
Abstract
Background
Intramyocellular lipids are an important source of fuel for mitochondrial fat oxidation and play an important role in intramuscular lipid homeostasis. We hypothesised that due to the phenotype associated with cancer cachexia, there would exist an association between increasing weight loss and the number/size of intramyocellular lipid droplets.
Methods
Nineteen cancer patients and 6 controls undergoing surgery were recruited. A rectus abdominis biopsy was performed and processed for transmission electron microscopy (TEM). The number of intramyocellular lipid droplets and lipid droplet diameter were calculated from the TEM images. CT scans, performed as part of patients' routine care, were analysed to determine amount of adipose (intermuscular, visceral and subcutaneous) and muscle tissue.
Results
Compared with controls, cancer patients had increased numbers of lipid droplets (mean (SD) 1.8 (1.9) vs. 6.4 (9.1) per ×2,650 field, respectively, p = 0.036). Mean (SD) lipid droplet diameter was also higher in cancer patients compared with controls (0.42 (0.13) vs. 0.24 (0.21) μm, p = 0.015). Mean lipid droplet count correlated positively with the severity of weight loss (R = 0.51, p = 0.025) and negatively with CT-derived measures of intermuscular fat (R = −0.53, p = 0.022) and visceral fat (R = −0.51, p = 0.029).
Conclusions
This study suggests that the number and size of intramyocellular lipid droplets is increased in the presence of cancer and increases further with weight loss/loss of adipose mass in other body compartments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Background
Cachexia continues to represent a therapeutic challenge in cancer patients. The syndrome is a complex process characterised by weight loss and is associated with increased morbidity and mortality [1, 2]. Whilst both lean and adipose tissue become depleted, there is evidence that body fat is lost more rapidly than lean tissue [3]. The drivers of lipolysis or possibly reduced lipogenesis [4] in cancer cachexia are still to be elucidated fully. However, TNFα [5], ZAG [6, 7] and MIC-1 [8] have been suggested as potential mediators. Adipose tissue is composed predominately of stored lipid droplets [9] and is intimately involved with energy homeostasis and metabolism through secreted adipokines [10]. Additionally, it influences insulin sensitivity, affects immune and inflammatory pathways and interacts with catecholamines [11, 12]. The catabolism of lipids generates fatty acids that can either be utilised by skeletal muscle or further metabolised to take part in the Krebs cycle [9]. Triglyceride-containing lipid droplets are dynamic organelles stored on demand in all cells and grow through a fusion process mediated by SNARE proteins, including SNAP23 [13]. Within skeletal muscle, it is thought that intramyocellular lipid/lipid droplets act as fuel stores for mitochondrial fat oxidation [14]. Lipid droplets are usually in direct contact with mitochondria presumably to allow rapid transport when required in situations such as exercise [14]. Indeed, intramyocellular lipid decreases upon acute exercise [15–18] and almost completely disappears after marathon running [19, 20]. Conversely, physical inactivity and a diet excessive in fats can lead to an increase in intramyocellular lipid [18]. Endurance training causes a rise in intramyocellular lipid content supporting the role of lipid droplets as an energy source during physical activity [14]. Although the presence of lipid droplets in skeletal muscle is part of the normal physiology of healthy individuals with or without physical training, associations have been shown between increased droplet number and pathological states such as the presence of type 2 diabetes/insulin resistance [14, 21] and ageing [22]. With ageing, not only are numbers of lipid droplets increased, but their association with mitochondria appears to be disrupted [22] and mitochondrial function is altered [23, 24]. In the morbidly obese, raised intramyocellular lipid content has been reported to be associated with insulin resistance and to decrease after weight loss/bariatric surgery [25, 26]. In patients with gastrointestinal cancer, increased levels of intramyocellular lipid have also been reported. Using magnetic resonance spectroscopy, a 35% higher level of intramyocellular lipids was observed in patients with cachexia (defined by >10% weight loss in previous 6 months) compared with weight-stable cancer patients [27].
