
Abstract
Breast cancer incidence is actually the highest one among all cancers. Overall breast cancer management is associated with challenges considering risk assessment and predictive diagnostics, targeted prevention of metastatic disease, appropriate treatment options, and cost-effectiveness of approaches applied. Accumulated research evidence indicates promising anti-cancer effects of phytochemicals protecting cells against malignant transformation, inhibiting carcinogenesis and metastatic spread, supporting immune system and increasing effectiveness of conventional anti-cancer therapies, among others. Molecular and sub-/cellular mechanisms are highly complex affecting several pathways considered potent targets for advanced diagnostics and cost-effective treatments. Demonstrated anti-cancer affects, therefore, are clinically relevant for improving individual outcomes and might be applicable to the primary (protection against initial cancer development), secondary (protection against potential metastatic disease development), and tertiary (towards cascading complications) care. However, a detailed data analysis is essential to adapt treatment algorithms to individuals’ and patients’ needs. Consequently, advanced concepts of patient stratification, predictive diagnostics, targeted prevention, and treatments tailored to the individualized patient profile are instrumental for the cost-effective application of natural anti-cancer substances to improve overall breast cancer management benefiting affected individuals and the society at large.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why 3PM concepts are pivotal to advance primary, secondary, and tertiary care in the overall breast cancer management?
According to the World Health Organization, female breast cancer has now surpassed lung cancer as the leading cause of global cancer incidence, as of 2021, accounting for estimated 2.3 million new annual cases (12%) worldwide [1]. Alarming statistics are particularly dramatic for the triple-negative breast cancer (TNBC): more than 50% of affected individuals in this patient cohort die within the first 6 months of the metastatic disease [2]. Patient stratification demonstrates that lymph node-positive TNBC patients being slim (BMI < 18.5) have particularly poor outcomes [3]. Young patients aged below 35 years diagnosed with metastatic breast cancer demonstrate significantly lower 5-year disease-free survival and significantly higher prevalence of distant metastasis compared to their counterparts aged above ≥ 65 years [4]. Rapidly increasing breast cancer incidence in general and, in particular, aggressive metastatic breast cancer sub-types in young female populations prompt application of advanced screening programmes, and targeted preventive and individualized approaches in overall breast cancer management [5]. To this end, primary (sub-optimal health conditions with evident risks of the disease predisposition), secondary (predisposition to the metastatic breast cancer), and tertiary (making palliative care to the management of chronic disease) care in the framework of predictive, preventive, and personalized medicine is considered an advanced strategy to improve individual outcomes and cost-efficacy of the disease management [6,7,8,9,10].
Phytochemicals are instrumental to advance cancer management
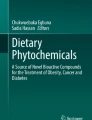
Phytochemicals as secondary plant metabolites represent non-nutrient chemical compounds of plants [11]. The sources of phytochemicals include vegetables, fruits, grains, beverages, and medicinal plants [12]. Examples of bioactive phytochemicals are represented by numerous polyphenols, carotenoids, organosulfur compounds, and alkaloids (Fig. 1) [13].

Classification and main sources of phytochemicals [12,13,14,15,16,17]. Polyphenols, carotenoids, organosulfur compounds, and alkaloids represent examples of large classes of phytochemicals. Polyphenols (plant phenolics) are further divided into flavonoids, phenolic acids, coumarins, stilbenes, hydrolyzable, condensed tannins, lignans, and lignins [13]. Indeed, current evidence state over 8000 identified polyphenols, but the number is largely underestimated [18]. Carotenoids are naturally occurring liposoluble pigments (red, orange, yellow) of fruits and vegetables and can be found also in fungi, algae, and bacteria. Nearly 700 carotenoids have been identified and can be further divided into carotenes, xantophylls, and apocarotenoids (derivatives) [14]. The presence of nitrogen atoms/s is a basic characteristic of alkaloids [19]. Alkaloids can be subdivided into numerous sub-classes. As stated by Heinrich et al. in October 2020, the Dictionary of Natural Products included 27,683 alkaloids [20]. Organosulfur compounds include isothiocyanates, indoles, allylic sulfur compounds, and sulforaphane [15]
Traditional Chinese medicine (TCM) herbs has been used to prevent and treat diseases for thousands of years [21]. It is currently investigated whether it could prevent or treat cancer or enhance conventional anticancer therapies [22]. Written records of plants used for medicinal purposes date back 5000 years to Sumerians, but archaeological studies provided evidence of using medicinal plants 60,000 years ago in an area now called Iraq. Despite the long history of use and many times effectivity, the use of herbal medicine declined with the progress of modern or conventional Western medicine due to the lack of scientific proofs and verifications [23]. Nevertheless, recent research and the modern approach of the individual persons to their health status highlight the potential of phytochemicals for human health. Phytochemicals, either isolated or their mixtures in whole plant foods, exert many biological activities, including antioxidant, immunomodulatory, anti-microbial, anti-inflammatory, and anticancer. In addition, phytochemicals might have only minimal side effects, are cost-effective, and are usually widely available. Nevertheless, the usability of phytochemicals faces several complications, such as a low bioavailability due to their rapid and extensive metabolism, which is commonly individual in patient and for each phytochemical different [12, 24,25,26,27]. But these negatives do not disclassify phytochemicals and their use as a traditional or modern treatment of various diseases [28]. Preclinical research highlights the vast potential of phytochemical to combat breast cancer functioning as preventive or therapeutic agents [24, 29,30,31].
Pleiotropic effects of phytochemicals demonstrated in vitro and in vivo
Recent evidence demonstrates pleiotropic effects of phytochemicals (isolated or their mixtures) on multiple signalling pathways and suppresses malignant transformation in vitro and in vivo [32].
Results of experiments showed a direct association between the application of phytochemicals and the suppression of cancer development through the modulation of different cell signalling pathways [33]. Numerous phytoconstituents in function food regulate events connected with malignant transformation, such as apoptosis [26], proliferation [34], angiogenesis [27], inflammation [35], invasiveness, and metastasis [12]. Many studies described the significant role of phytochemicals in modulating epigenetic changes and metabolic reprogramming—key events for cancer initiation, promotion, and progression [36, 37]. Preclinical trials using breast cancer models demonstrated oncostatic effects of secondary metabolites of plants via modulation of critical enzymes contributing to aerobic glycolysis [38], detoxification and antioxidant machinery [39], DNA repair mechanisms [40], or programmed cell death [25]. In addition, phytochemicals can in experimental models of breast cancer restore global and gene-specific promoter DNA methylation patterns [41], alter the gene expression by modulating miRNA expression [42], or affect histone modifications [43].
Multiple chemopreventive and oncostatic effects of phytochemicals observed in preclinical research represent a promising avenue in cancer management, which could be introduced in the clinical sphere. More in-depth investigations of the role of phytochemicals will accelerate the development of novel therapeutic strategies to improve life quality and the overall survival of patients with breast cancer.
Current state of clinical evidence on the effectiveness of phytochemicals in breast cancer management
Despite intensive evaluation in preclinical cancer research, limited evidence is available for the effectiveness of natural compounds in the clinical sphere [27]. Nevertheless, current clinical studies provide valuable evidence on effectiveness of phytochemicals in breast cancer management, especially of breast cancer preventive agents, phytochemicals as therapeutic agents, phytochemicals combined with conventional therapies (e.g. chemotherapy), or phytochemicals mitigating the side effects of current therapeutic approaches.
Phytochemicals in breast cancer prevention
The biological activities of fruits, vegetables, or medicinal plants are attributed to the presence of phytochemicals (isolated or their mixtures) [12, 25, 44, 45]. Despite the crucial anticancer activity of isolated phytochemicals, current research highlights the potent additive or synergic effects of mixtures of phytochemicals in whole plant food [24, 27, 29, 44, 46,47,48]. Healthy diet patterns characterized by a greater intake of whole plant-based food have been on a long-term basis associated with a reduced risk of cancer. Previous studies showed a reduced risk of breast cancer associated with a Mediterranean diet [49, 50], with a consumption of a specific type of fruits (peaches/nectarines) [51], or with polyphenols present in green tea [52].
Table 1 shows the current clinical evaluations conducted on breast cancer patients and analyses the association between breast cancer risk and dietary patterns.
