
Abstract
Introduction
Naloxone is commonly administered in emergency department (ED) to reverse opioid intoxication. Several naloxone dose recommendations exist for acute management of opioid intoxication based on limited published clinical data. A case series of ED patients with opioid-induced ventilatory depression that was reversed using a low-dose naloxone (0.04 mg with titration) is presented.
Methods
ED patients with opioid-induced ventilatory depression requiring naloxone administration were identified through medical toxicology consultation. Retrospective review of medical records was performed. Collected data included history, and pre- and post-naloxone data, including respiratory rate (RR), pulse oximetry (pulse ox), end-tidal CO2 level (ET-CO2), and Richmond Agitation Sedation Scale (RASS).
Results
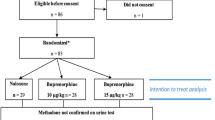
Fifteen ED patients with moderate to severe opioid-induced ventilatory depression (median RR, 6 breaths/min) who were managed using low-dose naloxone strategy were identified. Twelve of 15 patients reported ingestion of methadone (range, 30 to 180 mg). The median naloxone dose of 0.08 mg (range, 0.04 to 0.12 mg) reversed opioid-induced ventilatory and CNS depression. Two patients experienced acute opioid withdrawal after receiving 0.08 mg.
Conclusion
ED patients with moderate to severe opioid-induced ventilatory depression can be reversed using 0.04 mg IV naloxone with appropriate dose titration.

Similar content being viewed by others


Abbreviations
- ET-CO2 :
-
End-tidal CO2 level
- ED:
-
Emergency department
- CNS:
-
Central nervous system
- RASS:
-
Richmond Agitation Sedation Scale
- RR:
-
Respiratory rate
- IV:
-
Intravenous
References
Foldes FF. The Human Pharmacology and Clinical Use of Narcotic Antagonists. Med Clin North Am. 1964;48:421–43.
Buajordet I, Naess AC, Jacobsen D, Brors O. Adverse events after naloxone treatment of episodes of suspected acute opioid overdose. Eur J Emerg Med. 2004;11(1):19–23.
Manfredi PL, Ribeiro S, Chandler SW, Payne R. Inappropriate use of naloxone in cancer patients with pain. J Pain Symptom Manage. 1996;11(2):131–4.
Doyon S. Opioids. In: Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, editors. Tintinalli’s emergency medicine: a comprehensive study guide. 7th ed. New York: McGraw-Hill; 2011. p. 1230–3.
Bardsley CH. Opioids. In: Marx JA, Hockberger RS, Walls RM, editors. Rosen’s emergency medicine: concepts and clinical practice. 8th ed. Philadelphia, PA: Elsevier/Saunders; 2013. p. 2052–6.
Nelson LS, Howland MA. Antidotes in depth: opioid antagonists. In: Hoffman RS, Howland MA, Lewin NA, Nelson LS, Goldfrank LR, editors. Goldfrank’s toxicologic emergencies. 10th ed. New York: McGraw-Hill Medical; 2014. p. 510–5.
Kim HK, Nelson LS. Reducing the harm of opioid overdose with the safe use of naloxone: a pharmacolgic review. Expert Opin Drug Saf. 2015;14(7):1137–46.
Boyer EW. Management of opioid analgesic overdose. N Engl J Med. 2012;367(2):146–55.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN guildelines): Adult Cancer Pain. 2014. http://www.nccn.org/professionals/physician_gls/pdf/pain.pdf. Accessed 15 Nov 2014
Connors NC, Nelson LS. Wide variation in naloxone dosing recommendations for acute opioid toxicity. J Med Toxicol. 2014;10:76–7.
Conflict of Interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kim, H.K., Nelson, L.S. Reversal of Opioid-Induced Ventilatory Depression Using Low-Dose Naloxone (0.04 mg): a Case Series. J. Med. Toxicol. 12, 107–110 (2016). https://doi.org/10.1007/s13181-015-0499-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13181-015-0499-3