
Abstract
Ketamine has been the commonest abusive substance used by Hong Kong teenager since 2005. It is also the fourth commonest poison encountered in Hong Kong Poison Information Centre (HKPIC) poisoning data in 2010. From June 2008 to July 2011, HKPIC managed 188 and 96 cases of acute and chronic ketamine poisoning, respectively, which reflect its acute and chronic toxicity pattern. Demographically, there is a male predominance, and the majority is between the ages of 10–39. For the acute cases, 48 % presented with neurological features such as confusion, drowsiness, or transient loss of consciousness which usually subside with supportive care in a few hours. For the chronic cases, 92 % of them presented with features of ketamine cystitis while about 66 % presented with chronic abdominal pain. The current understanding of ketamine cystitis and chronic abdominal pain will be reviewed. Management is primarily symptomatic measures and most importantly abstinence from ketamine use.
Similar content being viewed by others


Introduction
Ketamine is a “dissociative anesthetic” that was first synthesized in 1964; it is used as an intravenous anesthetic therapeutically and has also increasingly been used as an abusive agent. In Hong Kong, ketamine has been the commonest abusive substance in teenagers since 2005 [1] according to the data of the Central Registry of Drug Abuse in which abusive cases are voluntarily reported by law enforcement departments, welfare agencies, health care facilities, and tertiary institutions. The Hong Kong Poison Information Centre (HKPIC) was established in 2005 and provides 24-h phone consultation service to health care professionals in Hong Kong for poison information and clinical management advice. It now receives about 4,500 poisoning cases per year. From the data of HKPIC, ketamine-related poisoning contributed to 7.1 % of the poisoning case and is the fourth commonest poison encountered in the year 2010 [2]. Recreational ketamine abusers may seek medical advice for acute, sub-acute, or chronic presentations for physical, psychiatric, or social problems.
Method
From June 2008 to July 2011, the ketamine poisoning cases in the HKPIC database were retrieved to study the patterns of acute and chronic toxicity. Acute cases were defined as those who presented with an acute ketamine-related problem to the Accident and Emergency Department (AED) while chronic cases were those who presented with sub-acute or chronic problems in the outpatient clinic.
Data collected included patient demographic data (age, sex), exposure data (route, duration of ketamine abuse), clinical data (clinical features, investigations results), and management data (use of decontamination, antidotes, and other specific treatments). The presentation is further classified into each of the following entities clinically: neurological, urinary, cardiovascular, gastrointestinal, nasal, and psychiatric.
Results
Totally, there were 284 cases, including 188 acute and 96 chronic cases, respectively. All cases abused ketamine by insufflation. The age and gender distribution of our cases was shown in Figs. 1 and 2.

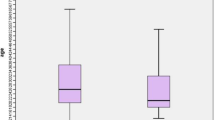
Sex and age distribution of acute cases

Sex and age distribution of chronic cases
For the 188 acute cases (Fig. 3), 90 cases (48 %) presented with neurological features such as confusion, drowsiness, or transient loss of consciousness which usually subsided with supportive care in 2 to 6 h. Sixty cases (32 %) had lower urinary tract symptoms compatible with ketamine cystitis while 50 (27 %) abusers presented with cardiovascular features such as hypertension (systolic blood pressure >160 mmHg or diastolic pressure >90 mmHg) and tachycardia (heart rate >100 per minute). Forty nine (26 %) of them presented with abdominal pain, and 19 (10 %) patients presented with acute psychiatric problems such as acute psychosis, respectively.

Presenting symptoms of acute cases
For the 96 chronic cases (Fig. 4), their mean and median duration of ketamine abuse is 8.6 years (SD, 4.1 years) and 4 years, respectively. Majority (88, 92 %) of them presented with features of ketamine cystitis such as dysuria, urgency, and frequency while 63 (66 %), 40 (42 %), and 15 (16 %) of them presented with chronic abdominal pain, nasal problems (including three cases of septal perforation), and psychiatric features, respectively.

Presenting symptoms of chronic cases
Discussion
For the 188 acute cases, the commonest presentation was neurological features. The typical acute ketamine intoxication syndrome in our case series is confusion, dizziness, impaired conscious level, or a reported transient period of loss of consciousness, with the classical “nasal halo” (Fig. 5). From our clinical experience, nystagmus is also commonly seen on those cases who can comply with physical examination. About 27 % of our cases had cardiovascular features; nearly all of them were in the form of mild hypertension and tachycardia. The clinical effect usually lasts for a few hours, and most cases can be managed with conservative and supportive measures. The findings are comparable to our study concerning the ketamine abusers' presentation in AED from 2005 to 2008 [3].

