
Abstract
Researchers and policymakers often rely on the infant mortality rate as an indicator of a country’s health. Despite arguments about its relevance, uniform measurement of infant mortality is necessary to guarantee its use as a valid measure of population health. Using important socioeconomic indicators, we develop a novel method to adjust country-specific reported infant mortality figures. We conclude that an augmented measure of mortality that includes both infant and late fetal deaths should be considered when assessing levels of social welfare in a country. In addition, mortality statistics that exhibit a substantially high ratio of late fetal to early neonatal deaths should be more closely scrutinized.




Similar content being viewed by others


Notes
These calculations use World Bank data from the period 2001–2011, which is the most recent decade for which GDP and IMR data are available for both Cuba and OECD countries. Specifically, average GDP per capita in constant 2005 U.S. dollars is $4,077 (Cuba) and $35,844 (OECD), and average IMR is 5.45 (Cuba) and 4.28 (OECD). Using purchasing power parity–adjusted GDP per capita, the ratio of GDP per capita between OECD countries and Cuba, and that of the United States and Cuba, is 2.39 and 3.22, respectively.
Refer to the Data and Definitions section for definitions of late fetal and early neonatal deaths.
Throughout this study, we use the fetus weight (rather than the gestational age) as the classification criteria for late fetal deaths. Hence, a death of a fetus weighing 500 g or more constitutes a late fetal death.
Following the ICD-10 definitions, the late fetal mortality rate (LFMR) uses total births (live births + fetal deaths) instead of live births only.
A follow-up study describes these deaths for the year 2004 (World Health Organization, WHO 2007).
The definition of a live birth varies greatly from country to country and even within countries. For example, some countries declare a live birth only if the newborn weighs at least 500 g or if the gestational age is at least 22 weeks, while other countries might have no lower limit on classifications of live births.
For more information on data collection for each country, refer to the European Perinatal Health Report prepared by the EURO-PERISTAT (2008) project.
In the case of fetal deaths, most PERISTAT countries use a cutoff for their classifications of at least 500 g or 22 weeks of gestation as recommended by the WHO ICD-10 definitions. In the case of live births, most countries did not have a limit on weight or gestational age in their classifications.
Data for the United Kingdom is divided into three regions: England and Wales, Northern Ireland, and Scotland. In this analysis, we exclude France because of an obvious disparity in the reported live births and fetal deaths (i.e., only 14,737 live births are reported when, according to other sources, there were more than 700,000). Cyprus and Greece were excluded because of missing comparable information on fetal deaths.
Similar to PERISTAT countries, Cuba reports all deaths of fetuses weighting at least 500 g. In the case of live births, it is not clear from the Anuario Estadístico de Salud (2010) whether very LBW and extremely LBW births are included in their classification. However, the definition of live births does not play a significant part in the correction of mortality statistics presented in this article.
Stillbirths are equivalent to late fetal deaths.
A 2004 follow-up study by the same organization found that the average LFMR and ENMR across various world regions are very similar. For example, the average LFMR and ENMR for Africa were 28 and 29, respectively; for Asia, 25 and 23; for Latin America and the Caribbean, 8 and 10; for Europe, 5 and 4; and for North America, 3 and 3.
Recall that the WHO study states that the LFD should equal or, more likely, exceed the END.
Refer to Online Resource 1, Fig. S1, for the LFD-END ratio for Cuba between 1996 and 2012, along with LFDs and ENDs.
See Belanger and Flynn (2009) for a discussion of abortions and state-sponsored abortion policies in Cuba.
An alternative point of concern is that PERISTAT countries might classify LTAs as LFDs. In the case of PERISTAT countries, there is very little indication that they include LTAs as part of LFDs. According to the report, most countries used the WHO’s ICD-10 definition as well. However, it is important to highlight that even if PERISTAT countries include LTAs in their LFDs, the results presented in this article are valid because Cuba’s LFD-END ratio is an outlier even when PERISTAT countries’ ratios are artificially inflated by the inclusion of LTAs. See footnote 30 for a detailed explanation of this aspect after discussing the empirical methodology.
