
Abstract
We present a new mortality projection methodology that distinguishes smoking- and non-smoking-related mortality and takes into account mortality trends of the opposite sex and in other countries. We evaluate to what extent future projections of life expectancy at birth (e 0) for the Netherlands up to 2040 are affected by the application of these components. All-cause mortality and non-smoking-related mortality for the years 1970–2006 are projected by the Lee-Carter and Li-Lee methodologies. Smoking-related mortality is projected according to assumptions on future smoking-attributable mortality. Projecting all-cause mortality in the Netherlands, using the Lee-Carter model, leads to high gains in e 0 (4.1 for males; 4.4 for females) and divergence between the sexes. Coherent projections, which include the mortality experience of the other 21 sex- and country-specific populations, result in much higher gains for males (6.4) and females (5.7), and convergence. The separate projection of smoking and non-smoking-related mortality produces a steady increase in e 0 for males (4.8) and a nonlinear trend for females, with lower gains in e 0 in the short run, resulting in temporary sex convergence. The latter effect is also found in coherent projections. Our methodology provides more robust projections, especially thanks to the distinction between smoking- and non-smoking-related mortality.


Similar content being viewed by others
References
Alders, M., Keilman, N., & Cruijsen, H. (2007). Assumptions for long-term stochastic population forecasts in 18 European countries. European Journal of Population, 23, 33–69.
Alho, J. (2008). Aggregation across countries in stochastic population forecasts. International Journal of Forecasting, 24, 343–353.
Alho, J., Alders, M., Cruijsen, H., Keilman, N., Nikander, T., & Pham, D. Q. (2006). New forecast: Population decline postponed in Europe. Statistical Journal of the United Nations ECE, 23, 1–10.
Bongaarts, J. (2005). Long-range trends in adult mortality: Models and projection methods. Demography, 42, 23–49.
Bongaarts, J. (2006). How long will we live? (Policy Research Division Working Papers 215). New York: Population Council.
Bonneux, L., Looman, C. W. N., & Coebergh, J. W. (2003). Sterfte door roken in Nederland: Meer dan een miljoen doden tussen 1950 en 2015 [Mortality due to smoking in the Netherlands: 1.2 million tobacco-related deaths between 1950 and 2015]. Nederlands Tijdschrift voor Geneeskunde, 147, 917–921.
Booth, H. (2006). Demographic forecasting: 1980 to 2005 in review. International Journal of Forecasting, 22, 547–581.
Booth, H., Hyndman, R., Tickle, L., & de Jong, P. (2006). Lee-Carter mortality forecasting: A multi-country comparison of variants and extensions. Demographic Research, 15(9), 289–310. doi:10.4054/DemRes.2006.15.9
Booth, H., Maindonald, J., & Smith, L. (2002). Applying Lee-Carter under conditions of variable mortality decline. Population Studies, 56, 325–336.
Cairns, A. J. G., Blake, D., Dowd, K., Coughlan, G. D., Epstein, D., & Khalaf-Allah, M. (2011). Mortality density forecasts: An analysis of six stochastic mortality models. Insurance: Mathematics and Economics, 48, 355–367.
Coelho, E., & Nunes, L. C. (2011). Forecasting mortality in the event of a structural change. Journal of the Royal Statistical Society—Series A, 174, 713–736.
Doll, R., Peto, R., Wheatley, K., Gray, R., & Sutherland, I. (1994). Mortality in relation to smoking: 40 years’ observations on male British doctors. British Medical Journal, 309, 901–911.
Ediev, D. M. (2008). Extrapolative projections of mortality: Towards a more consistent method. Part I: The central scenario (Vienna Institute of Demography Working Papers 3/2008). Vienna, Austria: Vienna Institute of Demography.
Eurostat. (2010). EUROPOP2008 convergence scenario, national level—assumptions—life expectancy at birth. Retrieved from http://epp.eurostat.ec.europa.eu/portal/page/portal/population/data/database
Ezzati, M., & Lopez, A. D. (2003). Measuring the accumulated hazards of smoking: Global and regional estimates for 2000. Tobacco Control, 12, 79–85.