A recent case–control study in a Middle Eastern country demonstrated an inverse association (P < 0.05) between dietary total antioxidant capacity and the risk of breast cancer [53]. Similarly, an inverse association between legumes and nuts as the whole food group and breast cancer was observed in Iranian women [54]. Also, a population-based case–control study in Iranian women demonstrated an inverse association between adherence to plant-based diet index and hypothesized healthy plant-based diet index connected with breast cancer risk [55]. The Healthy Eating Index (HEI) is a standard measure of diet quality that assesses the quality of diet based on the evaluation of the intake of total fruits, whole fruits, total vegetables, greens and beans, whole grains, dairy, total food proteins, seafood and plant proteins, fatty acids, refined grains, sodium, added sugars, and saturated fats. Indeed, the HEI score is associated with a decreased risk of breast cancer [56]. Moreover, pro-vegetarian dietary patterns are predominantly plant-based or plant-forward but not fully vegetarian or vegan. A large prospective study conducted on a Mediterranean cohort described that a moderate adherence to pro-vegetarian dietary patterns might decrease the risk of breast cancer [57]. Interestingly, Farvid et al. (2019) evaluated a plant-based diet and the risk of breast cancer through repeated measures over 30 years. The results showed the association of larger fruit and vegetable intake, especially cruciferous and yellow or orange vegetables, and a lower risk of breast cancer. The intake of total vegetables was linked to a lower risk of oestrogen receptor-negative (ER-) breast cancer, higher intake of total fruits and vegetables with a lower risk of HER2-enriched, basal-like, and luminal A breast cancer molecular subtypes [58]. Similarly, women consuming a healthier diet (β-carotene, vitamins A and C, and folate) were at decreased risk of breast cancer compared with women with a diet characterized by high fat and lamb meat [60]. In addition, greater intake of bean fiber, beans, and grains may lower the risk of ER- and progesterone receptor-negative (PR-) breast cancer [61]. Moreover, a higher intake of cruciferous vegetable, glucosinolates, and isothiocyanates is indicated to be inversely associated with breast cancer risk in Chinese women [62]. Mammographic density (MD) describes the relative amount of fibroglandular to fat tissue, which is often reported as percent MD (PMD)—a proportion of dense area over total breast area [63]. MD is considered an independent risk factor for breast cancer [59]. Women with ≥ 75% MD are associated with a 4 to 6 times greater risk of breast cancer than women with MD below 10% [63]. Nevertheless, a randomized intervention trial suggested that a 24-month dietary intervention (plant foods with a low glycaemic load, low in saturated fats and alcohol) or physical training (combining daily moderate-intensity activities and session of more strenuous activity once per week) could reduce mammographic breast density [59]. Similarly, green tea extract supplementation reduced PMD in younger women compared with the placebo group [63]. Multivariate case–control analyses revealed an inverse association between adherence to the Mediterranean Diet and risk of ER- postmenopausal breast cancer (approximately 40% reduction of risk), but the study did not show significant association with oestrogen receptor positive (ER +) or total breast cancer risk. These results provide proofs of special benefits of diet containing large amounts of phytochemicals in the breast cancer prevention due to the poor prognosis of ER- breast cancer subtype [64].
However, for more efficient chemopreventive analyses, surrogate endpoint biomarkers should be validated for the short-term assessment of breast cancer risk. Still, any chemopreventive agent should be precisely evaluated, for example by assessing potential long-term toxicity during repeated use [65].
Phytochemicals mitigating side effects of cancer therapy
The benefits of utilization of phytochemicals are also associated with reducing the side effects of conventional therapeutic strategies. Table 2 provides an overview of the current clinical research conducted on the effects of phytochemicals to mitigate the side effects of conventional therapeutic approaches against breast cancer; indeed, these studies are specified in Table 2.
For decades, surgery represented a mainstay in breast cancer therapy [77]. Breast cancer-related lymphedema (BCRL), described as a regional and generalized accumulation of lymph fluid in the interstitial space of the upper limb due to the interruption of the axillary lymphatic system, is a common complication associated with breast cancer surgery. Indeed, Linfadren® that contains flavonoid diosmin, coumarins, and phenolic glycoside arbutin was safe and effective when combined with complex decongestive therapy (CDT) for reducing BCRL compared to CDT alone [66].
Except for surgery, the primary treatment modalities for breast cancer include radiation, chemotherapy, hormone-based therapies, or targeted therapy [78, 79]. Indeed, conventional breast cancer therapies are associated with various adverse effects. Topical application of gel with silymarin, a flavonoid extracted from Silybum marianum (silymarin gel 1% containing extract with 80% of flavonolignans including silybin, silychristin, silydianin, 2,3‐dehydrosilybin, and 2,3‐dihydrosilychristin once daily), reduced radiodermatitis’s severity and delays its occurrence after 5 weeks of application in breast cancer patients undergoing radiotherapy [67]. Similarly, Nigela sativa L. extract (5% gel administered twice a day at least two hours before and after radiotherapy) decreased the severity of acute radiation dermatitis and delayed moist desquamation onset in breast cancer patients undergoing radiotherapy [68]. As stated above, epidemiologic studies conclude that green teas decrease the risk of breast cancer [52]. The flavonoid epigallocatechin-3-gallate (EGCG) represents the most abundant catechin in green tea and is most likely responsible for the potent biological activity of green tea [80]. A study by Zhu et al. (2016) stated the topical EGCG as an effective treatment of dermatitis induced by radiation. They demonstrated reduced pain, burning feeling, itching, pulling, and tenderness in breast cancer patients undergoing a mastectomy followed by radiotherapy; besides, no grade 3 or 4 dermatitis was observed in patients receiving EGCG even though receiving the same dose of radiation [69].
Worsened quality of life (QoL) and toxicity is common during breast cancer therapy. For example, an impaired nutritional status due to gastro-intestinal toxicity (nausea, vomiting) during chemotherapy during prolonged time may result in the interruption of the treatment. Worsening QoL might be related to worsened prognosis and an increase in the risk of recurrence [70]. However, the nutritional intervention on healthy eating (emphasizing fruits, vegetables, grains, among others) during the first three cycles of neoadjuvant chemotherapy could minimize clinical involutions during therapy and therapy interruptions. This nutritional intervention preserved QoL and handgrip strength showing decreased occurrence of nausea/vomiting and loss of appetite, and lower frequency of leukopenia and abdominal pain when compared with the control [70]. Anthracycline-based chemotherapy is a backbone of adjuvant breast cancer therapy. However, anthracycline-based chemotherapy is associated with myelosuppression, hair loss, and cardiotoxicity as the most serious side effect. An administration of phytochemicals or herbs could represent a potent shift to prevent anthracycline-induced cardiotoxicity. Platycodon grandiflorum that has been long used in traditional Chinese medicine to treat cardiovascular diseases prevented acute and chronic cardiac injury induced by anthracycline in early breast cancer patients without compromising the effects of the chemotherapy. However, the antitumor activity itself was not affected [71]. Peppermint (Mentha piperita) extract exerted a significant decrease in the man score of severity of nausea, vomiting, and anorexia in breast cancer patients undergoing chemotherapy compared with the control group [72]. The subcutaneous injection of mistletoe extracts showed a trend toward less neutropenia and improved pain and appetite loss scores in breast cancer patients undergoing surgery and adjuvant chemotherapy with cyclophosphamide, adriamycin, and 5-fluorouracil. However, the mistletoe extracts did not affect the frequency of relapse or metastasis within 5 years [73]. Also, ginger capsules relieved chemotherapy-induced nausea and vomiting in breast cancer patients undergoing chemotherapy [74].
Oestrogens are crucially involved in the pathogenesis of breast cancer. Aromatase catalyses essential steps in the biosynthesis of oestrogen; and thus, aromatase inhibitors represent effective targeted therapy in ER + breast cancer patients [81]. Musculoskeletal symptoms (bone pain, arthralgia, myalgia, carpal tunnel syndrome, trigger finger) develop in approximately half of the patients on aromatase inhibitors. Therefore, aromatase inhibitor-associated musculoskeletal symptoms (AIMSS) among patients on aromatase inhibitors result in lower QoL and poor adherence to aromatase inhibitors. Indeed, the discontinuation of therapy due to musculoskeletal symptoms occurs in up to 20% of them. Indeed, early discontinuation and non-adherence to aromatase inhibitors are related to an increase in mortality of breast cancer patients [76]. The conventional therapy for AIMSS includes NSAIDs, analgesics, or vitamin D. Still, there is a need for more effective AIMSS management [76]. Therefore, a pilot study by Martínez et al. (2019) demonstrated that olive-derived polyphenol hydroxytyrosol combined with omega-3 fatty acids and curcumin could reduce pain and inflammation (indicated by decreased CRP) in breast cancer patients with aromatase-induced musculoskeletal symptoms [75].
Improved musculoskeletal symptoms were observed in patients with AIMSS after an administration of preparation from Chinese medicine (Yi Shen Jian Gu granules composed of twelve herbs including Caulis trachelospermi (LuoShiTeng), Fructus corni (ShanZhuYu), Phryma leptostachya (TouGuCao), Poria (FuLing), Radix achyranthis bidentatae (NiuXi), Radix angelicae sinensis (DangGui), Radix paeoniae albae (BaiShao), Radix rehmanniae preparatae (ShuDiHuang), Rhizoma chuanxiong (ChuanXiong), Rhizoma corydalis (YanHuSuo), Rhizoma cyperi (XiangFu), and Semen cuscutae (TuSiZi)) [76].
