
Abstract
Although acute appendicitis remains the most common cause of acute abdomen in General Surgery practice, negative appendectomy rates are still high in particularly female patients. Appendicitis scoring systems considering gender can help the clinician to reduce negative appendectomy rates in females. This present study aims to compare the Lintula, Ripasa, Fenyo-Lindberg scoring systems, which use gender as a variable, with the Alvarado, Karaman, scoring systems to evaluate which CSS is more successful in the differential diagnosis of appendicitis in females. We analyzed the records of the patients operated on with a prediagnosis of acute appendicitis in our clinic between 2020 and 2021, retrospectively. Alvarado, adult appendicitis score (AAS), appendicitis inflammatory response score (AIRS), Ripasa, Karaman, Lintula, and Fenyo Lindberg scores were calculated for each patient. The patients were divided into two groups as male and female, according to gender. Receiver operator characteristic (ROC) curve analysis was used to identify the best cut-off value and assess the performance of the test score for appendicitis. Three hundred and sixty-three patients were included in the study. One hundred seventy-two (47.4%) of the patients were male, and 191 (52.6%) were female. Alvarado and AAS were the most valuable score in female (AUC: 0.805, sensitivity: 0.63, specificity: 0.83; and area under curve (AUC): 0.794, Sensitivity 0.71, Specificity: 0.76, respectively), male group (AUC: 0.828, Sensitivity: 0.71, Specificity: 0.83; and AUC: 0.834, Sensitivity 0.74, Specificity: 0.77, respectively), and when patients were not categorized by gender (AUC: 0.818, Sensitivity: 0.67 Specificity: 0.83; and AUC: 0.794, Sensitivity 0.71, Specificity: 0.76, respectively). Although the Alvarado scoring system is the first defined appendicitis scoring system, it seems as superior to the many scoring systems defined after it in predicting appendicitis, even in female patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introductıon
Acute appendicitis remains the most common cause of acute abdomen in General Surgery practice [1]. However, difficulties are experienced in the differential diagnosis of appendicitis, especially in conditions where the surgeon is inexperienced or there are technical deficiencies [2]. Negative appendectomies cause various morbidities such as wound infection in 10–12% of patients and intra-abdominal adhesions that may cause infertility in the future. Furthermore, unnecessary appendectomies cause a prolonged hospital stay and an increase in health expenditures [2,3,4]. Routine computed tomographic examination (CT), which can be used to reduce the negative appendectomy rate, will cause unnecessary radiation exposure, especially in patients of childbearing age [5]. Ultrasound (USG) is the imaging method that should be the first choice in diagnosing appendicitis due to its lower cost, easier accessibility, and no radiation exposure compared to CT, with a sensitivity of 79% and a specificity of 87% [6]. Nevertheless, USG performed by an inexperienced radiologist with a heavy patient load, especially outside of working hours, may mislead the clinician and cause overtreatment or under treatment [7, 8].
Numerous clinical scoring systems (CSSs) have been developed since Alvarado's description of the first CSS for appendicitis. CSSs can be useful for reducing negative appendectomy rates, which can cause several morbidities, particularly in women [9]. In this study, we aim to compare the adult appendicitis score (AAS), Lintula, Ripasa, and Fenyo-Lindberg CSSs, which use the gender as a variable, with the Alvarado, appendicitis inflammatory response score (AIRS), and Karaman CSSs to evaluate which of them is more successful in the differential diagnosis of appendicitis in women.
Materials and methods
Approval for the study was obtained from Local Ethics Committee (Approval No: E-71522473–050.01.04-25251-251). The records of patients who were operated on with the initial diagnosis of acute appendicitis in our clinic between 2020 and 2021 were reviewed retrospectively. Patients under the age of 18, who were pregnant, and who had undergone previous abdominal surgery were excluded from the present study. Mann–Whitney U Test for nonparametric numeric variables, chi-squared test for categorical variables were used to compare variables between male and female patient groups.
Patients’ gender, nationality, age, complaints, physical examination findings, the results of white blood cell (WBC) count, C-Reactive Protein (CRP) level, neutrophil count (Neu), mean platelet volume (MPV), left shift in neutrophils values, urinalysis and abdominoplevic CT were recorded. Alvarado, adult appendicitis score (AAS), appendicitis inflammatory response score (AIRS), Karaman, Ripasa, Lintula and Fenyo Lindberg scores were calculated for each patient. Histopathological examination results of appendectomy specimens were used for final diagnosis, and we used them to evaluate the predictive power of CSSs.