Giannakouris, K. (2004). EUROPOP 2004: Methodology for drafting mortality assumptions (Working paper for the Ageing Working Group of the Economic Policy Committee). Luxembourg: European Commission.
Gjonca, A., Tomassini, C., Toson, B., & Smallwood, S. (2005). Sex differences in mortality, a comparison of the United Kingdom and other developed countries. Health Statistics Quarterly, 26, 6–16.
Gjonca, A., Tomassini, C., & Vaupel, J. W. (1999). Male-female differences in mortality in the developed world (MPIDR Working Paper WP-1999-009). Rostock, Germany: Max Planck Institute for Demographic Research.
Goméz de Leon, J., & Texmon, I. (1992). Methods of mortality projections and forecasts. In N. Keilman & H. Cruijsen (Eds.), National population forecasting in industrialized countries (pp. 61–74). Amsterdam, The Netherlands: Swets and Zeitlinger.
Gunning-Schepers, L. J. (1988). The health benefits of prevention. A simulation approach. Rotterdam, The Netherlands: Erasmus University Rotterdam.
Janssen, F., & Kunst, A. E. (2005). Cohort patterns in mortality trends among the elderly in seven European countries, 1950–99. International Journal of Epidemiology, 34, 1149–1159.
Janssen, F., & Kunst, A. E. (2007). The choice among past trends as a basis for the prediction of future trends in old-age mortality. Population Studies, 61, 315–326.
Janssen, F., Kunst, A. E., & Mackenbach, J. P. (2007). Variations in the pace of old-age mortality decline among seven European countries, over the period 1950 to 1999: The role of smoking and factors earlier in life. European Journal of Population, 23, 171–188.
Janssen, F., Mackenbach, J. P., & Kunst, A. E. (2004). Trends in old-age mortality in seven European countries, 1950–1999. Journal of Clinical Epidemiology, 57, 203–216.
Janssen, F., Nusselder, W. J., Looman, C. W. N., Mackenbach, J. P., & Kunst, A. E. (2003). Stagnation in mortality decline among elders in The Netherlands. The Gerontologist, 43, 722–734.
Lee, R. D., & Carter, L. (1992). Modeling and forecasting U.S. mortality. Journal of the American Statistical Association, 87, 659–671.
Lee, R., & Miller, T. (2001). Evaluating the performance of Lee-Carter mortality forecasts. Demography, 38, 537–549.
Lee, R. D., & Nault, F. (1993). Modeling and forecasting provincial mortality in Canada. Paper presented at the World Congress of the IUSSP, Montreal, Canada.
Li, N., & Lee, R. (2005). Coherent mortality forecasts for a group of populations: An extension of the Lee-Carter method. Demography, 42, 575–594.
Lopez, A. D., Collishaw, N. E., & Piha, T. (1994). A descriptive model of the cigarette epidemic in developed countries. Tobacco Control, 3, 242–247.
Lundström, H. (2003). Mortality assumptions for Sweden. The 2000–2050 population projection. In T. Bengtsson & N. Keilman (Eds.), Perspectives on mortality forecasting I. Current practice (pp. 59–74). Stockholm: Swedish National Social Insurance Board.
Meslé, F. (2004). Espérance de vie: Un avantage féminin menacé? [Life expectancy: A female advantage under threat]. Population & Sociétés, 402.
Murphy, M. J. (1990). Methods of forecasting mortality for population projections. In British Society for Population Studies (Ed.), Population projections: Trends, methods and uses (pp. 87–101). London, UK: Office of Population Censuses and Surveys.
Olshansky, S. J. (1988). On forecasting mortality. The Milbank Quarterly, 66, 482–530.
Pampel, F. C. (2001). Cigarette diffusion and sex differences in smoking. Journal of Health and Social Behaviour, 42, 388–404.
Pampel, F. C. (2002). Cigarette use and the narrowing sex differential in smoking. Population and Development Review, 28, 77–104.
Pampel, F. C. (2003). Declining sex differences in mortality from lung cancer in high-income nations. Demography, 40, 45–65.
