
Abstract
Objective
To assess the association of demographic and clinical aspects with radiographically diagnosed pneumonia.
Design
By active surveillance, the admitted pneumonia cases by the pediatrician on duty were identified in a 2-year period. Demographic, clinical and radiographic data were registered into standardized forms.
Setting
A public university pediatric hospital in Salvador, Northeast Brazil.
Patients
Children <5 years-old.
Main outcome measures
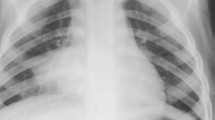
Radiographically diagnosed pneumonia based on detection of pulmonary infiltrate/consolidation.
Results
301 cases had the chest X-ray evaluated by a pediatric radiologist blinded to clinical information, among whom pulmonary infiltrate and consolidation were described in 161 (54%) and 119 (40%), respectively. Chest X-ray was read normal for 140 cases. Overall, the median age was 17 months (mean 20±14, range 12 days-59 months). Pulmonary infiltrate was less frequently described among patients aged under 1 year (41.3% vs 59.9%, P=0.002, OR [95%CI] = 0.47 [0.29–0.76]) and hyperinflation was significantly more frequent in this age group (27.9% vs 4.1%, P<0.001, OR [95%CI] = 9.14 [4.0–20.9]). By multiple logistic regression, fever on admission was independently associated with pulmonary infiltrate (OR [95%CI] = 1.68 [1.03–2.73]) or consolidation (1.79 [1.10–2.92]), wheezing was independently associated with absence of pulmonary infiltrate (0.53 [0.33–0.86]) or of consolidation (0.53 [0.33–0.87]). The positive likelihood ratio of fever on examination for pulmonary infiltrate and consolidation was 1.49 (95%CI: 1.11–1.98) and 1.49 (95%CI: 1.14–1.94), respectively.
Conclusion
Presence of fever enhanced 2.5 times the chance of children hospitalized with lower respiratory tract disease to have radiographically diagnosed pneumonia.
Similar content being viewed by others


References
Stein RT, Marostica PJ. Community-acquired pneumonia: a review and recent advances. Pediatr Pulmonol. 2007;42:1095–1103.
Lynch T, Platt R, Gouin S, Larson C, Patenaude Y. Can we predict which children with clinically suspected pneumonia will have the presence of focal infiltrates on chest radiograph? Pediatrics. 2004;113:e186–e189.
Donnelly LF. Maximizing the usefulness of imaging in children with community-acquired pneumonia. Am J Roentgen. 1999;172:505–512.
Swingler GH, Zwarenstein M. Chest radiograph in acute respiratory infections in children. The Cochrane Library, 3, 2007.
Cherian T, Mulholland EK, Carlin JB, Ostensen H, Amin R, Campo M, et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull World Health Organ. 2005;83:353–359.
El-Radhi AS, Barry W. Thermometry in paediatric practice. Arch Dis Child. 2006;91:351–356.
World Health Organization. Global database on child growth and malnutrition: the Z-score or standard deviation system (WHO/NUT/97.4). Geneva: WHO; 1997 [online]. Available from: URL: www.who.int/ nutgrowthdb. Accessed April 10, 2008.
Shann F, Hart K, Thomas D. Acute lower respiratory infections in children: possible criteria for selection of patients for antibiotic therapy and hospital admission. Bull World Health Organ. 1984;62:749–753.
Campbell H, Byass P, Greenwood BM. Simple clinical signs for diagnosis of acute lower respiratory infections. Lancet. 1988;2:742–743.
Cherian T, John TJ, Simoes E, Steinhoff MC, John M. Evaluation of simple clinical signs for the diagnosis of acute lower respiratory infection. Lancet. 1988;2:125–128.
Spooner V, Barker J, Tulloch S, Lehmann D, Marshall TF, Kajoi M, et al. Clinical signs and risk factors associated with pneumonia in children admitted to Goroka Hospital, Papua New Guinea. J Trop Pediatr. 1989;35:295–300.
Sachdev HPS, Vasanthi B, Satyanarayana L, Puri RK. Simple predictors to differentiate acute asthma from ARI in children: Implications for refining case management in the ARI Control Program. Indian Pediatr. 1995;31:1251–1259.
Castro AV, Nascimento-Carvalho CM, Ney-Oliveria F, Araújo-Neto CA, Andrade SC, Loureiro LL, et al. Additional markers to refine the World Health Organization algorithm for diagnosis of pneumonia. Indian Pediatr. 2005;42:773–781.
Smyth RL, Openshaw PJ. Bronchiolitis. Lancet. 2006;368:312–322.
Hazir T, Nisar YB, Qazi SA, Khan SF, Raza M, Zameer S, et al. Chest radiography in children aged 2–59 months diagnosed with non-severe pneumonia as defined by World Health Organization: descriptive multicentre study in Pakistan. BMJ. 2006;333:629.
World Health Organization. Integrated Management of Childhood Illness chart booklet. (WC 503.2). Geneva: WHO, 2008. Available from: URL://whqlibdoc.who.int/publications/2008/9789241597289_eng.pdf. Accessed December 10, 2008.
Factor SH, Schillinger JA, Kalter HD, Saha S, Begum H, Hossain A, et al. Diagnosis and management of febrile children using the WHO/UNICEF guidelines for IMCI in Dhaka, Bangladesh. Bull World Health Organ. 2001;79:1096–1105.
Mathews B, Shah S, Cleveland RH, Lee EY, Bachur RG, Neuman MI. Clinical predictors of pneumonia among children with wheezing. Pediatrics. 2009;124:e29–e36.
Graham SM, English M, Hazir T, Enarson P, Duke T. Challenges to improving case management of childhood pneumonia at health facilities in resource-limited settings. Bull World Health Organ. 2008;86:349–355.
Castro AV, Nascimento-Carvalho CM, Ney-Oliveira F, Araújo-Neto CA, Andrade SC, Loureiro L, et al. Pulmonary infiltrate among children with cough and tachypnea. Pediatr Infect Dis J. 2006;25:757.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Key, N.K., Araújo-Neto, C.A., Cardoso, M.R.A. et al. Characteristics of radiographically diagnosed pneumonia in under-5 children in Salvador, Brazil. Indian Pediatr 48, 873–877 (2011). https://doi.org/10.1007/s13312-011-0142-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13312-011-0142-6