Nasal halo
For the 96 chronic cases, 92 % of them have features of ketamine cystitis. The typical clinical syndrome of ketamine cystitis includes lower urinary tract symptoms such as dysuria, urgency, and frequency. There are also features of small, painful bladder and upper urinary tract obstruction. Apart from Hong Kong, ketamine cystitis is known and reported in countries including Canada, Japan, Taiwan, the UK, and others [4, 5].
The causative agent for ketamine cystitis is believed to be ketamine itself or its metabolites. Although the possibility of unrecognized adulterants to be the cause for the syndrome is raised, it is very unlikely based on the fact that the syndrome is similar in different geographic areas over time in which the adulterant is expected to vary. For the mechanism of damage, it is still unconfirmed at this moment, and possible mechanisms including direct toxic damage, microvascular injury, or immune-related damage to the urinary tract by ketamine or/and its metabolites were suggested [6]. Concerning the duration of ketamine abuse and the development of ketamine cystitis, our data found the median years of exposure was 4 for our cohort in which 92 % of them have features of ketamine cystitis. Another study in Hong Kong found that a ketamine abuser with at least 2 years of exposure (more than three uses per week) had significantly lower voided volume and higher scores in the Pelvic Pain, Urgency and Frequency questionnaire, which is comparable with our clinical experience [7].
Until now, no proven effective treatment for ketamine cystitis is established except ketamine abstinence. A recent study of 66 ketamine abusers found that the voided volume was significantly higher for those who quitted ketamine for more than 1 year than those who still abused ketamine or stopped it for less than 3 months [7].
In our chronic cases, two thirds had features of ketamine-associated abdominal pain. The pain is usually moderate to severe, dull or cramping pain in the epigastrium, with associated nausea and vomiting, and some cases have deranged liver function tests also. Case reports suggested the pain being biliary in origin [8–10], in the form of cholestasis and biliary dilatation with uniform pattern, with fusiform dilatation of the entire common hepatic and bile duct [8]. However, the mechanism of this pathology remains unknown. In a retrospective study of 37 ketamine abusers for the upper gastrointestinal problems [11], 75.7 % of them had upper GI symptoms, which are comparable to our chronic cohort. Fifteen (40.5 %) and 9 (24.3 %) of them had elevated alanine aminotransferase (ALT) and alkaline phosphate (ALP), respectively, but the study was unable to demonstrate any association between epigastric pain and deranged ALT or ALP. Only 14 of the abusers underwent an esophagogastroduodenoscopy examination in which 12 of them had gastritis while one abuser had gastroduodenitis and the other had a normal finding.
The management of ketamine-associated abdominal pain is primarily symptomatic and again, most importantly, abstinence from ketamine use. It was shown that the odd ratio of symptomatic relief of the abdominal pain is 12.5 (95 % CI 1.2–130) for those who stopped ketamine versus those who continued its use [11].
There are several limitations of this study. First of all, our consultation and reporting system was on a completely voluntary basis. Secondly, data were obtained from the consulting medical professions and may be incomplete in some case. However, given the number of case we received (4,500 per year) and the accessibility to the clinical records of nearly all of our consultation/reporting cases, we believed the data represented the updated acute and chronic presentations of ketamine abusers in Hong Kong.
Conclusion
We present a large case series of 284 ketamine abuser with regard to their acute and chronic toxic manifestations. In acute intoxication, neurological features in terms of confusion and impaired consciousness are the commonest presentations. For chronic presentations, majority had features of ketamine cystitis and chronic abdominal pain. Management is primarily symptomatic measures and most importantly abstinence from ketamine use.
Change history
08 June 2021
A Correction to this paper has been published: https://doi.org/10.1007/s13181-021-00841-8
References
Narcotics Division, Security Bureau, the Government of Hong Kong Special Administrative Region of the People's Republic of China (2009) Central registry of drug abuse, http://www.nd.gov.hk/en/drugstatistics.htm. Accessed on 13 Feb 2012
Chan YC, Tse ML, Lau FL (2012) Hong Kong Poison Information Centre: annual report 2010. Hong Kong J Emerg Med 19:110
Ng SH, Tse ML, Ng HW, Lau FL (2010) Emergency department presentation of ketamine abusers in Hong Kong: a review of 233 cases. Hong Kong Med J 16(1):6–11
Wood D, Cottrell A, Baker SC, Southgate J, Harris M, Fulford S, Woodhouse C, Gillatt D (2011) Recreational ketamine: from pleasure to pain. BJU Int 107(12):1881–1884
Nomiya A, Nishimatsu H, Homma Y (2011) Interstitial cystitis symptoms associated with ketamine abuse: the first Japanese case. Int J Urol 18(10):735
Chu PS, Kwok SC, Lam KM, Chu TY, Chan SW, Man CW, Ma WK, Chui KL, Yiu MK, Chan YC, Tse ML, Lau FL (2007) ‘Street ketamine’-associated bladder dysfunction: a report of ten cases. Hong Kong Med J 13(4):311–313
Mak SK, Chan MT, Bower WF, Yip SK, Hou SS, Wu BB, Man CY (2011) Lower urinary tract changes in young adults using ketamine. J Urol 186(2):610–614
Wong SW, Lee KF, Wong J, Ng WW, Cheung YS, Lai PB (2009) Dilated common bile ducts mimicking choledochal cysts in ketamine abusers. Hong Kong Med J 15(1):53–56
Lo RS, Krishnamoorthy R, Freeman JG, Austin AS (2011) Cholestasis and biliary dilatation associated with chronic ketamine abuse: a case series. Singap Med J 52(3):e52–e55
Seto WK, Ng M, Chan P, Ng IO, Cheung SC, Hung IF, Yuen MF, Lai CL (2011) Ketamine-induced cholangiopathy: a case report. Am J Gastroenterol 106(5):1004–1005
Poon TL, Wong KF, Chan MY, Fung KW, Chu SK, Man CW, Yiu MK, Leung SK (2010) Upper gastrointestinal problems in inhalational ketamine abusers. J Dig Dis 11(2):106–110
Author information
Authors and Affiliations
Corresponding author
Additional information
The original online version of this article was revised: Please note that author given name and surname were inadvertently transposed in this article as original published: Chan Yiu-Cheung should have read Yiu-Cheung Chan.
About this article
Cite this article
Chan, YC. Acute and Chronic Toxicity Pattern in Ketamine Abusers in Hong Kong. J. Med. Toxicol. 8, 267–270 (2012). https://doi.org/10.1007/s13181-012-0229-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13181-012-0229-z