2004;23:1226–43.
Reeves ND, Maganaris CN, Narici MV. Ultrasonographic assessment of human skeletal muscle size. Eur J Appl Physiol. 2004;91:116–8.
Fuller N, Hardingham C, Graves M, et al. Predicting composition of leg sections with anthropometry and bioelectrical impedance analysis, using magnetic resonance imaging as reference. Clinical Science. 1999;96(6):647–57.
Rolland Y, Lauwers-Cances VR, Cournot M, et al. Sarcopenia, calf circumference, and physical function of elderly women: a cross-sectional study. J Am Geriatr Soc. 2003;51:1120–4.
Heymsfield S, McManus C, Smith J. Anthropometric measurement of muscle mass: revised equations for calculating bone-free arm muscle area. Am J Clin Nutr. 1982;36(4):680–90.
Calles-Escandon J, Cunningham JJ, Snyder P, et al. Influence of exercise on urea, creatinine, and 3-methylhistidine excretion in normal human subjects. Am J Physiol. 1984;246:E334–8.
Rennie MJ, Phillips S, Smith K. Reliability of results and interpretation of measures of 3-methylhistidine in muscle interstitium as marker of muscle proteolysis. J Appl Physiol. 2008;105:1380–1. authorreply1382–3.
Millward DJ, Bates PC, Grimble GK, et al. Quantitative importance of non-skeletal-muscle sources of N tau-methylhistidine in urine. Biochem J. 1980;190:225–8.
Tesch PA, von Walden F, Gustafsson T, et al. Skeletal muscle proteolysis in response to short-term unloading in humans. J Appl Physiol. 2008;105:902–6.
Smith IJ, Dodd SL. Calpain activation causes a proteasome-dependent increase in protein degradation and inhibits the Akt signalling pathway in rat diaphragm muscle. Exp Physiol. 2007;92:561–73.
Enns DL, Raastad T, Ugelstad I, et al. Calpain/calpastatin activities and substrate depletion patterns during hindlimb unweighting and reweighting in skeletal muscle. Eur J Appl Physiol. 2007;100:445–55.
Bartoli M, Richard I. Calpains in muscle wasting. Int J Biochem Cell Biol. 2005;37:2115–33.
Smith IJ, Lecker SH, Hasselgren P-O. Calpain activity and muscle wasting in sepsis. Am J Physiol Endocrinol Metab. 2008;295:E762–71.
Murphy RM, Goodman CA, McKenna MJ, et al. Calpain-3 is autolyzed and hence activated in human skeletal muscle 24 h following a single bout of eccentric exercise. J Appl Physiol. 2007;103:926–31.
Guyon JR, Kudryashova E, Potts A, et al. Calpain 3 cleaves filamin C and regulates its ability to interact with gamma- and delta-sarcoglycans. Muscle Nerve. 2003;28:472–83.
Du J, Wang X, Miereles C, et al. Activation of caspase-3 is an initial step triggering accelerated muscle proteolysis in catabolic conditions. J ClinInvest. 2004;113:115–23.
Byun Y, Chen F, Chang R, et al. Caspase cleavage of vimentin disrupts intermediate filaments and promotes apoptosis. Cell Death Differ. 2001;8:443–50.
Chen F, Chang R, Trivedi M, et al. Caspase proteolysis of desmin produces a dominant-negative inhibitor of intermediate filaments and promotes apoptosis. J Biol Chem. 2003;278:6848–53.
Pereira AMM, Strasberg-Rieber M, Rieber M. Invasion-associated MMP-2 and MMP-9 are up-regulated intracellularly in concert with apoptosis linked to melanoma cell detachment. Clin Exp Metastasis. 2005;22:285–95.
Mort JS, Recklies AD, Poole AR. Extracellular presence of the lysosomal proteinase cathepsin B in rheumatoid synovium and its activity at neutral pH. Arthritis Rheum. 1984;27:509–15.
Premzl A, Zavasnik-Bergant V, Turk V, et al. Intracellular and extracellular cathepsin B facilitate invasion of MCF-10A neoT cells through reconstituted extracellular matrix in vitro. Exp Cell Res. 2003;283:206–14.
Poole AR, Hembry RM, Dingle JT. Cathepsin D in cartilage: the immunohistochemical demonstration of extracellular enzyme in normal and pathological conditions. J Cell Sci. 1974;14:139–61.
Poole AR, Hembry RM, Dingle JT, et al. Proceedings: extracellular release of cathepsin D from cells in human normal and rheumatoid. Ann Rheum Dis. 1974;33:405–6.
Johnson P, Lobley GE, Perry SV. Distribution and biological role of 3-methyl-histidine in actin and myosin. Biochem J. 1969;114:34P.
Fedorova M, Kuleva N, Hoffmann R. Identification, quantification, and functional aspects of skeletal muscle protein-carbonylation in vivo during acute oxidative stress. J Proteome Res. 2010;9:2516–26.
Conflict of interest
All of the authors are employed at Nordic Bioscience whose chief business is research in and development of serum biomarkers of progressive degenerative diseases like osteoarthritis, osteoporosis and alzhimers. Morten Asser Karsdal also owns stocks in Nordic Bioscience.
Ethical guidelines
The authors accept the ethical guidelines presented for this journal and hereby verify that the present paper is in agreement with said ethical guidelines [80] and by extension the Vancouver guidelines governing rules of authorship.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Nedergaard, A., Karsdal, M.A., Sun, S. et al. Serological muscle loss biomarkers: an overview of current concepts and future possibilities. J Cachexia Sarcopenia Muscle 4, 1–17 (2013). https://doi.org/10.1007/s13539-012-0086-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13539-012-0086-2