We sought to carry out a quantitative morphological examination of lipid droplets in human cancer-associated weight loss using electron microscopy. We hypothesised that due to the phenotype associated with cancer cachexia (lipid mobilisation, insulin resistance [4], systemic inflammation [28], sarcopenia [29] and reduced physical activity [30]), there would be an association between increasing weight loss and the number/size of intra-myocellular lipid droplets. Additionally, we examined the relationship between lipid droplets, anthropometry and/or CT-derived body composition measures.
2 Methods
2.1 Participants
Patients (n = 19) were recruited using the following inclusion criteria: diagnosis of upper gastrointestinal (oesophageal, gastric, pancreatic) cancer, undergoing potentially curative surgery, age 18–85. Patients were excluded if they had metastatic disease, were undergoing palliative surgery or were knowingly taking anabolic/catabolic agents. There were no patients with uncontrolled diabetes or known thyroid disorders. Three patients had completed a course of neoadjuvant chemotherapy, but were not undertaking chemotherapy at the time of surgery. A group of weight-stable patients undergoing elective abdominal surgery for benign conditions participated as controls (n = 6). All procedures were approved by the local research ethics committee. Written informed consent was obtained. The study conformed to the standards set by the Declaration of Helsinki.
2.2 Anthropometry, weight loss and performance status
Body weight was measured with subjects in light clothing using a beam scale (Seca, UK). Height was measured using a standard wall-mounted measure. Triceps skin fold (TSF) thickness (callipers, Holtain Ltd Crymych, UK) and mid-arm circumference (MAC) were measured to calculate mid-arm muscle circumference (MAMC). Arm muscle CSA was calculated according to the equation: \( \left( {{\text{MAC}} - \pi \times {\text{TS}}{{\text{F}}^{{2}}}/{4}\pi } \right) - {1}0\left( {\text{male}} \right) \) and \( \left( {{\text{MAC}} - \pi \times {\text{TS}}{{\text{F}}^{{2}}}/{4}\pi } \right) - {6}.{5}\left( {\text{female}} \right) \) [31]. The patients' clinical details were recorded and degree of weight loss from self-reported pre-illness stable weight documented. Karnofsky performance score was assessed in each patient by a single observer.
2.3 Blood measures
A fasting venous blood sample was taken on the morning of surgery. CRP was measured in all patients. A CRP ≥5 mg/l (the upper limit of normal in our lab) was considered consistent with the presence of systemic inflammation. Due to the limited availability of raw plasma samples, the other blood measures were performed in a subset of patients (albumin n = 18, insulin n = 13, glucose n = 14, cortisol n = 17, homeostatic model assessment of insulin resistance (HOMA-IR) n = 10, cortisol/insulin ratio n = 17). All samples were processed in the Department of Clinical Chemistry, Royal Infirmary, Edinburgh (fully accredited by Clinical Pathology Accreditation Ltd, UK) using standard automated methods.
2.4 Muscle biopsy and transmission electron microscopy (TEM)
All biopsies were taken at the start of open abdominal surgery under general anaesthesia. Patients had undergone an overnight fast. The edge of the rectus abdominis was exposed and a 1-cm3 specimen removed using sharp dissection. A small section was cut and fixed in 3% glutaraldehyde in 0.1 M sodium cacodylate buffer, pH 7.3, for 2 h then washed in three 10-min changes of 0.1 M sodium cacodylate. Specimens were then post-fixed in 1% osmium tetroxide in 0.1 M sodium cacodylate for 45 min and washed in three 10-min changes of 0.1 M sodium cacodylate buffer. These sections were then dehydrated in 50%, 70%, 90% and 100% normal grade acetones for 10 min each, then for a further two 10-min changes in analar acetone. Samples were then embedded in Araldite resin. Sections, 1-μm thick, were cut on a Reichert OMU4 ultramicrotome (Leica Microsystems (UK) Ltd, Milton Keynes), stained with toluidine blue and viewed in a light microscope to select suitable areas for investigation. Ultrathin sections, 60-nm thick were cut from selected areas, stained in uranyl acetate and lead citrate, then viewed in a Phillips CM120 transmission electron microscope (FEI UK Ltd, Cambridge, England). A Gatan Orius CCD camera (Gatan UK, Oxon, England) set at ×2,650 magnification was used to capture images. Photographs were taken at random, and lipid droplets were counted manually (by one observer blinded to the patient diagnosis) in at least two fields per patient and the average count recorded. The diameter of each visible lipid droplet was measured in micrometre using ImageJ and the mean lipid droplet diameter calculated for each patient. Identified lipid droplets were examined at high magnification (×11,000) to ensure the absence of a double membrane, thus distinguishing them from vacuolated giant mitochondria [32].