In addition to the side effects of above discussed anticancer strategies, depression, anxiety, and psychosocial distress can occur in up to half of the patients after breast cancer diagnosis and mastectomy. Also, recently emphasized enhanced recovery after surgery (ERAS) protocols highlight the reduction of opioid analgesics and anxiolytics in patients undergoing microvascular breast reconstruction to reduce risk factors such as an overdose or respiratory distress and reduce comorbid psychological symptoms such as depression and anxiety. Shammas et al. (2021) evaluated effects of lavender oil but observed no advantages in treatment of depression, anxiety, sleep, or pain of patients undergoing microvascular breast reconstruction [82]. On the contrary, lavender oil inhaled before breast surgery decreased anxiety in breast cancer patients [83]. Therefore, low-risk therapeutics of natural origin lowering pain, anxiety, and depression still wait to be identified.
In summary, phytochemicals and their mixtures in whole plants exert potent capacity to combat the side effects of current anticancer conventional therapeutic strategies. However, the clinical research in this area can still be considered poor and requires a comprehensive approach that would allow broad use of phytochemicals in clinical practice.
Phytochemicals combined with conventional anticancer agents
Conventional anticancer strategies combined with phytochemicals are a promising strategy in the treatment of breast cancer. An early performed clinical trial (2012) conducted on ten breast cancer patients undergoing radiotherapy demonstrated the potential of EGCG to enhance radiotherapy demonstrated through decreased levels of vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), and reduced activation of matrix metalloproteinase (MMP)-9 and MMP-2 in patients receiving radiotherapy plus EGCG compared to patients receiving radiotherapy alone. Therefore, these results supported the potential of EGCG to serve as an adjuvant against metastatic breast cancer [84]. Similarly, a double-blinded, randomized controlled clinical trial (2015) conducted on fifty-six breast cancer patients revealed that regular onion administration was associated with reduced tumour biomarkers carcinoembryonic antigen (CEA) and cancer antigen 125 (CA-125) during doxorubicin chemotherapy [85].
In addition, as shown in Table 3, also recent breast cancer clinical evaluations provided promising results on the efficacy of phytochemicals enhancing the anticancer effect of conventional therapeutics.
A recent randomized controlled pilot trial by Xu et al. (2021) evaluated the effects of traditional Chinese medicine (based on mixing Poria cocos (Fu Ling), Atractylodes macrocephala (Bai Zhu), Ginger pinellia (Jiang Ban Xia), Fritillaria thunbergii (Zhe Bei Mu), Curcuma aromatica (Yu Jin), Scutellaria baicalensis (Huang Qin), Curcuma zedoaria (E Zhu), Citrus aurantium (Zhi Qiao), Citrus reticulata (Chen Pi), Solanum lyratum (Bai Ying), chicken’s gizzard-membrane (Ji Nei Jin), turtle carapace Trionyx sinensis (Bie Jia), Glycyrrhiza glabra (Gan Cao), and centipede Scolopendra subspinipes (Wu Gong)) in patients receiving chemotherapy for HER2-positive breast cancer. The authors concluded that personalization of traditional Chinese medicine could enhance effectiveness (lower predictive markers CEA, CA 125, CA 153) and mitigate side effects (cardiac events, less significant reduction of white blood cells, better hepatic function) of trastuzumab-containing chemotherapy in HER2-positive breast cancer patients [86]. Moreover, fasting-mimicking diet (FMD) based on a 4-day plant-based low amino-acid substitution food as an adjunct to neoadjuvant chemotherapy for HER2-negative stage II/III resulted in more likely occurring Miller and Payne 4/5 pathological response that indicates 90–100% tumour-cell loss and reduced DNA damage in lymphocytes induced by chemotherapy [87]. Furthermore, a recent comparative, randomized, double-blinded placebo-controlled clinical trial by Saghatelyan (2020) evaluated the efficacy and safety of curcumin combined with paclitaxel in advanced, metastatic breast cancer patients. The combination of curcumin and paclitaxel was superior to a paclitaxel-placebo group in terms of objective response rate (ORR) and physical performance. Also, curcumin demonstrated no safety issues and no reduction of QoL, and could also be an effective agent to reduce fatigue [88]. Arglabin is a sesquiterpene guaianolide γ-lactone isolated from Artemisia glabella [91], an endemic plant of Central Kazakhstan. Long-term results of combination therapy of locally advanced breast cancer including chemotherapeutic regimens and arglabin revealed that arglabin included in AC regimen increases 3-year disease-free survival by 28% when compared with the standard regimen [89]. Fresh yellow onion ameliorated insulin resistance and hyperglycaemia in breast cancer patients during doxorubicin-based chemotherapy. Thus, a high onion intake represents possible promising synergistic effect in doxorubicin-based chemotherapy [90].
In 2017, Meng et al. presented a prospective cohort study protocol to evaluate TCM herbs to treat triple-negative breast cancer described by aggressive behaviour, rapid progression, low disease-free survival, and high risk of recurrence and metastasis. The association between CHM and recurrence and metastasis rate represents the study’s primary objective. In contrast, secondary objectives include the relationship between QoL and CHM and the correlation between symptoms (sleep quality, fatigue, depression, anxiety) related to breast cancer and CHM [22]. The results of the study are to be evaluated.
In summary, recent evidence supports the potential of phytochemicals in combination with conventional anticancer agents. However, expanded comprehensive analyses of the effects of phytochemicals enhancing conventional therapy are necessary to advance breast cancer management and identify better therapeutic strategies.
Phytochemicals in breast cancer treatment
Previously published studies indicate the efficacy of naturally occurring phytochemicals (not combined with conventional anticancer therapies) in the treatment of breast cancer. In a phase IB (2012) [65] and IIB (2015) dose-escalation trial, Crew et al. highlighted the efficacy of polyphenon E, a green tea extract, to affect biomarkers of tumour growth signalling and angiogenesis in hormone-receptor negative breast cancer. The extract specifically decreased serum HGF involved in tumour growth, migration, invasion, and VEGF, essential for tumour angiogenesis [92]. Some other early clinical studies also indicated potent anticancer effects of phytochemicals, based on 12-month dietary changes such as vegetables or fruits among others (2015). The dietary changes positively changed LUMA DNA and LINE-1 DNA methylation [93]. A phenolic compound trans-resveratrol (2012) decreased methylation of tumour suppressor RASSF-1α [94]. In addition, a phase IB dose-escalation study by Perez et al. (2010) demonstrated that Scutellaria barbata (BZL101) is safe and well-tolerated and exerts promising anticancer potential in women with metastatic breast cancer [95].
In addition to earlier dated studies, more recent clinical evaluations (Table 4) evaluated the effects of phytochemicals (not combined with conventional anticancer therapies) in breast cancer therapy.
Long-term follow-up of the Women’s Health Initiative Randomized Trial recently highlighted that low-fat dietary patterns characterized by increased fruits, vegetables, and grains might reduce the risk of death in postmenopausal breast cancer patients [96]. Moreover, Lazzeroni et al. (2017) conducted a presurgical study to evaluate the effects of lecithin formulation of green tea extract (Greenselect Phytosome®, GSP) in early breast cancer patients. Total EGCG content was analysed in all tumour tissues and the concentration was found to be higher than that in normal tissue. Moreover, free EGCG plasma level correlated with decreased Ki67, a marker of tumour cell proliferation, in tumour tissue. Therefore, these results highlight the increase of EGCG bioavailability through oral GSP and its possible antiproliferative effects in breast cancer patients [98]. Similarly, a year earlier, Lazzeroni et al. (2016) demonstrated that silybin-phosphatidylcholine administration (orally bioavailable complex of a flavonoid silybin) resulted in high silybin blood concentration and selective accumulation in breast tumour tissue of early breast cancer patients. These results can serve as a basis for future clinical evaluation of silybin in breast cancer prevention [99]. Moreover, long-term pre-diagnosis consumption of soy may result in an increased expression of tumour suppressor microRNA and genes and decreased expression of oncogenes as demonstrated by over-expressed microRNA-29a-3p and IGF1R and under-expressed KRAS and FGFR4 in TNBC tissues of women with high soy intake [100]. Moreover, the intake of cruciferous vegetables was associated with a decrease in cell proliferation demonstrated by lower protein expression of Ki67 in ductal carcinoma in situ but not in benign or invasive ductal carcinoma tissues [101]. In addition, ten herbs of CHM correlated with favourable survival outcomes in metastatic breast cancer patients and the bioinformatic analyses suggest inhibition of HSP90, ERα, and TOP-II related pathway as a potential mechanism of their anticancer action [97]. The potential anticancer effects of the phytochemicals were also evaluated in breast cancer survivors. Apart from the actual therapy of breast cancer, the understanding of whether post-diagnosis lifestyle (characterized by high intake of fruit and vegetable, low energy-dense food, regular physical activity, and healthy body weight) also affects the outcome of breast cancer survivors in terms of favourable inflammatory, metabolic, hormonal, and DNA methylation changes decreasing the risk of recurrence. A short-term dietary intervention on nutrition education exerted efficacy in increasing vegetable and fruit intake in Hispanic breast cancer survivors and altered biomarkers of breast cancer recurrence risk—borderline significant increase in global DNA methylation [102].