Pampel, F. C. (2005). Forecasting sex differences in mortality in high income nations: The contribution of smoking. Demographic Research, 13(18), 455–484. doi:10.4054/DemRes.2005.13.18
Peto, R., Lopez, A. D., Boreham, J., Thun, M., & Heath, C., Jr. (1992). Mortality from tobacco in developed countries: Indirect estimation from national vital statistics. Lancet, 339, 1268–1278.
Pollard, J. (1987). Projection of age-specific mortality rates. Population Bulletin United Nations, 21(22), 55–69.
Preston, S., & Wang, H. (2006). Sex mortality differences in the United States: The role of cohort smoking patterns. Demography, 43, 631–646.
Preston, S. H., Glei, D. A., & Wilmoth, J. R. (2010). A new method for estimating smoking-attributable mortality in high-income countries. International Journal of Epidemiology, 39, 430–438.
Renshaw, A. E., & Haberman, S. (2006). A cohort-based extension to the Lee-Carter model for mortality reduction factors. Insurance: Mathematics and Economics, 58, 556–570.
Rostron, B. L. (2010). A modified new method for estimating smoking-attributable mortality in high-income countries. Demographic Research, 23(14), 399–420. doi:10.4054/DemRes.2010.23.14
Rostron, B. L., & Wilmoth, J. R. (2011). Estimating the effect of smoking on slowdowns in mortality declines in developed countries. Demography, 48, 461–479.
Shang, H. L., Booth, H., & Hyndman, R. (2011). Point and interval forecasts of mortality rates and life expectancy: A comparison of ten principal component methods. Demographic Research, 25(5), 173–214. doi:10.4054/DemRes.2011.25.5
Sprague, W. W. (2009). LCFIT: Web-based software for estimating the Lee-Carter method for modeling and forecasting mortality, with extensions to coherent forecasts of Li and Lee, and Lee-Carter method with sparse and incomplete data. Retrieved from http://lcfit.demog.berkeley.edu
Statistics Canada. (2010). Population projections for Canada: Provinces and territories 2005–2031. Section I: Methods and assumptions. Retrieved from http://www.statcan.gc.ca/pub/91-520-x/00105/4095124-eng.htm
Trovato, F., & Lalu, N. M. (1996). Narrowing sex differentials in life expectancy in the industrialized world: Early 1970’s to early 1990’s. Social Biology, 43, 20–37.
United Nations Department of Economic and Social Affairs Population Division. (2004). World population to 2300. New York: United Nations.
United Nations Population Division. (2007). World population prospects: The 2006 revision. New York: United Nations.
van Bodegom, D., Bonneux, L., Engelaer, F. M., Lindenberg, J., Meij, J. J., & Westendorp, R. G. J. (2010). Dutch life expectancy from an international perspective. Leiden, The Netherlands: Leyden Academy on Vitality and Ageing.
van der Meulen, A., van Duin, C., & Garssen, J. (2009). Bevolkingsprognose 2008–2050: Model en veronderstellingen betreffende de sterfte [Population forecast 2008–2050: The method and assumptions regarding mortality]. Bevolkingstrends, 2009(1), 41–53.
van Duin, C., van der Meulen, A., & Garssen, J. (2006). Bevolkingsprognose 2006–2050: Model en veronderstellingen betreffende de sterfte [Population forecast 2006–2050: The method and assumptions regarding mortality]. Bevolkingstrends, 2006(4), 62–77.
van Oers, J. A. M. (2002). Health on course? The 2002 Dutch public health status and forecasts report [in Dutch]. Bilthoven, The Netherlands: RIVM Bohn Stafleu Van Loghum.
van Poppel, F., & de Beer, J. (1996). Evaluation of standard mortality projections for the elderly. In G. Caselli & A. D. Lopez (Eds.), Health and mortality among elderly populations (pp. 288–312). Oxford, UK: Clarendon Press.
Waldron, I. (1993). Recent trends in sex mortality ratios for adults in developed countries. Social Science & Medicine, 36, 451–462.
Wang, H., & Preston, S. H. (2009). Forecasting United States mortality using cohort smoking histories. Proceedings of the National Academy of Sciences, 106, 393–398.