2.5 CT-based body composition analysis
CT scans were performed as part of the cancer patients' routine management but were not available for the benign controls. The CSA of adipose tissue (comprising subcutaneous, visceral and intermuscular) and muscle was measured at the level of the third lumbar vertebrae (L3). Adipose and muscle CSA measured at L3 are linearly related to whole body values [33]. All images were analysed by a single trained observer with SliceOmatic V4.3 software (Tomovision, Montreal, Canada) which enables specific tissue demarcation using Hounsfield unit (HU) thresholds. The HU ranges used were −29 to +150 for skeletal muscle [34], −190 to −30 for subcutaneous and intramuscular adipose tissue [35] and −150 to −50 for visceral adipose tissue [36]. Tissue boundaries were corrected manually if required. CSAs (square centimetres) were computed automatically by summing tissue pixels, multiplying by pixel surface area and subsequently normalised for stature (square centimetres per square metre).
2.6 Statistical analysis
SPSS v15.0 statistical software was used for data analysis. Student's two-tailed t test was used to compare means between groups. Variables are reported as mean ± standard deviation (SD) unless otherwise stated. The Mann–Whitney test was used for non-parametric analysis. Data were log-transformed when appropriate. Associations between variables were evaluated using Pearson's correlation (bivariate) analysis. Statistical significance was set at a p value (two tailed) of <0.05.
3 Results
Nineteen cancer patients (11 men, 8 women) and 6 controls (2 men, 4 women) were recruited. Demographics are shown in Table 1. Eight patients had pancreatic cancer, four gastric, three oesophageal, three oesophagogastric junctions and one patient with small bowel cancer. The mean body mass index (BMI) of both the cancer patient and control groups was >25. Cancer patients were older than controls (mean age (standard deviation) 67 (10) vs. 53 (8) years, respectively, p = 0.005) and had a significantly higher percentage weight loss (6.0% (7.1%) vs. −0.3% (1.4%), respectively, p = 0.002). Mid-arm muscle circumference (MAMC) and arm muscle cross-sectional area (CSA) were not significantly different between controls and cancer patients. There was a trend towards higher Karnofsky performance scores in controls compared with cancer patients (98.3 (3.1) vs. 91.7 (8.6), p = 0.083). Significantly more cancer patients exhibited systemic inflammation (C-reactive protein (CRP) ≥5 mg/l) than controls (n = 11/19 vs. 0/6, respectively, p = 0.020 Fisher's exact test). Both the average lipid droplet number (6.4 (9.1) vs. 1.8 (1.9), p = 0.036, see also Fig. 1) and the average lipid droplet diameter (0.42 (0.13) vs. 0.24 (0.21) μm, p = 0.015) were higher in the cancer cohort compared with controls.