Last but not least, Teixeira et al. (2017) evaluated the bioavailability and metabolism of ellagitannins and anthocyanins after the consumption of native Brazilian cherry–grumixama fruit by humans, followed by the analysis of its anticancer activity in vitro. Eventually, phenolic acids and urolithin conjugates were the primary metabolites circulating and excreted in the urine. The subjects were classified as high and low urinary metabolite excretors demonstrating interindividual variability in the metabolism of polyphenols. Also, these metabolites were effective in inhibiting cell proliferation and G2/M cell cycle arrest in breast cancer MDA-MB-231 cells in vitro [103].
Despite already published clinical trials, several studies registered at clinicaltrials.gov deals with the potent efficacy of phytochemicals in breast cancer, for example:
-
The intervention of whole-food, plant-based nutrition in metastatic breast cancer patients (ClinicalTrials.gov Identifier: NCT03045289)
-
The response of overweight postmenopausal women with breast cancer to exercise and a plant-based diet (ClinicalTrials.gov Identifier: NCT04298086)
-
The impact of plant extracted natural compounds on breast cancer survival time and regression at stage IV (ClinicalTrials.gov Identifier: NCT00910884)
In summary, the above-discussed results of clinical studies or overview of registered clinical trials point to a poor clinical analysis of the potential effects of phytochemicals without the intervention of conventional therapeutics to treat breast cancer.
Potential limitations of effective use of phytochemicals in clinical practice
Extensive metabolism of naturally occurring plant secondary metabolites is considered a limitation of their bioavailability and bioactivity in vivo. The metabolization of phytochemicals occurs in the small and large intestine, and in the liver through associated phase I and II metabolism. Moreover, the absorption, distribution, metabolism, and elimination of phytochemicals and thus the circulating concentrations, elimination, and tissue exposure to the phytochemical are affected by age, sex, genotype, habitual diet, prescribed medications, and the gut microbiome. Despite the role of the factors on the side of the individual, the metabolism of phytochemicals is also affected by the structural complexity of phytochemicals alone [12, 104]. However, despite the described low bioavailability and bioactivity of phytochemicals in organisms, preclinical in vivo studies demonstrate a potent anticancer efficacy of whole plant food in animal models [29, 35, 42, 43, 48, 105]. Furthermore, some metabolites exert a better physiological function when compared with their precursor [12, 106].
Phytochemicals are generally considered safe and well-tolerated but several minor to more severe side effects have been also observed, e.g. mild gastro-intestinal symptoms, haemolytic anaemia, increased risk of hepatotoxicity, or toxic flavonoid-drug interactions [12, 107, 108]. Therefore, the correct dosage of phytochemicals is essential, depending on various factors, including the individual’s genetic background under the principles of predictive, preventive, and personalized medicine.
Conclusions and expert recommendations for primary, secondary, and tertiary care in overall breast cancer management
Nanotechnology represents nanometric (< 500 nm) delivery systems that can enhance the bio-accessibility and bioavailability of hydrophobic compounds and can be used as drug-delivery vehicles, especially in targeted and combination therapy [109, 110]. In humans, phytochemicals exert poor bioavailability and absorption, rapid clearance, resistance, and toxicity. The reduction of mentioned disadvantages by using its nanoparticles is in the infancy of clinical trials but represents a huge potential in future cancer strategies [111]. Small particle sizes and unique materials used in delivery systems increase the stability and resistance to enzymatic activity in the gastrointestinal tract [112].
The extensive preclinical research revealed that phytochemical nanoparticles effectively target drug delivery with less/no side effects [113,114,115,116,117,118]. On the other hand, there is still insufficient evidence in the clinical sphere. Food and Drug Administration (FDA) approved several liposomes and polymer-based therapeutic nanoparticles for clinical use. The chemotherapeutic nanoparticles such as Doxil® (liposome-encapsulated doxorubicin), Abraxane® (albumin-bound paclitaxel), and Oncaspar® (PEG-Asparaginase) have emerged on the pharmaceutical market to date [111]. In terms of phytochemical nanoparticles, in a randomized, multicentre, parallel design in six female patients with invasive breast carcinoma (stage IIIA or IIIB), the nano-Ayurvedic medicine-gold nanoparticles-based drug along with the standard of care treatment (doxorubicin and cyclophosphamide) exhibited 100% clinical benefits compared to patients with standard of care only [118].
Nanomedicine, the alternative drug delivery and improvement of the treatment efficacy, could represent an innovative way in cancer treatment management in the future (e.g. replacement of current anticancer drugs). Still more detailed clinical studies are needed.
Primary care is at the forefront of the paradigm change in breast cancer management from reactive to the predictive, preventive, and personalized approach
Breast cancer is a systemic multi-factorial disease initiated towards increasing health risks such as internal and external stress factors on one hand and, on the other hand, insufficiently effective protection mechanisms against the disease development [119]. The disease is progressing over years from sub-optimal health conditions to the clinical manifestation of potentially metastatic breast cancer. The time period between a reversible damage to health and irreversible organ damage with cascading complications is the operating timeframe for the primary care in breast cancer prediction and individualized protection. To this end, the majority of breast cancer cases are preventable that makes primary care to the key point in the paradigm change from the currently applied reactive disease management to the cost-effective 3PM approach [6, 7]. Health risk assessment followed by targeted damage-mitigating measures and protection tailored to the individualized patient profile are instrumental to reverse health damage at the level of sub-optimal health [120, 121]. As demonstrated above, an application of phytochemicals in the framework of primary care might be a particularly cost-effective approach exemplified by the evidence-based protection against the non-physiologic inflammation [35] and mitochondrial dysfunction [122] as well as against the Warburg malignant transformation [38]. In 2018, Polivka J Jr. et al. published a strategic article which later on has been distinguished by Springer-Nature as groundbreaking scientific findings that could help humanity and protect our planet in category “Medicine and Public Health”. The article presented new concepts of 3P medicine focused on the primary care and targeted prevention of one of the most aggressive and devastating BC subtypes, namely the pregnancy-associated breast cancer (PABC) [5]. The current article follows the principles and innovation of the distinguished publication and details a protective approach applicable to persons at high PABC risk.
Secondary care: risk assessment, patient stratification, and targeted prevention of metastatic breast cancer
Secondary care in breast cancer management is essential to identify affected individuals and to protect them against breast cancer-associated metastatic disease. Early BC diagnosis utilising non-invasive liquid biopsy approach is highly beneficial to improve individual outcomes [8, 123]. Furthermore, from the predictive diagnostic point of view, specifically patients’ phenotyping, for example, characteristic for “pre-metastatic niches” in individuals with the Flammer syndrome phenotype [124] and liquid biopsy-based risk assessment are instrumental to estimate metastatic potential of clinically manifested breast cancer in each individual case. Multiomic targets including disease- and stage-specific cell-free nucleic acid patterns and enumeration of circulating tumour cells (CTCs density in blood stream) are highly recommended for secondary prevention in overall breast cancer management [8]. For the stratified patients, flavonoids per evidence are of great clinical utility as an effective sensitizer for anti-cancer therapy [125]. Finally, patients stratified as being highly predisposed to metastatic BC might strongly benefit from the administration of low-toxicity natural anticancer agents targeting specifically CTCs [126].
Natural substances in secondary cancer care: potential protection of treated cancer patients against stroke
Treated cancer patients frequently die of a non-cancer cause well exemplified by stroke. Stroke in cancer may occur as a severe comorbidity or resulting from the cancer treatment; the described cases are non-bacterial thrombotic endocarditis, hypercoagulability, therapy, or direct tumour compression of blood vessels [127]. Bang et al. stated that one in seven to eight patients with ischemic stroke also has hidden or known cancer while cancer-related coagulopathy is a mechanism of stroke in 40% of them. Thrombin generation causing stroke related to coagulopathy is enhanced by both malignancy itself and cancer treatment (chemotherapy). Furthermore, a significantly increased risk of stroke may result from accelerated atherosclerosis—the side effect of radiotherapy. To this end, cancer and stroke share common risks such as vascular dysregulation and ischemic lesions [, 5, 124, 128, 129], further pronounced under the cancer treatment conditions [129, 130]. The study by Zaorsky et al. concluded that the risk of stroke among cancer patients is twice as high as that of the general population, particularly increasing later on in life. The study demonstrates high plurality of strokes in patients older than 40 years diagnosed with cancer of prostate, breast, and colorectum. Further breast cancer patients co-diagnosed with sleep disorders are at significantly increased stroke risk [131]. Consequently, risk assessment and advanced protective strategies in cancer treatments focused on individualized protection against stroke are strongly recommended [127].