Descriptive analyses were performed to provide data regarding the general characteristics of the study population. Kolmogorov–Smirnov test was used to evaluate whether the distributions of numerical variables were normal. Accordingly, the Mann–Whitney U Test was used to compare the nonparametric numeric variables between groups. The numeric variables were presented as mean ± standard deviation or median [Q1–Q3]. Categorical variables were compared by the chi-squared test. Categorical variables were presented as a count and percentage. A p value < 0.05 was considered significant. Receiver operator characteristic (ROC) curve analysis was used to identify the best cut-off value and assess the performance of the test score for appendicitis. Analyses were performed using SPSS statistical software (IBM SPSS Statistics, Version 23.0. Armonk, NY: IBM Corp.)
Results
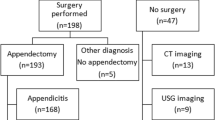
The records of 402 patients with an initial diagnosis of appendicitis during the last year were evaluated for study inclusion. Twelve patients under the age of eighteen, 18 patients with the history of previous abdominal surgery, and 9 pregnant patients were excluded from the study. Totally, 172 (47.4%) of the 363 patients included in the study were male, and 191 (52.6%) were female. (Table 1).
Although the mean age of the females was tended to be lower than that of the male patients, the difference was not statistically significant (32:17–86 vs. 33:17–83; p = 0.91).
When the complaints of the patients at the time of admission to the hospital were examined, no significant difference was observed between the male and female patient groups in terms of vomiting, loss of appetite, duration of symptoms, and increasing pain (p = 0.10, p = 0.77, p = 0.48, p = 0.50; respectively). Pain outside the right lower quadrant was found to be significantly less in the male patient group (25.6%) than in the female patient group (39.3%) (p = 0.02). Pain transition from the umbilicus to the lower right quadrant was found to be significantly higher in the male (58.7%) group than in the female (47.1%) group (p = 0.02).
There was no difference between male and female patient groups in terms of fever, bowel sounds with auscultation, tenderness in the right lower quadrant, Rebound, Rigidity, Rovsing sign (p = 0.31, p = 0.30, p = 0.89, p = 0.08, p = 0.95, 0.20; respectively). (Table 1).
There was no significant difference between male and female patient groups in terms of CRP, Neutrophil count (Neu), Mean platelet volume (MPV), Left shift in neutrophils values (p = 0.56, p = 0.52, p = 0.82, p = 0.79; respectively). WBC values were found to be significantly higher in the male patient group (11.9 ± 14.8) than in the female patient group (9.72 ± 15.5) (p = 0.02). Negative urine examination was found to be significantly higher in the male patient group (149/86.6%) than in the female patient group (140/73.3%) (p < 0.05). The reporting rate of CT as appendicitis was significantly higher for male patients (69.8%) than for female patients (59.5%) (p = 0.04). (Table 1).
As a result of the histopathological examination of the pathology specimens, appendicitis was detected in 220 (60.6%) patients but not in 143 (39.4%) patients. When the histopathological examination results were categorized by gender, the rate of acute appendicitis in female patients (52.9%) was found to be statistically significantly lower than in male patients (69.2%) (p < 0.05). (Table 1) We summarized the distribution of the results of clinic scoring systems between the genders in Table 2.
When the patients were not categorized by gender, receiver operating characteristic curve (ROC Curve) analyses revealed that Alvarado score (AUC: 0.818, sensitivity: 0.67 specificity: 0.83) was found to be more successful than Karaman score (AUC: 0.754, sensitivity 0.67, specificity: 0.72), Raja Isteri Pengiran Anak Saleha Appendicitis (Ripasa) Score (AUC: 0.654, sensitivity 0.54, specificity:0.62) Lintula score (AUC: 0.667, sensitivity 0.64, specificity: 0.63), Fenyo Lindberg score (AUC: 0.711, sensitivity 0.65, specificity: 0.65), and AIRS (AUC: 0.743, sensitivity 0.67, specificity: 0.68) whereas its accuracy was similar with AAS (AUC: 0.801, sensitivity 0.74, specificity: 0.68) (Table 3, Fig. 1). In female patients, Alvarado score (AUC: 0.805, sensitivity: 0.63, specificity: 0.83) and AAS (AUC: 0.794, sensitivity 0.71, specificity: 0.76) were detected as more successful than Karaman score (AUC: 0.728, sensitivity: 0.63, specificity: 0.72), Ripasa score (AUC: 0.680, sensitivity: 0.62, specificity: 0.60), Lintula score (AUC: 0.648, sensitivity: 0.63, specificity: 0.62), Fenyo Lindberg score (AUC: 0.689 sensitivity: 0.61, specificity: 0.58), and AIRS (AUC: 0.740, sensitivity 0.67, specificity: 0.64) (Table 3, Fig. 2). In male patients, Alvarado score (AUC: 0.828, sensitivity: 0.71, specificity: 0.83) and AAS (AUC: 0.834, sensitivity 0.74, specificity: 0.77) were detected more successful than Karaman score (AUC: 0.729, sensitivity: 0.71, specificity: 0.73), Ripasa score (AUC: 0.601, sensitivity: 0.57, specificity: 0.56), Lintula score (AUC: 0.658, sensitivity: 0.65, specificity: 0.66), Fenyo Lindberg score (AUC: 0.698 sensitivity: 0.64, specificity: 0.60) and AIRS (AUC: 0.766, sensitivity 0.66, specificity: 0.74) (Table 3, Fig. 3).