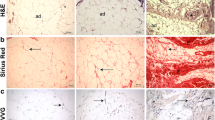
Representative electron micrographs for controls and cancer patients. a. Images are all at ×2,650 magnification. Greater numbers of lipid droplets (white vacuoles) were evident with increasing weight loss. Percent (%) values for cancer patients refer to weight change from pre-illness stable weight. Bars represent 2 μm. b. ×11,000 magnification image of a lipid droplet demonstrating the absence of double membranes, thus distinguishing it from vacuolated giant mitochondria [36]
3.1 Changes associated with increasing weight loss/altered body composition in the cancer patients
In the cancer patients, percentage weight loss (range −10.4% to 17.1%) correlated negatively with mid-arm circumference (R = −0.51, p = 0.024) and MAMC (R = −0.46, p = 0.047), and there was a trend towards a reduction in arm muscle CSA (R = −0.44, p = 0.058). There were, however, no significant correlations between percentage weight loss and CT-derived values of muscle mass. CT-derived measures of intermuscular and visceral fat were not significantly associated with weight loss, but there was a trend towards a (negative) association between weight loss and subcutaneous fat (R = −0.42, p = 0.082). Percentage weight loss correlated negatively with albumin (R = −0.56, p = 0.015), but there were no significant associations with CRP (R = 0.15, p = 0.549), insulin (R = −0.32, p = 0.280), glucose (R = 0.19, p = 0.509), cortisol (R = −0.27, p = 0.295), HOMA-IR (R = −0.18, p = 0.614) or cortisol/insulin ratio (R = 0.44, p = 0.137).
The average lipid droplet number correlated positively with percentage weight loss (R = 0.51, p = 0.025, Fig. 2), but there was no relationship between weight loss and lipid droplet diameter (R = 0.15, p = 0.535). MAMC, arm muscle CSA and CT-derived muscle mass did not correlate significantly with either lipid droplet count or lipid droplet diameter. Both weight (R = −0.61, p = 0.007) and BMI (R = −0.46, p = 0.050) correlated negatively with the number of lipid droplets. There were significantly greater numbers of lipid droplets in patients with lower CT-derived measures of intermuscular fat (R = −0.53, p = 0.022) and visceral fat (R = −0.51, p = 0.029), and there was also a trend towards an association between droplet number and subcutaneous fat (R = −0.46, p = 0.055). No relationship was demonstrated between patients' age and number of lipid droplets (R = −0.30, p = 0.209) or between the number of lipid droplets and the lipid droplet diameter (R = 0.34, p = 0.152). There were no significant associations between the number of lipid droplets and plasma levels of albumin (R = −0.28, p = 0.256), CRP (R = −0.10, p = 0.695), insulin (R = −0.26, p = 0.391), glucose (R = −0.03, p = 0.926), cortisol (R = −0.13, p = 0.633), HOMA-IR (R = −0.38, p = 0.280) or cortisol/insulin ratio (R = 0.09, p = 0.783).

Percentage weight loss versus lipid droplet number. There was a significant positive correlation between percentage weight loss and LD number (R = 0.51, p = 0.025; Pearson's correlation, two tailed). There was no significant difference in LD number according to tumour site (one-way ANOVA, p = 0.559). LD lipid droplet
4 Discussion
The current study demonstrates a progressive rise in the number of intramyocellular lipid droplets in relation to both increasing weight loss and depletion of adipose tissue mass in patients with cancer. In addition, the presence of cancer was associated with increased lipid droplet numbers compared with controls. Thus, the presence of increased intramyocellular lipid droplets does not seem to be related exclusively to weight loss but rather is probably linked to the mediators of the processes underlying such weight loss (which is variably expressed depending on the individual patient). Increasing weight loss, however, does seem to exacerbate the observed changes in ultrastructure.
Patients with obesity have increased intramyocellular lipid droplets [37], whereas we observed a paradoxical negative association between BMI and number of lipid droplets: that is, the lower the BMI, the higher the number of lipid droplets. These findings suggest that increased intramyocellular lipid droplets are not specific to either a net positive or negative energy balance but may relate to the underlying causes of shifts in energy balance.
Consistent with the above hypothesis, we observed significant negative associations between CT-derived measures of fat mass (intermuscular, visceral and subcutaneous) and the number of intramyocellular lipid droplets. This would suggest that the changes within the myocytes were not related exclusively to local (skeletal muscle) events but rather to the overall state of net lipid mobilisation and negative energy balance or perhaps endocrine disruption.
The size of lipid droplets as well as their number may be physiologically significant. However, in the present study, although the average number of lipid droplets increased with progressive weight loss, there was no association between weight loss and lipid droplet diameter. This could represent the lipid droplets reaching a plateau of growth or may simply be due to their being a wide variability in lipid droplet diameter.