Except cancer, naturally occurring phytochemicals and plant-based diet (rich in vegetable, fruit, grains, and olive oil also known as a Mediterranean diet pattern) exert efficacy in the protection against stroke, among others [132, 133]. The stroke-preventive activity of polyphenols is based on the effects on the cardio- and cerebrovascular system while their efficacy is suggested also when administered after the stroke onset and thus promoting the recovery of stroke patients [134]. An imbalance between antioxidants and pro-oxidants can result in cell damage, autophagy, apoptosis, and necrosis during stroke. To this end, potent anti-oxidative effects against stress protecting cells from damage are attributed to propolis that is rich in phenolics, flavonoids, and terpenes. Therefore, stroke-predisposed patients may strongly benefit from the daily supplementation with propolis [135]. Moreover, findings of the recently performed clinical study demonstrated that moderate habitual intake of flavonoid-rich foods results in lower risk of ischemic stroke [136]. Similarly, higher consumption of flavonoid-rich food (particularly citrus fruit, grapes, strawberries) was associated with a decreased risk of stroke in Japanese women [137].
The above-mentioned clinical trials demonstrating the efficacy of phytochemical-rich food in decreasing the risk of stroke have been conducted on subjects without cancer history [136, 137]. Further recent evidence supports biological effects of naturally occurring phytochemicals of potential clinical utility also against the cancer-related stroke. The flavonoid isoquercetin has been demonstrated to target protein disulfide isomerase (required for thrombus formation) and thus to improve coagulation markers in advanced cancer patients [138]. Based on the above discussed protective effects against cardiovascular and cerebrovascular damage among others, here we conclude a potential efficacy of naturally occurring phytochemicals against stroke as a frequent complications and cause of death in the patient cohort with treated cancer. Follow-up research to the topic is essential to advance secondary care in overall breast cancer management.
Tertiary care of breast cancer: making palliation to the management of chronic disease
The motivation of the tertiary care is to advance palliation to the management of chronic disease. The task is highly ambitious, since breast cancer is known as capable to spread metastasis to the lymph nodes, bones, lung, liver, and brain, which are the most frequently reported sites of metastatic disease in BC [124]. Flavonoids and their nanotechnologically created derivatives have been reported as being of potentially great clinical utility for tertiary care. Their evident immune-supportive and drug-sensitizing effects which significantly increase sensitivity of malignant cells to anti-cancer therapies up to reversing anti-cancer therapy resistance, are a promising approach complementary to the therapeutic modalities currently applied within the tertiary care [125].
Anti-COVID-19 protection of infected cancer patients
Several studies demonstrated that cancer patients including breast malignancies are at higher risk of severe illness and related deaths from COVID-19 infection. Managing cancer care under pandemic conditions is challenging. A multidisciplinary approach for optimal care of cancer patients in hospital settings is essential [139]. Due to their evident anti-inflammatory, anti-bacterial, and anti-viral properties, flavonoids are of great clinical utility in secondary and tertiary care of COVID-19-infected cancer patients including breast malignancies [125].
Data availability
Not applicable.
Code availability
Not applicable.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49. https://doi.org/10.3322/caac.21660.
Vaz-Luis I, Lin NU, Keating NL, Barry WT, Winer EP, Freedman RA. Factors associated with early mortality among patients with de novo metastatic breast cancer: a population-based study. Oncologist. 2017;22:386–93. https://doi.org/10.1634/theoncologist.2016-0369.
Chung IY, Lee JW, Lee JS, Park YR, Min YH, Lee Y, Yoon TI, Sohn G, Lee SB, Kim J, et al. Interaction between body mass index and hormone-receptor status as a prognostic factor in lymph-node-positive breast cancer. PLoS ONE. 2017;12:e0170311. https://doi.org/10.1371/journal.pone.0170311.
Wang J, Wang J, Li Q, Zhang P, Yuan P, Ma F, Luo Y, Cai R, Fan Y, Chen S, et al. Young breast cancer patients who develop distant metastasis after surgery have better survival outcomes compared with elderly counterparts. Oncotarget. 2017;8:44851–9. https://doi.org/10.18632/oncotarget.15268.
Polivka J, Altun I, Golubnitschaja O. Pregnancy-associated breast cancer: the risky status quo and new concepts of predictive medicine. EPMA J. 2018;9:1–13. https://doi.org/10.1007/s13167-018-0129-7.
Golubnitschaja O, Liskova A, Koklesova L, Samec M, Biringer K, Büsselberg D, Podbielska H, Kunin AA, Evsevyeva ME, Shapira N, et al. Caution, “normal” BMI: health risks associated with potentially masked individual underweight-EPMA Position Paper. EPMA J. 2021;2021:1–22. https://doi.org/10.1007/s13167-021-00251-4.
Wang W, Yan Y, Guo Z, Hou H, Garcia M, Tan X, Anto EO, Mahara G, Zheng Y, Li B, et al. All around suboptimal health — a Joint Position Paper of the Suboptimal Health Study Consortium and European Association for Predictive Preventive and Personalised Medicine. EPMA J. 2021;12:403–33. https://doi.org/10.1007/s13167-021-00253-2.
Crigna AT, Samec M, Koklesova L, Liskova A, Giordano FA, Kubatka P, Golubnitschaj a O. Cell-free nucleic acid patterns in disease prediction and monitoring-hype or hope? EPMA J. 2020;11(4):1–25. https://doi.org/10.1007/s13167-020-00226-x.
Fröhlich H, Patjoshi S, Yeghiazaryan K, Kehrer C, Kuhn W, Golubnitschaja O. Premenopausal breast cancer: potential clinical utility of a multi-omics based machine learning approach for patient stratification. EPMA J. 2018;9:175–86. https://doi.org/10.1007/s13167-018-0131-0.
Goldstein E, Yeghiazaryan K, Ahmad A, Giordano FA, Fröhlich H, Golubnitschaja O. Optimal multiparametric set-up modelled for best survival outcomes in palliative treatment of liver malignancies: unsupervised machine learning and 3 PM recommendations. EPMA J. 2020;11(3):1–11. https://doi.org/10.1007/s13167-020-00221-2.
Yoo S, Kim K, Nam H, Lee D. Discovering health benefits of phytochemicals with integrated analysis of the molecular network, chemical properties and ethnopharmacological evidence. Nutrients. 2018;10:1042. https://doi.org/10.3390/nu10081042.
Liskova A, Koklesova L, Samec M, Smejkal K, Samuel SM, Varghese E, Abotaleb M. Biringer K. Kudela E. Danko J. et al. Flavonoids in cancer metastasis. Cancers 2020;12(6):1498. https://doi.org/10.3390/cancers12061498.
Srivastava SK, Arora S, Singh S, Singh AP. Phytochemicals, microRNAs, and cancer: implications for cancer prevention and therapy. In: Chandra D, editor. Mitochondria as targets for phytochemicals in cancer prevention and therapy. New York, NY: Springer; 2013. pp. 187–206.
Koklesova L, Liskova A, Samec M, Zhai K, Abotaleb M, Ashrafizadeh M, Brockmueller A, Shakibaei M, Biringer K, Bugos O, et al. Carotenoids in cancer metastasis-status quo and outlook. Biomolecules. 2020;10:E1653. https://doi.org/10.3390/biom10121653.
Ruhee RT, Roberts LA, Ma S, Suzuki K. Organosulfur compounds: a review of their anti-inflammatory effects in human health. Front Nutr. 2020;7:64. https://doi.org/10.3389/fnut.2020.00064.
Williamson G. The role of polyphenols in modern nutrition. Nutr Bull. 2017;42:226–35. https://doi.org/10.1111/nbu.12278.
Hussain G, Rasul A, Anwar H, Aziz N, Razzaq A, Wei W, Ali M, Li J, Li X. Role of plant derived alkaloids and their mechanism in neurodegenerative disorders. Int J Biol Sci. 2018;14:341–57. https://doi.org/10.7150/ijbs.23247.
Cory H, Passarelli S, Szeto J, Tamez M, Mattei J. The role of polyphenols in human health and food systems: a mini-review. Front Nutr. 2018;5:87. https://doi.org/10.3389/fnut.2018.00087.
Eguchi R, Ono N, Hirai Morita A, Katsuragi T, Nakamura S, Huang M, Altaf-Ul-Amin M, Kanaya S. Classification of alkaloids according to the starting substances of their biosynthetic pathways using graph convolutional neural networks. BMC Bioinformatics. 2019;20:380. https://doi.org/10.1186/s12859-019-2963-6.
Heinrich M, Mah J, Amirkia V. Alkaloids used as medicines: structural phytochemistry meets biodiversity-an update and forward look. Mol Basel Switz. 1836;2021:26. https://doi.org/10.3390/molecules26071836.
Poo CL, Dewadas HD, Ng FL, Foo CN, Lim YM. Effect of traditional chinese medicine on musculoskeletal symptoms in breast cancer: a systematic review and meta-analysis. J Pain Symptom Manage. 2021;62:159–73. https://doi.org/10.1016/j.jpainsymman.2020.11.024.