This expands on the idea presented in Gonzalez (2015).
Table S2 in Online Resource 1 provides a detailed description of these determinants.
Hemminki and Rimpela (1991) and Singh et al. (1997) provided examples of studies where LBW is clearly associated with anemic women. Other studies, such as Tamura et al. (1996) and Rondo et al. (1997), showed a positive association between preterm delivery (an important determinant of fetal deaths) and the incidence of anemia in mothers. See Allen (2000) for a survey of the detrimental effects of anemia on pregnancy outcomes. In the case of adolescent pregnancy, Olausson et al. (1999) found that the risk of neonatal mortality is significantly increased for mothers aged 13–17 relative to mothers aged 20–24. The rates of very preterm births are also significantly higher for the former age group relative to the latter. In the case of maternal mortality, Anderson et al. (2007) found in Haiti that after a maternal death, the likelihood of experiencing the loss of the child is approximately 55 %. In the case of abortions, we want to capture the possibility that abortions may affect LFDs in cases where LTAs may be classified as LFDs. We thank an anonymous referee for this suggestion.
Refer to Online Resource 1 for further discussion of the choice of dependent variable and the functional form for Eq. (1).
Refer to Shmueli (2010) for a detailed treatment of the differences between explanatory and predictive modeling.
Recall that because all specifications use a log-log form, the linear prediction needs to be retransformed from logs to levels.
Refer to Online Resource 1 for a detailed description of the specifications used. The 95 % confidence intervals of the predictions (in brackets below the point estimates in Table 1) are calculated via bootstrap with 250 replications. Each replication involves a draw of the sample with replacement and of size equal to the sample size in the corresponding specification. The lower and upper levels of the interval are given by the 2.5 and 97.5 percentiles, respectively, of the distribution of estimates obtained from the 250 replications.
Both the high point estimate and the wide confidence interval in Eqs. (3) and (4) relative to other specifications result from including two regressors—namely, the maternal mortality rate and the number of physicians—for which Cuba is a significant outlier. As discussed in Online Resource 1, this leads to unnecessary inflation of the standard error of the prediction (Verbeek 2008) and hence the limits of the confidence interval.
Because the proceeding analysis uses the adjusted ratio for Cuba, we omit the Cuba subscript used before.
In Eq. (6), if PERISTAT countries classify late-term abortions as LFDs, then r would be higher, and thus Cuba’s corrected ENDs would be lower than if LTAs were not part of LFDs in comparison countries. If that is the case, then Cuba’s corrected ENDs should be interpreted as a lower bound on the actual ENDs.
An interesting exercise that might be used to assess the validity of Assumption 2 would be to compare perinatal mortality rates across urban and rural regions in Cuba. The idea is that the quality of perinatal mortality records may differ substantially between rural and urban areas as is the case in many developing countries. Therefore, lower levels of perinatal mortality in rural areas relative to urban areas should raise flags on the quality of the perinatal statistics. Unfortunately, Cuba does not provide fetal and neonatal mortality data by region or urban/rural status in order to perform these comparisons. However, most births in Cuba occur within health facilities, even in rural areas. For example, for 2004, Cuba reported that 99.9 % of births took place in health facilities (Dirección Nacional de Registros Médicos y de Salud 2010).
r min., r median, and r max. are 1.04, 1.80, and 3.03, respectively.
See Verbeek (2008), for example, for a detailed treatment of this issue.
These estimates are the ones obtained using the imputation approach presented in panel a of Table 2.
This value corresponds to using the highest LFD-END ratio observed in the PERISTAT sample.
The highest ENMR corresponds to Latvia with 3.78 deaths per 1,000 live births.