ROC Curve analysis not regarding gender

ROC Curve Analysis of Female Patients

ROC Curve Analysis of Male Patients
Dıscussıon
Particularly in young, fertile, female patients, acute pelvic pain that requires admission to the hospital is frequently encountered. In this situation, the differential diagnosis must be made among various diseases such as acute pelvic pain, diseases such as acute appendicitis, pelvic inflammatory disease, ovarian torsion, cystitis, rupture of follicle cyst, intestinal obstruction [10, 11]. The rate of negative appendectomy in females is much higher than in males, varying between 3 and 25% in various publications [2, 12,13,14]. We found that the rate of negative appendectomy was significantly higher in our female patient group than in our male patient group. This difference could be resulted from the conditions of our healthcare system during the pandemic. The opportunities for in-hospital observations with conservative approach in patients with abdominal pain were limited, and the repetition of pre-surgical researches including comprehensive gynecologic, gastroenterologic, and psychological evaluations for the differential diagnosis could not be done in most of the patients. In addition to the fact that surgeons are in favor of operating patients with right lower quadrant pain, rather than following up to avoid possible appendicitis perforation, it may be thought that microscopic appendix inflammation may be overlooked even if macroscopically normal appendicitis is encountered in a patient operated for abdominal pain [15].
Appendicitis scoring systems considering gender can help the clinician to reduce negative appendectomy rates in women [16]. Adult appendicitis score (AAS), Fenyö-Lindberg, Lintula, and RIPASA scores consider gender as a variable for the prediction of acute appendicitis, although its weight varies in each scoring system. It has been shown in various publications that Fenyo-Lindberg is more successful than other scoring systems in predicting acute appendicitis in women [16]. The scoring system defined by Lintula and colleagues, in their study with patients aged 4–15 years who underwent surgery for acute appendicitis, is also being used in adults [17]. Although the Ripasa score was developed in 2010 based on the idea that there may be differences between geographical regions in terms of the success of scoring systems, it also uses gender as a variable [18]. Our study revealed that, even though each of the three scoring systems was successful in predicting appendicitis, they were not superior to the Alvarado and Karaman scores. In both Karaman and Alvarado scoring systems, gender is not considered when calculating the score. In their published study in 2018, they claimed that the Karaman scoring system is superior to the Alvarado score in predicting appendicitis and reducing the rate of negative appendectomy [7]. In our study, we found that the Karaman scoring system was more successful in predicting appendicitis either in male or female patient groups than scoring systems that considering gender. When all patients were evaluated without gender categorization, the Karaman score was again found to be more successful than the scoring systems considering gender as a parameter. However, the Alvarado scoring system was found to be more successful in predicting appendicitis than all scoring systems, including the Karaman score, in both male and female patient groups.
In similar with our results, a recent systematic literature review performed by Podda and colleagues for the studies regarding the usage of common CSSs and imaging for the diagnosis of appendicitis revealed that Alvarado, AIR and AAS scores were sufficiently sensitive to exclude appendicitis, accurately identifying low-risk patients and decreasing the need for imaging and the negative appendectomy rates in these patients [19]. On the other hand, for young patients deemed to be at high-risk of appendicitis according to the scores, because of the high prevalence of the disease in this group of patients (~ 90%), a negative imaging scan cannot rule out appendicitis. According to this review, the sensitivity and specificity were 0.91–0.94 and 0.90–0.95 for CT scan, and 0.78–0.88 and 0.81–0.94 for USG, respectively. Therefore, Podda and colleagues concluded that a high-probability score for appendicitis may be used to select patients in which imaging was not needed in young patients. When the surgeon deems diagnostic imaging is still needed to confirm appendicitis despite the patient has been scored at high-risk, a conditional CT scan strategy is advised, with CT scan performed only after a negative or equivocal USG results.
The main limitation of the present study is that our population was composed of the patients admitted to our hospital that is also the main centre serving also for patients with the novel coronavirus 2019 (COVID-19) during the pandemic in our city. The opportunities for in-hospital observations with conservative approach in patients with abdominal pain were limited, and the repetition of pre-surgical researches including comprehensive gynecologic, gastroenterologic, and psychological evaluations for the differential diagnosis could not be done in most of the patients. Therefore, the negative appendectomy rate was higher than expected in our study population (more higher in females).