Meng H, Peng N, Yu M, Sun X, Ma Y, Yang G, Wang X. Treatment of triple-negative breast cancer with Chinese herbal medicine: a prospective cohort study protocol. Medicine (Baltimore). 2017;96:e8408. https://doi.org/10.1097/MD.0000000000008408.
Pan S-Y, Litscher G, Gao S-H, Zhou S-F, Yu Z-L, Chen H-Q, Zhang S-F, Tang M-K, Sun J-N, Ko K-M. Historical perspective of traditional indigenous medical practices: the current renaissance and conservation of herbal resources. Evid Based Complement Altern Med ECAM. 2014;2014:525340. https://doi.org/10.1155/2014/525340.
Kapinova A, Kubatka P, Liskova A, Baranenko D, Kruzliak P, Matta M, Büsselberg D, Malicherova B, Zulli A, Kwon TK, et al. Controlling metastatic cancer: the role of phytochemicals in cell signaling. J Cancer Res Clin Oncol. 2019;145:1087–109. https://doi.org/10.1007/s00432-019-02892-5.
Abotaleb M, Samuel S, Varghese E, Varghese S, Kubatka P, Liskova A, Büsselberg D. Flavonoids in cancer and apoptosis Cancers. 2018;11:28. https://doi.org/10.3390/cancers11010028.
Koklesova L, Liskova A, Samec M, Buhrmann C, Samuel SM, Varghese E, Ashrafizadeh M, Najafi M, Shakibaei M, Büsselberg D, et al. Carotenoids in cancer apoptosis-the road from bench to bedside and back. Cancers. 2020;12(9):2425. https://doi.org/10.3390/cancers12092425.
Liskova A, Koklesova L, Samec M, Varghese E, Abotaleb M, Samuel SM, Smejkal K, Biringer K, Petras M, Blahutova D et al. Implications of flavonoids as potential modulators of cancer neovascularity. J Cancer Res Clin Oncol. 2020;146(12):3079–3096. https://doi.org/10.1007/s00432-020-03383-8.
Rathaur P, Johar KSR. Metabolism and pharmacokinetics of phytochemicals in the human body. Curr Drug Metab. 2019;20:1085–102. https://doi.org/10.2174/1389200221666200103090757.
Kubatka P, Uramova S, Kello M, Kajo K, Samec M, Jasek K, Vybohova D, Liskova A, Mojzis J, Adamkov M, et al. Anticancer activities of thymus vulgaris L. in Experimental breast carcinoma in vivo and in vitro. Int J Mol Sci. 2019;20(7):1749. https://doi.org/10.3390/ijms20071749.
Abotaleb M, Liskova A, Kubatka P, Büsselberg D. Therapeutic potential of plant phenolic acids in the treatment of cancer. Biomolecules. 2020;10(2):221. https://doi.org/10.3390/biom10020221.
Liskova A, Kubatka P, Samec M, Zubor P, Mlyncek M, Bielik T, Samuel SM, Zulli A, Kwon TK, Büsselberg D. Dietary phytochemicals targeting cancer stem cells. Molecules. 2019; 24(5):899. https://doi.org/10.3390/molecules24050899.
Banudevi S, Swaminathan S, Maheswari KU. Pleiotropic role of dietary phytochemicals in cancer: emerging perspectives for combinational therapy. Nutr Cancer. 2015;67:1021–48. https://doi.org/10.1080/01635581.2015.1073762.
Choudhari AS, Mandave PC, Deshpande M, Ranjekar P, Prakash O. Phytochemicals in cancer treatment: from preclinical studies to clinical practice. Front Pharmacol. 2020;10:1614. https://doi.org/10.3389/fphar.2019.01614.
Kwaśnik P, Lemieszek MK, Rzeski W. Impact of phytochemicals and plant extracts on viability and proliferation of NK cell line NK-92 - a closer look at immunomodulatory properties of Goji berries extract in human colon cancer cells. Ann Agric Environ Med AAEM. 2021;28:291–9. https://doi.org/10.26444/aaem/133801.
Kubatka P, Mazurakova A, Samec M, Koklesova L, Zhai K, AL-Ishaq R, Kajo K, Biringer K, Vybohova D, Brockmueller A, et al. Flavonoids against non-physiologic inflammation attributed to cancer initiation, development, and progression—3PM pathways. EPMA J. 2021;12:559–87. https://doi.org/10.1007/s13167-021-00257-y.
Thakur VS, Deb G, Babcook MA, Gupta S. Plant phytochemicals as epigenetic modulators: role in cancer chemoprevention. AAPS J. 2014;16:151–63. https://doi.org/10.1208/s12248-013-9548-5.
Guo B, Zhang Y, Hui Q, Wang H, Tao K. Naringin suppresses the metabolism of A375 cells by inhibiting the phosphorylation of C-Src. Tumor Biol. 2016;37:3841–50. https://doi.org/10.1007/s13277-015-4235-z.
Samec M, Liskova A, Koklesova L, Samuel SM, Zhai K, Buhrmann C, Varghese E, Abotaleb M, Qaradakhi T, Zulli A, et al. Flavonoids against the Warburg phenotype—concepts of predictive, preventive and personalised medicine to cut the Gordian knot of cancer cell metabolism. EPMA J. 2020;11:377–98. https://doi.org/10.1007/s13167-020-00217-y.
Koklesova L, Liskova A, Samec M, Qaradakhi T, Zulli A, Smejkal K, Kajo K, Jakubikova J, Behzadi P, Pec M, et al. Genoprotective activities of plant natural substances in cancer and chemopreventive strategies in the context of 3P medicine. EPMA J. 2020;11:261–87. https://doi.org/10.1007/s13167-020-00210-5.
Lagunas-Rangel FA, Bermúdez-Cruz RM. Natural compounds that target DNA repair pathways and their therapeutic potential to counteract cancer cells. Front Oncol. 2020;10: 598174. https://doi.org/10.3389/fonc.2020.598174.
Jasek K, Kubatka P, Samec M, Liskova A, Smejkal K, Vybohova D, Bugos O, Biskupska-Bodova K, Bielik T, Zubor P, et al. DNA methylation status in cancer disease: modulations by plant-derived natural compounds and dietary interventions. Biomolecules. 2019;9(7):289. https://doi.org/10.3390/biom9070289.
Samec M, Liskova A, Kubatka P, Uramova S, Zubor P, Samuel SM, Zulli A, Pec M, Bielik T, Biringer K, et al. The role of dietary phytochemicals in the carcinogenesis via the modulation of miRNA expression. J Cancer Res Clin Oncol. 2019;145:1665–79. https://doi.org/10.1007/s00432-019-02940-0.
Samec M, Liskova A, Koklesova L, Mestanova V, Franekova M, Kassayova M, Bojkova B, Uramova S, Zubor P, Janikova K, et al. Fluctuations of histone chemical modifications in breast, prostate, and colorectal cancer: an implication of phytochemicals as defenders of chromatin equilibrium. Biomolecules. 2019;9(12):829. https://doi.org/10.3390/biom9120829.
Kapinova A, Stefanicka P, Kubatka P, Zubor P, Uramova S, Kello M, Mojzis J, Blahutova D, Qaradakhi T, Zulli A, et al. Are plant-based functional foods better choice against cancer than single phytochemicals? A critical review of current breast cancer research. Biomed Pharmacother Biomedecine Pharmacother. 2017;96:1465–77. https://doi.org/10.1016/j.biopha.2017.11.134.
Zhang Y-J, Gan R-Y, Li S, Zhou Y, Li A-N, Xu D-P, Li H-B. Antioxidant phytochemicals for the prevention and treatment of chronic diseases. Mol Basel Switz. 2015;20:21138–56. https://doi.org/10.3390/molecules201219753.
Kubatka P, Kapinová A, Kružliak P, Kello M, Výbohová D, Kajo K, Novák M, Chripková M, Adamkov M, Péč M, et al. Antineoplastic effects of Chlorella pyrenoidosa in the breast cancer model. Nutr Burbank Los Angel Cty Calif. 2015;31:560–9. https://doi.org/10.1016/j.nut.2014.08.010.
Kubatka P, Kello M, Kajo K, Samec M, Liskova A, Jasek K, Koklesova L, Kuruc T, Adamkov M, Smejkal K, et al. Rhus Coriaria L. (Sumac) demonstrates oncostatic activity in the therapeutic and preventive model of breast carcinoma. Int. J Mol Sci. 2020;22(1):183. https://doi.org/10.3390/ijms22010183.
Kubatka P, Kello M, Kajo K, Samec M, Jasek K, Vybohova D, Uramova S, Liskova A, Sadlonova V, Koklesova L, et al. Chemopreventive and therapeutic efficacy of Cinnamomum zeylanicum L bark in experimental breast carcinoma: mechanistic in vivo and in vitro analyses. Molecules. 2020;25:1399. https://doi.org/10.3390/molecules25061399.