Wilmoth, J. R. (2000). Demography of longevity: Past, present, and future trends. Experimental Gerontology, 35, 1111–1129.
Wilson, T., & Bell, M. (2007). Probabilistic regional population forecasts: The example of Queensland, Australia. Geographic Analysis, 39, 1–25.
Acknowledgments
We would like to thank Anouschka van der Meulen and Trudy Lisci from Statistics Netherlands for the provision of detailed data on all-cause mortality and population size.
Author information
Authors and Affiliations
Corresponding author
Appendix: Projection of Smoking-Related Mortality
Appendix: Projection of Smoking-Related Mortality
Future levels of the age- and sex-specific etiological fraction (EF) (i.e., the proportion of all deaths attributable to smoking) for the Netherlands (Fig. 3) were estimated by applying the general ideas from the descriptive model of the smoking epidemic (Lopez et al. 1994), by examining historical trends in etiological fractions by age and sex, and by studying recent trends in smoking prevalence.
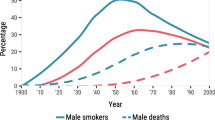
The descriptive model of the smoking epidemic shows the common pattern of an increase and thereafter a decrease in smoking prevalence, followed by similar patterns in smoking-attributable mortality three to four decades later. For females, the increase in both smoking prevalence and smoking-attributable mortality started later than for males and is more modest. All countries follow more or less the same patterns, but with a different timing of onset, saturation, and so on (Lopez et al. 1994).
Females in Denmark and in England and Wales are among the few who already experienced a peak in smoking-attributable mortality. In these two countries, the smoking-attributable mortality trends by age for males show a clear cohort pattern up to the peak, followed by a period pattern after the peak. For females, the cohort pattern is much less evident. An important observation is that for each age group the time span between the maximum EF for males and the maximum EF for females is almost the same and approximately equals the number of years between males and females in reaching the maximum EF for all ages combined.
In the Netherlands, the maximum level of EF for all ages combined was reached for males in 1983, whereas the maximum has not yet been reached by females in any of the age groups. For females, we therefore need to estimate the year and level of the maximum EF, as well as the trend up to and after this maximum. For males, it is necessary to estimate only the future decline.
To estimate the year in which EF will reach its maximum among Dutch females, we applied an age-period-cohort Poisson regression model to lung cancer mortality data from 1950 to 2004 by five-year age groups and five-year periods. As an offset term, we used the log of the average population. By adding the average age of dying from lung cancer (68) to the cohort with the highest lung cancer mortality (1953), we obtained the year in which EF reaches its maximum for females: 2021. This year resembles adding a lag time of 35–41 years to the years 1980–1986, in which smoking prevalence reached its maximum level among Dutch females. The years in which EF will reach its maximum for females for the separate age groups were subsequently estimated by applying the difference in timing between males and females of the maximum EF for all ages combined (38) to the years in which the maximum EF was reached for males in the separate age groups. These years in which the EF reached its maximum for males were assessed by means of the smoothed trends, obtained by fitting fourth-degree polynomials.
For females, the trend in the age-specific EF up to the maximum was based on the age-specific growth rate observed over the past 10 years. A deceleration of the growth rate to 1 was applied.
The age-specific long-term decline after the maximum for both males and females was set equal to the trend in EF for all ages combined after the maximum for males (–1.5 %), which reflects the current trend in smoking prevalence for all ages combined (–1.7 % for males, and –1.3 % for females), as well as the similarity in the current decline in smoking prevalence in the Netherlands between both sexes and the different age groups.

Smoking-attributable mortality fractions (EF) by age and sex, observed (smoothed) and projected, 1950–2040. The restriction that the proportion of the population exposed to smoking should be smaller or equal to 1 is responsible for the plateau for males aged 45–49 in 1954–1985
Rights and permissions
About this article
Cite this article
Janssen, F., van Wissen, L.J.G. & Kunst, A.E. Including the Smoking Epidemic in Internationally Coherent Mortality Projections. Demography 50, 1341–1362 (2013). https://doi.org/10.1007/s13524-012-0185-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13524-012-0185-x