
Abstract
Objective(s)
To study the epidemiology and outcome of pregnancy complicated by obstetric cholestasis (OC).
Methods(s)
Retrospective case control study of 45 women with OC at a tertiary private hospital from November 2003 to November 2006. Statistical analysis was performed using the z test when appropriate. A p value <0.05 was considered statistically significant.
Results
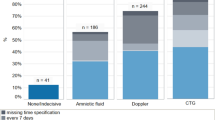
The incidence of OC was 8.2%. The most common symptom was generalized pruritus which appeared after 28 weeks in 73.3% cases. The cesarean section rate was 93.3%. A higher incidence of meconium staining in amniotic fluid at delivery (17.1% vs 1.1%, p<0.005) and preterm premature rupture of membranes (8.9% vs 1.1%, p<0.01) was noted without an increase in preterm delivery rate (24.4% vs 15.6%, not significant). There was no statistically significant difference in the following parameter — pathological cardiotocography, 1–5 minute Apgar score <7, intrauterine growth restriction, neonatal intensive care admission or perinatal mortality. There was no case of postpartum hemorrhage.
Conclusion
The incidence of OC is high in the Indian population. Perinatal outcome is good in actively managed women, although at the cost of a high intervention rate.
Similar content being viewed by others

References
Kenyon AP, Girling JC, Obstetric cholestasis. In, Studd J. (Editor), Progress in Obstetrics and Gynaecology Edinburgh: Churchill Livingstone, 2005;37–56.
Royal College of Obstetricians and Gynecologists. Obstetric cholestasis. RCOG Guideline No.43, 2006.
Reyes H. The spectrum of liver and gastrointestinal disease seen in cholestasis of pregnancy. Gastroenterol Clin North Am 1992;21:905–921.
Kenyon AP, Piercy CN, Girling J et al. Obstetric cholestasis, outcome with active management: a series of 70 cases. BJOG 2002;109:282–288.
Rioseco AJ, Ivankovic MB, Manzur A et al. Intrahepatic cholestasis of pregnancy: a retrospective case-control study of perinatal outcome. Am J Obstet Gynecol 1994;170:890–895.
Fisk NM, Storey GN. Fetal outcome in obstetric cholestasis. Br J Obstet Gynaecol 1988;95:1137–1143.
Ray A, Tata RJ, Balsara R et al. Cholestasis of pregnancy. J Obstet Gynecol India 2005;55:247–250.
Heinonen S, Kirkinen P. Pregnancy outcome with intrahepatic cholestasis. Obstet Gynecol 1999;94:189–193.
Zapata R, Sandoval L, Palma J et al. Ursodeoxycholic acid in the treatment of intrahepatic cholestasis of pregnancy. A12 year experience. Liver Int 2005;25:548–554.
Rodrigues CM, Marin JJ, Brites D. Bile acid patterns in meconium are influenced by cholestasis of pregnancy and not altered by ursodeoxycholic acid treatment. Gut 1999;45:446–452.
Alsulyman OM, Ouzounian JG, Ames-Castro M et al. Intrahepatic cholestasis of pregnancy: perinatal outcome associated with expectant management. Am J Obstet Gynecol 1996;175:957–960.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Padmaja, M., Bhaskar, P., Kumar, G.J. et al. A study of obstetric cholestasis. J Obstet Gynecol India 60, 225–231 (2010). https://doi.org/10.1007/s13224-010-0030-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-010-0030-3