Toledo E, Salas-Salvadó J, Donat-Vargas C, Buil-Cosiales P, Estruch R, Ros E, Corella D, Fitó M, Hu FB, Arós F, et al. Mediterranean diet and invasive breast cancer risk among women at high cardiovascular risk in the PREDIMED Trial: a randomized clinical trial. JAMA Intern Med. 2015;175:1752–60. https://doi.org/10.1001/jamainternmed.2015.4838.
Castelló A, Pollán M, Buijsse B, Ruiz A, Casas AM, Baena-Cañada JM, Lope V, Antolýn S, Ramos M, Muñoz M, et al. Spanish Mediterranean diet and other dietary patterns and breast cancer risk: Case-Control EpiGEICAM Study. Br J Cancer. 2014;111:1454–62. https://doi.org/10.1038/bjc.2014.434.
Fung TT, Chiuve SE, Willett WC, Hankinson SE, Hu FB, Holmes MD. Intake of specific fruits and vegetables in relation to risk of estrogen receptor-negative breast cancer among postmenopausal women. Breast Cancer Res Treat. 2013;138:925–30. https://doi.org/10.1007/s10549-013-2484-3.
Ogunleye AA, Xue F, Michels KB. Green tea consumption and breast cancer risk or recurrence: a meta-analysis. Breast Cancer Res Treat. 2010;119:477–84. https://doi.org/10.1007/s10549-009-0415-0.
Sasanfar B, Toorang F, Maleki F, Esmaillzadeh A, Zendehdel K. Association between dietary total antioxidant capacity and breast cancer: a case-control study in a Middle Eastern country. Public Health Nutr. 2021;24:965–72. https://doi.org/10.1017/S1368980019004397.
Sharif Y, Sadeghi O, Benisi-Kohansal S, Azadbakht L, Esmaillzadeh A. Legume and nuts consumption in relation to odds of breast cancer: a case-control study. Nutr Cancer. 2021;73:750–9. https://doi.org/10.1080/01635581.2020.1773874.
Rigi S, Mousavi SM, Benisi-Kohansal S, Azadbakht L, Esmaillzadeh A. The association between plant-based dietary patterns and risk of breast cancer: a case-control study. Sci Rep. 2021;11:3391. https://doi.org/10.1038/s41598-021-82659-6.
Kord-Varkaneh H, Salehi-Sahlabadi A, Zarezade M, Rahmani J, Tan SC, Hekmatdoost A, Rashidkhani B. Association between Healthy Eating Index-2015 and breast cancer risk: a case-control study. Asian Pac J Cancer Prev APJCP. 2020;21:1363–7. https://doi.org/10.31557/APJCP.2020.21.5.1363.
Romanos-Nanclares A, Toledo E, Sánchez-Bayona R, Sánchez-Quesada C, Martínez-González MÁ, Gea A. Healthful and unhealthful provegetarian food patterns and the incidence of breast cancer: results from a Mediterranean cohort. Nutr Burbank Los Angel Cty Calif. 2020;79–80:110884. https://doi.org/10.1016/j.nut.2020.110884.
Farvid MS, Chen WY, Rosner BA, Tamimi RM, Willett WC, Eliassen AH. Fruit and vegetable consumption and breast cancer incidence: repeated measures over 30 years of follow-up. Int J Cancer. 2019;144:1496–510. https://doi.org/10.1002/ijc.31653.
Masala G, Assedi M, Sera F, Ermini I, Occhini D, Castaldo M, Pierpaoli E, Caini S, Bendinelli B, Ambrogetti D, et al. Can dietary and physical activity modifications reduce breast density in postmenopausal women? The DAMA Study, a randomized intervention trial in Italy. Cancer Epidemiol.Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am Soc Prev Oncol. 2019;28:41–50. https://doi.org/10.1158/1055-9965.EPI-18-0468.
Vahid F, Hatami M, Sadeghi M, Ameri F, Faghfoori Z, Davoodi SH. The association between the Index of Nutritional Quality (INQ) and breast cancer and the evaluation of nutrient intake of breast cancer patients: a case-control study. Nutr Burbank Los Angel Cty Calif. 2018;45:11–6. https://doi.org/10.1016/j.nut.2017.06.011.
Sangaramoorthy M, Koo J, John EM. Intake of bean fiber, beans, and grains and reduced risk of hormone receptor-negative breast cancer: The San Francisco Bay Area Breast Cancer Study. Cancer Med. 2018;7:2131–44. https://doi.org/10.1002/cam4.1423.
Zhang N-Q, Ho SC, Mo X-F, Lin F-Y, Huang W-Q, Luo H, Huang J, Zhang C-X. Glucosinolate and isothiocyanate intakes are inversely associated with breast cancer risk: a case-control study in China. Br J Nutr. 2018;119:957–64. https://doi.org/10.1017/S0007114518000600.
Samavat H, Ursin G, Emory TH, Lee E, Wang R, Torkelson CJ, Dostal AM, Swenson K, Le CT, Yang CS, et al. A randomized controlled trial of green tea extract supplementation and mammographic density in postmenopausal women at increased risk of breast cancer. Cancer Prev Res Phila Pa. 2017;10:710–8. https://doi.org/10.1158/1940-6207.CAPR-17-0187.
van den Brandt PA, Schulpen M. Mediterranean diet adherence and risk of postmenopausal breast cancer: results of a cohort study and meta-analysis. Int J Cancer. 2017;140:2220–31. https://doi.org/10.1002/ijc.30654.
Crew KD, Brown P, Greenlee H, Bevers TB, Arun B, Hudis C, McArthur HL, Chang J, Rimawi M, Vornik L, et al. Phase IB Randomized, double-blinded, placebo-controlled, dose escalation study of polyphenon E in women with hormone receptor-negative breast cancer. Cancer Prev Res Phila Pa. 2012;5:1144–54. https://doi.org/10.1158/1940-6207.CAPR-12-0117.
Cacchio A, Prencipe R, Bertone M, De Benedictis L, Taglieri L, D’Elia E, Centoletti C, Di Carlo G. Effectiveness and safety of a product containing diosmin, coumarin, and arbutin (Linfadren®) in addition to complex decongestive therapy on management of breast cancer-related lymphedema. Support Care Cancer. 2019;27:1471–80. https://doi.org/10.1007/s00520-018-4514-5.
Karbasforooshan H, Hosseini S, Elyasi S, Fani Pakdel A, Karimi G. Topical silymarin administration for prevention of acute radiodermatitis in breast cancer patients: a randomized, double-blind, placebo-controlled clinical trial. Phytother Res PTR. 2019;33:379–86. https://doi.org/10.1002/ptr.6231.
Rafati M, Ghasemi A, Saeedi M, Habibi E, Salehifar E, Mosazadeh M, Nigella Maham M, Sativa L. for Prevention of acute radiation dermatitis in breast cancer: a randomized, double-blind, placebo-controlled, clinical trial. Complement Ther Med. 2019;47:102205. https://doi.org/10.1016/j.ctim.2019.102205.
Zhu W, Jia L, Chen G, Zhao H, Sun X, Meng X, Zhao X, Xing L, Yu J, Zheng M. Epigallocatechin-3-gallate ameliorates radiation-induced acute skin damage in breast cancer patients undergoing adjuvant radiotherapy. Oncotarget. 2016;7:48607–13. https://doi.org/10.18632/oncotarget.9495.
de Souzada SilvaFayh APSLCAPT. Nutritional intervention contributes to the improvement of symptoms related to quality of life in breast cancer patients undergoing neoadjuvant chemotherapy: a randomized clinical trial. Nutrients. 2021;13:589. https://doi.org/10.3390/nu13020589.
Hao W, Shi Y, Qin Y, Sun C, Chen L, Wu C, Bao Y, Liu S. Platycodon grandiflorum protects against anthracycline-induced cardiotoxicity in early breast cancer patients. Integr Cancer Ther. 2020;19:1534735420945017. https://doi.org/10.1177/1534735420945017.
Jafarimanesh H, Akbari M, Hoseinian R, Zarei M, Harorani M. The effect of peppermint (Mentha piperita) extract on the severity of nausea, vomiting and anorexia in patients with breast cancer undergoing chemotherapy: a randomized controlled trial. Integr Cancer Ther. 2020;19:1534735420967084. https://doi.org/10.1177/1534735420967084.
Pelzer F, Tröger W, Nat DR. Complementary treatment with mistletoe extracts during chemotherapy: safety, neutropenia, fever, and quality of life assessed in a randomized study. J Altern Complement Med N Y N. 2018;24:954–61. https://doi.org/10.1089/acm.2018.0159.
Sanaati F, Najafi S, Kashaninia Z, Sadeghi M. Effect of ginger and chamomile on nausea and vomiting caused by chemotherapy in Iranian women with breast cancer. Asian Pac J Cancer Prev APJCP. 2016;17:4125–9.