The cancer patients in the present study were overweight (mean BMI > 25) and this probably reflects not only the increasing level of obesity in the general population, but that obesity is a risk factor for the development of cancer. It is important to recognise that underneath this mantle of fat, there may be clinically occult muscle wasting. Indeed, in the present study, there was an association between increasing weight loss and reduced mid-arm muscle circumference (an anthropometric index of whole body muscle mass). The trend towards sarcopenic obesity in advanced cancer patients has recently been emphasised [38]. Indeed, in a recent study of patients with advanced pancreatic cancer, we demonstrated sarcopenic obesity to be an independent determinant of reduced survival [29]. In the present study, we were not able to relate either anthropometric or CT-derived measures of muscle mass to the number of intramyocellular lipid droplets, but this probably reflects the relatively small sample size and the absence of pre-illness measures of muscle mass from which to estimate net loss. In future studies, it would be important to characterise further the likely parallel between metabolic syndrome, the cancer patient with sarcopenic obesity and the mechanisms that underlie the present observed changes in skeletal muscle ultrastructure.
The controls in the current study were younger than the cancer patients. It has been suggested that ageing results in an increase in intramyocellular lipid content [22]. Whilst this may be a contributing factor to the lower numbers of lipid droplets in the control group, the observed association between weight loss and lipid droplets in the cancer cohort was independent of age. Likewise, we did not observe differences in lipid droplet numbers between men and women (p = 0.630) or tumour site (one-way ANOVA, p = 0.559; see also Fig. 2). However, given that the numbers in each group were small, the influence of these factors would be better explored in a larger dataset.
The likely mechanism for the increased deposition of lipid within the skeletal muscle of weight-losing cancer patients probably reflects an imbalance between fatty acid supply and utilisation. The enhanced lipolysis in cancer cachexia has been long established. However, recent research has focused more closely on mitochondrial dysfunction and, as observed in sepsis [39], impaired mitochondrial fatty acid oxidation/oxidative capacity may contribute to lipid accumulation. Of interest, mitochondrial derangement has been demonstrated in COPD muscle wasting [40]. The present study did not extend to a detailed evaluation of myocellular mitochondrial ultrastructure or function, but clearly, this could be the focus of further research.
5 Conclusions
In summary, this study suggests that the presence of lipid droplets is related to the presence of cancer and increases with weight loss. The specific mechanisms/drivers of this phenomenon remain to be elucidated.
References
Dodson S, Baracos VE, Jatoi A, Evans WJ, Cella D, Dalton JT, et al. Muscle wasting in cancer cachexia: clinical implications, diagnosis, and emerging treatment strategies. Annu Rev Med. 2011;62:265–79.
Bossola M, Pacelli F, Tortorelli A, Doglietto GB. Cancer cachexia: it's time for more clinical trials. Ann Surg Oncol. 2007;14:276–85.
Fouladiun M, Korner U, Bosaeus I, Daneryd P, Hyltander A, Lundholm KG. Body composition and time course changes in regional distribution of fat and lean tissue in unselected cancer patients on palliative care–correlations with food intake, metabolism, exercise capacity, and hormones. Cancer. 2005;103:2189–98.
Tisdale MJ. Mechanisms of cancer cachexia. Physiol Rev. 2009;89:381–410.
Plomgaard P, Fischer CP, Ibfelt T, Pedersen BK, van Hall G. Tumor necrosis factor-alpha modulates human in vivo lipolysis. J Clin Endocrinol Metab. 2008;93:543–9.
Bing C, Bao Y, Jenkins J, Sanders P, Manieri M, Cinti S, et al. Zinc-alpha2-glycoprotein, a lipid mobilizing factor, is expressed in adipocytes and is up-regulated in mice with cancer cachexia. Proc Natl Acad Sci USA. 2004;101:2500–5.
Mracek T, Stephens NA, Gao D, Bao Y, Ross JA, Ryden M, et al. Enhanced ZAG production by subcutaneous adipose tissue is linked to weight loss in gastrointestinal cancer patients. Br J Cancer. 2011;104:441–7.