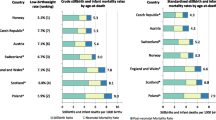
The data used to classify countries by income (high, middle) and geographical region (Europe, Latin America, North America) are from statistics reported by the World Bank (2015).
The solid vertical line uses the determinants approach (column 3, panel b in Table 2). The same analysis using the estimates from the imputation approach yields similar conclusions.
The boxplot for North America includes only two countries (Canada and the United States). Therefore, the lower and upper ends of the box are the reported IMR for these two countries, and the middle line is simply the average of the IMR for the two.
References
Aleshina, N., & Redmond, G. (2005). How high is infant and child mortality in central and eastern Europe and the CIS? Population Studies, 59, 39–54.
Allen, L. H. (2000). Anemia and iron deficiency: Effects on pregnancy outcomes. American Journal of Clinical Nutrition, 71, 1280–1284.
Anderson, F., Morton, S., Naik, S., & Gebrian, B. (2007). Maternal mortality and the consequences on infant and child survival in rural Haiti. Maternal and Child Health Journal, 11, 395–401.
Anthopolos, R., & Becker, C. M. (2010). Global infant mortality: Correcting for undercounting. World Development, 38, 467–481.
Belanger, D., & Flynn, A. (2009). The persistence of induced abortion in Cuba: Exploring the notion of an “abortion culture.” Studies in Family Planning, 40, 13–26.
Birchenall, J. A. (2007). Economic development and the escape from high mortality. World Development, 35, 543–568.
Brass, W. (1964, December). Uses of census and survey data for the estimation of vital rates. Paper presented at the African Seminar on Vital Statistics, Addis Ababa, Ethiopia.
Chay, K. Y., & Greenstone, M. (2000). The convergence in black-white infant mortality rates during the 1960’s. American Economic Review, 90, 326–332.
Cooper, R. S., Kenelly, J. F., & Orduez-Garca, P. (2006). Health in Cuba. International Journal of Epidemiology, 35, 817–824.
DePalma, A. (2007). “Sicko,” Castro and the “120 Years Club.” New York Times. Retrieved from http://www.nytimes.com/2007/05/27/weekinreview/27depalma.html
Dirección Nacional de Registros Médicos y de Salud. (2010). Anuario Estadístico de Salud 2010. La Habana, Cuba: Dirección Nacional de Registros Médicos y de Salud.
Duan, N. (1983). Smearing estimate: A nonparametric retransformation method. Journal of the American Statistical Association, 78, 605–610.
European Commission. (2003). Demographic statistics: Definitions and methods of collection in 31 European countries (Population and Social Conditions Working Paper No. 25). Luxembourg: Office for Official Publications of the European Communities.
EURO-PERISTAT. (2008). European perinatal health report. Retrieved from http://www.europeristat.com/
Foster, A., Gutierrez, E., & Kumar, N. (2009). Voluntary compliance, pollution levels, and infant mortality in Mexico. American Economic Review, 99, 191–197.
Gonzalez, R. (2015). Infant mortality in Cuba: Myth and reality. Cuban Studies, 43, 19–39.
Gruber, J., Hendren, N., & Townsend, R. M. (2014). The great equalizer: Health care access and infant mortality in Thailand. American Economic Journal: Applied Economics, 6, 91–107.
Gupta, S., Verhoeven, M., & Tiongson, E. R. (2003). Public spending on health care and the poor. Health Economics, 12, 685–696.
Hemminki, E., & Rimpela, U. (1991). Iron supplementation, maternal packed cell volume, and fetal growth. Archives of Disease in Childhood, 66, 422–425.
Hirschfeld, K. (2007a). Health, politics, and revolution in Cuba since 1898. Piscataway, NJ: Transaction Publishers.
Hirschfeld, K. (2007b). Reexamining the Cuban health care system: Toward a qualitative critique. Cuban Affairs, 2(3). Retrieved from http://www.cubanaffairsjournal.org
Kingkade, W., & Sawyer, C. (2001, August). Infant mortality in Eastern Europe and the former Soviet Union before and after the breakup. Paper presented at the 2001 IUSSP Meetings, Salvador de Bahia, Brazil.