Conclusıon
Although the Alvarado scoring system is the first defined appendicitis scoring system, it continues to be superior to the scoring systems defined after it in predicting appendicitis, even in female patients. The authors report on the use of cross-sectional imaging (i.e. CT scan) which identified appendicitis more frequently in males than in females. Further studies are warranted to clarify the utility of CSSs in decreasing the needs of CT imaging for the diagnosis of acute appendicitis.
References
Pieper R, Kager L (1982) The incidence of acute appendicitis and appendectomy. An epidemiological study of 971 cases. Acta Chir Scand 148:45–49
Gelpke K, Hamminga J, Bastelaar J, de Vos B, Bodegom M, Heineman E et al (2020) Reducing the negative appendectomy rate with the laparoscopic appendicitis score; a multicenter prospective cohort and validation study. Int J Surg 79:257–264
Lee M, Paavana T, Mazari F, Wilson TR (2014) The morbidity of negative appendicectomy. Ann R Coll Surg Engl 96:517–520
Practice Committee of the American Society for Reproductive Medicine in collaboration with the Society of Reproductive Surgeons (2019) Postoperative adhesions in gynecologic surgery: a committee opinion. Fertil Steril 112:458–463
Stroman DL, Bayouth C, Kuhn J, Westmoreland M, Jones R, Fisher TL et al (1999) The role of computed tomography in the diagnosis of acute appendicitis. The American Journal of Surgery 178:485–488
Gligorievski A (2018) US diagnosis of acute appendicitis. MOJ Anat Physiol 5:225–229
Karaman K, Ercan M, Demir H, Yalkın Ö, Uzunoğlu Y, Gündoğdu K et al (2018) The Karaman score: a new diagnostic score for acute appendicitis. Ulus Travma Acil Cerrahi Derg 24:545–551
Davenport MS, Ellis JH, Khalatbari SH, Myles JD, Klein KA (2020) Effect of work hours, caseload, shift type, and experience on resident call performance. Acad Radiol 17:921–927
Eskelinen M, Ikonen J, Lipponen P (1994) Sex-specific diagnostic scores for acute appendicitis. Scand J Gastroenterol 29:59–66
Gross M, Blumstein SL, Chow LC (2005) Isolated fallopian tube torsion: a rare twist on a common theme. Am J Roentgenol - AJR 185:1590–1592
Taylor S, Lee H, Singh R (2021) Innocent until proven guilty: acute on chronic tubal torsion mimicking pelvic inflammatory disease. J Surg Case Rep 5:187
Jess P, Bjerregaard B, Brynitz S, Holst-Christensen J, Kalaja E, Lund-Kristensen J (1981) Acute appendicitis. Prospective trial concerning diagnostic accuracy and complications. Am J Surg 141:232–234
Jeon BG (2017) Predictive factors and outcomes of negative appendectomy. Am J Surg 213:731–738
Chandrasegaram M, Rothwell LA, An EI, Miller RJ (2012) Pathologies of the appendix: a 10-year review of 4670 appendicectomy specimens. ANZ J Surg 82:844–847
Bhangu A, RIFT Study Group on behalf of the West Midlands Research Collaborative (2020) Evaluation of appendicitis risk prediction models in adults with suspected appendicitis. Br J Surg 107:73–86
Enochsson L, Gudbjartsson T, Hellberg A, Rudberg C, Wenner J, Ringqvist I et al (2004) The Fenyö-Lindberg scoring system for appendicitis increases positive predictive value in fertile women—a prospective study in 455 patients randomized to either laparoscopic or open appendectomy. Surg Endosc Other Interv Tech 18:1509–1513
Lintula H, Pesonen E, Kokki H, Vanamo K, Eskelinen MA (2005) diagnostic score for children with suspected appendicitis. Langenbeck’s Archives of Surgery 390:164–170
Chong CF, Adi MIW, Thien A, Suyoi A, Mackie AJ, Tin AS et al (2010) Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J 51:220–225
Podda M, Pisanu A, Sartelli M, Coccolini F, Damaskos D, Augustin G et al (2021) Diagnosis of acute appendicitis based on clinical scores: is it a myth or reality? Acta Biomed 92(4):e2021231
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Ethical approval
This is a retrospective study which has been conducted in accordance with the ethical standards as laid in the 1964 Helsinki Declaration.
Research involving human participants and animals.
A study-specific approval was obtained by the local ethical committee of Sakarya University Faculty of Medicine.
Informed Consent
Informed consent was obtained from all individual participants included in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Capoglu, R., Gonullu, E., Bayhan, Z. et al. Comparison of scoring systems regarding the gender as a parameter with the traditional scoring systems for predicting appendicitis. Updates Surg 74, 1035–1042 (2022). https://doi.org/10.1007/s13304-022-01272-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-022-01272-y