Ding Q, Mracek T, Gonzalez-Muniesa P, Kos K, Wilding J, Trayhurn P, et al. Identification of macrophage inhibitory cytokine-1 in adipose tissue and its secretion as an adipokine by human adipocytes. Endocrinology. 2009;150:1688–96.
Finn PF, Dice JF. Proteolytic and lipolytic responses to starvation. Nutrition. 2006;22:830–44.
Wang P, Mariman E, Renes J, Keijer J. The secretory function of adipocytes in the physiology of white adipose tissue. J Cell Physiol. 2008;216:3–13.
Balistreri CR, Caruso C, Candore G. The role of adipose tissue and adipokines in obesity-related inflammatory diseases. Mediat Inflamm. 2010;201:802078.
Lafontan M. Advances in adipose tissue metabolism. Int J Obes Lond. 2008;32 Suppl 7:S39–51.
Jagerstrom S, Polesie S, Wickstrom Y, Johansson BR, Schroder HD, Hojlund K, et al. Lipid droplets interact with mitochondria using SNAP23. Cell Biol Int. 2009;33:934–40.
Schrauwen-Hinderling VB, Hesselink MK, Schrauwen P, Kooi ME. Intramyocellular lipid content in human skeletal muscle. Obes Silver Spring. 2006;14:357–67.
Krssak M, Petersen KF, Bergeron R, Price T, Laurent D, Rothman DL, et al. Intramuscular glycogen and intramyocellular lipid utilization during prolonged exercise and recovery in man: a 13C and 1H nuclear magnetic resonance spectroscopy study. J Clin Endocrinol Metab. 2000;85:748–54.
Decombaz J, Schmitt B, Ith M, Decarli B, Diem P, Kreis R, et al. Postexercise fat intake repletes intramyocellular lipids but no faster in trained than in sedentary subjects. Am J Physiol Regul Integr Comp Physiol. 2001;281:R760–9.
Rico-Sanz J, Moosavi M, Thomas EL, McCarthy J, Coutts GA, Saeed N, et al. In vivo evaluation of the effects of continuous exercise on skeletal muscle triglycerides in trained humans. Lipids. 2000;35:1313–8.
Shaw CS, Clark J, Wagenmakers AJ. The effect of exercise and nutrition on intramuscular fat metabolism and insulin sensitivity. Annu Rev Nutr. 2010;30:13–34.
Staron RS, Hikida RS, Murray TF, Hagerman FC, Hagerman MT. Lipid depletion and repletion in skeletal muscle following a marathon. J Neurol Sci. 1989;94:29–40.
Kayar SR, Hoppeler H, Howald H, Claassen H, Oberholzer F. Acute effects of endurance exercise on mitochondrial distribution and skeletal muscle morphology. Eur J Appl Physiol Occup Physiol. 1986;54:578–84.
Bostrom P, Andersson L, Li L, Perkins R, Hojlund K, Boren J, et al. The assembly of lipid droplets and its relation to cellular insulin sensitivity. Biochem Soc Trans. 2009;37:981–5.
Crane JD, Devries MC, Safdar A, Hamadeh MJ, Tarnopolsky MA. The effect of aging on human skeletal muscle mitochondrial and intramyocellular lipid ultrastructure. J Gerontol A Biol Sci Med Sci. 2010;65:119–28.
Conley KE, Jubrias SA, Esselman PC. Oxidative capacity and ageing in human muscle. J Physiol. 2000;526(Pt 1):203–10.
Trounce I, Byrne E, Marzuki S. Decline in skeletal muscle mitochondrial respiratory chain function: possible factor in ageing. Lancet. 1989;1:637–9.
Gray RE, Tanner CJ, Pories WJ, MacDonald KG, Houmard JA. Effect of weight loss on muscle lipid content in morbidly obese subjects. Am J Physiol Endocrinol Metab. 2003;284:E726–32.
Greco AV, Mingrone G, Giancaterini A, Manco M, Morroni M, Cinti S, et al. Insulin resistance in morbid obesity: reversal with intramyocellular fat depletion. Diabetes. 2002;51:144–51.