Lofgren, K., & Lozano, R. (2015, May). Perinatal mortality in Mexico: Levels and trends by state and municipality, 1990 to 2013. Paper presented at the annual meeting of the Population Association of America, San Diego, CA.
McFarlane, A., Gissler, M., Bolumar, F., & Rassmusen, S. (2003). The availability of perinatal health indicators in Europe. European Journal of Obstetrics and Gynecology and Reproductive Biology, 111, 15–32.
McGuire, J. W. (2006). Basic health care provision and under-5 mortality: A cross-national study of developing countries. World Development, 34, 405–425.
Olausson, P. O., Cnattingius, S., & Haglund, B. (1999). Teenage pregnancies and risk of late fetal death and infant mortality. BJOG: An International Journal of Obstetrics and Gynaecology, 106, 116–121.
Ozcan, S. (2002). Does the mortality decline promote economic growth? Journal of Economic Growth, 7, 411–439.
Preston, S. H. (2007). The changing relation between mortality and level of economic development. International Journal of Epidemiology, 36, 484–490.
Pritchett, L., & Summers, L. (1996). Wealthier is healthier. Journal of Human Resources, 31, 841–868.
Rondo, P., Abbott, R., Rodrigues, L., & Tomkins, A. (1997). The influence of maternal nutritional factors on intrauterine growth retardation in Brazil. Paediatric and Perinatal Epidemiology, 11, 152–166.
Shmueli, G. (2010). To explain or to predict? Statistical Science, 25, 289–310.
Singh, P., Tyagi, M., Kumar, A., Dash, D., & Shankar, R. (1997). Fetal growth in maternal anemia. Journal of Tropical Pediatrics, 43, 89–92.
Stusser, R. J. (2012). Demystifying the Cuban health system: Insider’s view. Cuba in Transition, 21, 222–234.
Tamura, T., Goldenberg, R., Johnston, K., Cliver, S., & Hickey, C. (1996). Serum ferritin: A predictor of early spontaneous preterm delivery. Obstetrics and Gynecology, 87, 360–365.
Trussell, T. J. (1975). A re-estimation of the multiplying factors for the brass technique for determining childhood survivorship rates. Population Studies, 29, 97–108.
United Nations. (2013). Millennium development goals and beyond, 2015. Retrieved from http://www.un.org/millenniumgoals/
Velkoff, V. A., & Miller, J. E. (1995). Trends and differentials in infant mortality in the Soviet Union, 1970–90: How much is due to misreporting? Population Studies, 49, 241–258.
Verbeek, M. (2008). A guide to modern econometrics (3rd ed.). Chichester, UK: John Wiley and Sons.
World Bank. (2015). World Bank Databank. Retrieved from http://databank.worldbank.org
World Health Organization (WHO). (1993). International statistical classification of diseases and related health problems (10th revision) (ICD-10). Geneva, Switzerland: WHO.
World Health Organization (WHO). (2006). Neonatal and perinatal mortality: Country, regional and global estimates. Geneva, Switzerland: WHO.
World Health Organization (WHO). (2007). Neonatal and perinatal mortality: Country, regional and global estimates 2004. Geneva, Switzerland: WHO.
Acknowledgments
We thank Roberto Martin Gonzalez, M.D., Charles Becker, and participants at the annual meeting of the Association for the Study of Cuban Economy (ASCE) for useful comments and suggestions.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
ESM 1
(PDF 280 kb)
Rights and permissions
About this article

Cite this article
Gonzalez, R.M., Gilleskie, D. Infant Mortality Rate as a Measure of a Country’s Health: A Robust Method to Improve Reliability and Comparability. Demography 54, 701–720 (2017). https://doi.org/10.1007/s13524-017-0553-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13524-017-0553-7