
Abstract
Objective
To compare the frequency of asymmetric septal hypertrophy in appropriate for gestational age infants born to diabetic mothers with those born to non-diabetic mothers.
Methods
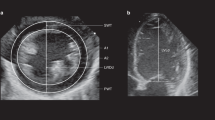
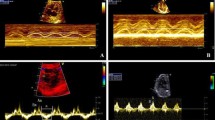
We compared 38 full term infants born to diabetic mothers with 85 full term infants of non-diabetic mothers. 2-D echocardiography was obtained in the first 24 hours after birth.
Results
Asymmetric septal hypertrophy was only present in infants born to diabetic mothers (50% vs. 0%; P<0.001). Intraventricular septum thickness and intraventricular septum/ posterior wall of the left ventricle ratio was also significantly higher in the first group (P<0.001). We found no correlation between mother´s glycated hemoglobin levels and intraventricular septum thickness in newborns.
Conclusions
Asymmetric septal hypertrophy is a common finding in infants born to diabetic mothers, even if they are appropriate for gestational age.
Similar content being viewed by others

References
Persson B, Hanson U. Neonatal morbidities in gestational diabetes mellitus. Diabetes Care. 1998;21:B79–84.
Breitweser JA, Meyer RA, Sperling MA, Tsang RC, Kaplan S. Cardiac septal hypertrophy in hyperinsulinemic infant. J Pediatr. 1980;96:535–9.
Cooper MJ, Enderlein MA, Tarnoff H, Rogé CL. Asymmetric septal hypertrophy in infants of diabetic mothers. Am J Dis Child. 1992;146:226–9.
Vela-Huerta MM, Vargas-Origel A, Olvera-López A. Asymmetrical septal hypertrophy in newborn infants of diabetic mothers. Am J Perinatol. 2000;2:89–94.
Weber H, Copel J, Reece MA, Green J, Kleinman CS. Cardiac growth in fetus of diabetic mothers with good metabolic control. J Pediatr. 1991;18:103–7.
Vincent M, Benbrik N, Romefort B, Colombel A, Bézieau S, Isidor B. Three patients presenting with severe macrosomia and congenital hypertrophic cardiomyopathy: a case series. J Med Case Rep. 2017;11:78.
Lubchenco LO. The estimation of gestational age in the high-risk infant. Philadelphia WB Saunders, 1976:9.
Taylor RM, Price-Douglas W. The STABLE program: postresuscitation/ pretransport stabilization care of sick infants. J Perinat Neonatal Nurs. 2008;22:159–65.
American Diabetes Association. Classification and diagnosis of diabetes}. Diabetes Care}. 2017};40}:S11–
Kitzmiller JL, Block JM, Brown FM, Catalano PM, Conway DL, Coustan DR, et al. Managing preexisting diabetes for pregnancy: summary of evidence and consensus recommendations for care. Diabetes Care. 2008;31:1060–79.
Zielinsky P, Piccoli AL Jr. Myocardial hypertrophy and dysfunction in maternal diabetes. Early Hum Dev. 2012;88:273–8.
Mert MK, Satar M, Özbarlas N, Yaman A, Özgünen FT, Asker HS, et al. Troponin T and NT ProBNP levels in gestational, type 1 and type 2 diabetic mothers and macrosomic infants. Pediatr Cardiol. 2016;37:76–83.
Gordon EE, Reinking BE, Hu S, Yao J, Kua KL, Younes AK, et al. Maternal hyperglycemia directly and rapidly induces cardiac septal overgrowth in fetal rats. J Diabetes Res. 2015; 479565:1–11.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Vela-Huerta, M.M., Amador-Licona, N., Orozco Villagomez, H.V. et al. Asymmetric Septal Hypertrophy in Appropriate for Gestational Age Infants Born to Diabetic Mothers. Indian Pediatr 56, 314–316 (2019). https://doi.org/10.1007/s13312-019-1522-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13312-019-1522-6