Weber MA, Krakowski-Roosen H, Schroder L, Kinscherf R, Krix M, Kopp-Schneider A, et al. Morphology, metabolism, microcirculation, and strength of skeletal muscles in cancer-related cachexia. Acta Oncol. 2009;48:116–24.
Stephens NA, Skipworth RJ, Fearon KC. Cachexia, survival and the acute phase response. Curr Opin Support Palliat Care. 2008;2:267–74.
Tan BH, Birdsell LA, Martin L, Baracos VE, Fearon KC. Sarcopenia in an overweight or obese patient is an adverse prognostic factor in pancreatic cancer. Clin Cancer Res. 2009;15:6973–9.
Moses AW, Slater C, Preston T, Barber MD, Fearon KC. Reduced total energy expenditure and physical activity in cachectic patients with pancreatic cancer can be modulated by an energy and protein dense oral supplement enriched with n-3 fatty acids. Br J Cancer. 2004;90:996–1002.
Heymsfield SB, McManus C, Smith J, Stevens V, Nixon DW. Anthropometric measurement of muscle mass: revised equations for calculating bone-free arm muscle area. Am J Clin Nutr. 1982;36:680–90.
Gdynia G, Keith M, Kopitz J, Bergmann M, Fassl A, Weber AN, et al. Danger signaling protein HMGB1 induces a distinct form of cell death accompanied by formation of giant mitochondria. Cancer Res. 2010;70:8558–68.
Mourtzakis M, Prado CM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab. 2008;33:997–1006.
Mitsiopoulos N, Baumgartner RN, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol. 1998;85:115–22.
Kvist H, Sjostrom L, Tylen U. Adipose tissue volume determinations in women by computed tomography: technical considerations. Int J Obes. 1986;10:53–67.
Vehmas T, Kairemo KJ, Taavitsainen MJ. Measuring visceral adipose tissue content from contrast enhanced computed tomography. Int J Obes Relat Metab Disord. 1996;20:570–3.
van Loon LJ, Koopman R, Manders R, van der Weegen W, van Kranenburg GP, Keizer HA. Intramyocellular lipid content in type 2 diabetes patients compared with overweight sedentary men and highly trained endurance athletes. Am J Physiol Endocrinol Metab. 2004;287:E558–65.
Prado CM, Lieffers JR, McCargar LJ, Reiman T, Sawyer MB, Martin L, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008;9:629–35.
Fredriksson K, Tjader I, Keller P, Petrovic N, Ahlman B, Scheele C, et al. Dysregulation of mitochondrial dynamics and the muscle transcriptome in ICU patients suffering from sepsis induced multiple organ failure. PLoS ONE. 2008;3:e3686.
Gosker HR, Hesselink MK, Duimel H, Ward KA, Schols AM. Reduced mitochondrial density in the vastus lateralis muscle of patients with COPD. Eur Respir J. 2007;30:73–9.
von Haehling S, Morley JE, Coats AJ, Anker SD. Ethical guidelines for authorship and publishing in the Journal of Cachexia, Sarcopenia and Muscle. J Cachexia Sarcopenia Muscle. 2010;1:7–8.
Acknowledgements
We are grateful to the consultant oesophagogastric and hepatobiliary surgeons at the Royal Infirmary of Edinburgh for assistance with patient recruitment and muscle biopsies and Stephen Mitchell at the University of Edinburgh for his help with the sample preparation, processing and use of transmission electron microscopy facilities. This study was supported by Cancer Research UK (grant no. C1128/A7309).
The authors of this manuscript certify that they complied with the Ethical guidelines for authorship and publishing in the Journal of Cachexia, Sarcopenia and Muscle [41].
Conflict of interest
None of the authors have declared any competing interests.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Stephens, N.A., Skipworth, R.J.E., MacDonald, A.J. et al. Intramyocellular lipid droplets increase with progression of cachexia in cancer patients. J Cachexia Sarcopenia Muscle 2, 111–117 (2011). https://doi.org/10.1007/s13539-011-0030-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13539-011-0030-x