Martínez N, Herrera M, Frías L, Provencio M, Pérez-Carrión R, Díaz V, Morse M, Crespo MC. A combination of hydroxytyrosol, omega-3 fatty acids and curcumin improves pain and inflammation among early stage breast cancer patients receiving adjuvant hormonal therapy: results of a pilot study. Clin Transl Oncol Off Publ Fed. Span Oncol Soc Natl Cancer Inst Mex. 2019;21:489–98. https://doi.org/10.1007/s12094-018-1950-0.
Peng N, Yu M, Yang G, Fu Q, Xu Y, Yu J, Liu Q, Li C, Xu W, Zhang Y, et al. Effects of the Chinese medicine Yi Shen Jian Gu granules on aromatase inhibitor-associated musculoskeletal symptoms: a randomized, controlled clinical trial. Breast Edinb Scotl. 2018;37:18–27. https://doi.org/10.1016/j.breast.2017.08.003.
Czajka ML, Pfeifer C. Breast cancer surgery. Treasure Island (FL): In StatPearls; StatPearls Publishing; 2021.
Schick J, Ritchie RP, Restini C. Breast cancer therapeutics and biomarkers: past, present, and future approaches. Breast Cancer Basic Clin Res. 2021;15:1178223421995854. https://doi.org/10.1177/1178223421995854.
Nounou MI, ElAmrawy F, Ahmed N, Abdelraouf K, Goda S, Syed-Sha-Qhattal H. Breast cancer: conventional diagnosis and treatment modalities and recent patents and technologies. Breast Cancer Basic Clin Res. 2015;9:17–34. https://doi.org/10.4137/BCBCR.S29420.
Hayakawa S, Ohishi T, Miyoshi N, Oishi Y, Nakamura Y, Isemura M. Anti-cancer effects of green tea epigallocatchin-3-gallate and coffee chlorogenic acid. Molecules. 2020;25:4553. https://doi.org/10.3390/molecules25194553.
Ratre P, Mishra K, Dubey A, Vyas A, Jain A, Thareja S. Aromatase inhibitors for the treatment of breast cancer: a journey from the scratch. Anticancer Agents Med Chem. 2020;20:1994–2004. https://doi.org/10.2174/1871520620666200627204105.
Shammas RL, Marks CE, Broadwater G, Le E, Glener AD, Sergesketter AR, Cason RW, Rezak KM, Phillips BT, Hollenbeck ST. The effect of lavender oil on perioperative pain, anxiety, depression, and sleep after microvascular breast reconstruction: a prospective, single-blinded, randomized, controlled trial. J Reconstr Microsurg. 2021;37:530–40. https://doi.org/10.1055/s-0041-1724465.
Beyliklioğlu A, Arslan S. Effect of lavender oil on the anxiety of patients before breast surgery. J. Perianesthesia Nurs. Off J Am Soc PeriAnesthesia Nurses. 2019;34:587–93. https://doi.org/10.1016/j.jopan.2018.10.002.
Zhang G, Wang Y, Zhang Y, Wan X, Li J, Liu K, Wang F, Liu K, Liu Q, Yang C, et al. Anti-cancer activities of tea epigallocatechin-3-gallate in breast cancer patients under radiotherapy. Curr Mol Med. 2012;12:163–76. https://doi.org/10.2174/156652412798889063.
Jafarpour-Sadegh F, Montazeri V, Adili A, Esfehani A, Rashidi M-R, Mesgari M, Pirouzpanah S. Effects of fresh yellow onion consumption on CEA, CA125 and hepatic enzymes in breast cancer patients: a double- blind randomized controlled clinical trial. Asian Pac J Cancer Prev APJCP. 2015;16:7517–22. https://doi.org/10.7314/apjcp.2015.16.17.7517.
Xu M, Wang Y, Wang H-C. Adjuvant concomitant treatment with traditional chinese medicines in patients receiving chemotherapy for HER2-positive breast cancer: a pilot randomized controlled trial. Complement Ther Clin Pract. 2021;43:101373. https://doi.org/10.1016/j.ctcp.2021.101373.
de Groot S, Lugtenberg RT, Cohen D, Welters MJP, Ehsan I, Vreeswijk MPG, Smit VTHBM, de Graaf H, Heijns JB, Portielje JEA, et al. Fasting mimicking diet as an adjunct to neoadjuvant chemotherapy for breast cancer in the multicentre randomized phase 2 DIRECT Trial. Nat Commun. 2020;11:3083. https://doi.org/10.1038/s41467-020-16138-3.
Saghatelyan T, Tananyan A, Janoyan N, Tadevosyan A, Petrosyan H, Hovhannisyan A, Hayrapetyan L, Arustamyan M, Arnhold J, Rotmann A-R, et al. Efficacy and safety of curcumin in combination with paclitaxel in patients with advanced, metastatic breast cancer: a comparative, randomized, double-blind, placebo-controlled clinical trial. Phytomedicine Int J Phytother Phytopharm. 2020;70:153218. https://doi.org/10.1016/j.phymed.2020.153218.
Zhumakayeva A, Rakhimov K, Sirota V, Arystan L, Madiyarov A, Adekenov S. Long-term results of combination therapy for locally advanced breast cancer. Georgian Med News. 2018;(282):30–5.
Jafarpour-Sadegh F, Montazeri V, Adili A, Esfehani A, Rashidi M-R, Pirouzpanah S. Consumption of fresh yellow onion ameliorates hyperglycemia and insulin resistance in breast cancer patients during doxorubicin-based chemotherapy: a randomized controlled clinical trial. Integr Cancer Ther. 2017;16:276–89. https://doi.org/10.1177/1534735416656915.
He W, Lai R, Lin Q, Huang Y, Wang L. Arglabin is a plant sesquiterpene lactone that exerts potent anticancer effects on human oral squamous cancer cells via mitochondrial apoptosis and downregulation of the MTOR/PI3K/Akt signaling pathway to inhibit tumor growth in vivo. J Buon off J Balk Union oncol. 2018;23:1679–85.
Crew KD, Ho KA, Brown P, Greenlee H, Bevers TB, Arun B, Sneige N, Hudis C, McArthur HL, Chang J, et al. Effects of a green tea extract, polyphenon E, on systemic biomarkers of growth factor signalling in women with hormone receptor-negative breast cancer. J Hum Nutr Diet Off J Br Diet Assoc. 2015;28:272–82. https://doi.org/10.1111/jhn.12229.
Delgado-Cruzata L, Zhang W, McDonald JA, Tsai WY, Valdovinos C, Falci L, Wang Q, Crew KD, Santella RM, Hershman DL, et al. Dietary Modifications, weight loss, and changes in metabolic markers affect global DNA methylation in Hispanic, African American, and Afro-Caribbean breast cancer survivors12. J Nutr. 2015;145:783–90. https://doi.org/10.3945/jn.114.202853.
Zhu W, Qin W, Zhang K, Rottinghaus GE, Chen Y-C, Kliethermes B, Sauter ER. Trans-resveratrol alters mammary promoter hypermethylation in women at increased risk for breast cancer. Nutr Cancer. 2012;64:393–400. https://doi.org/10.1080/01635581.2012.654926.
Perez AT, Arun B, Tripathy D, Tagliaferri MA, Shaw HS, Kimmick GG, Cohen I, Shtivelman E, Caygill KA, Grady D, et al. A phase 1B dose escalation trial of Scutellaria barbata (BZL101) for patients with metastatic breast cancer. Breast Cancer Res Treat. 2010;120:111–8. https://doi.org/10.1007/s10549-009-0678-5.
Chlebowski RT, Aragaki AK, Anderson GL, Pan K, Neuhouser ML, Manson JE, Thomson CA, Mossavar-Rahmani Y, Lane DS, Johnson KC, et al. Dietary modification and breast cancer mortality: long-term follow-up of the Women’s Health Initiative Randomized Trial. J Clin Oncol Off J Am Soc Clin Oncol. 2020;38:1419–28. https://doi.org/10.1200/JCO.19.00435.
Mao Y, Hao J, Jin Z-Q, Niu Y-Y, Yang X, Liu D, Cao R, Wu X-Z. Network pharmacology-based and clinically relevant prediction of the active ingredients and potential targets of Chinese herbs in metastatic breast cancer patients. Oncotarget. 2017;8:27007–21. https://doi.org/10.18632/oncotarget.15351.
Lazzeroni M, Guerrieri-Gonzaga A, Gandini S, Johansson H, Serrano D, Cazzaniga M, Aristarco V, Macis D, Mora S, Caldarella P, et al. A Presurgical study of lecithin formulation of green tea extract in women with early breast cancer. Cancer Prev Res Phila Pa. 2017;10:363–70. https://doi.org/10.1158/1940-6207.CAPR-16-0298.
Lazzeroni M, Guerrieri-Gonzaga A, Gandini S, Johansson H, Serrano D, Cazzaniga M, Aristarco V, Puccio A, Mora S, Caldarella P, et al. A presurgical study of oral silybin-phosphatidylcholine in patients with early breast cancer. Cancer Prev Res Phila Pa. 2016;9:89–95. https://doi.org/10.1158/1940-6207.CAPR-15-0123.
Guo X, Cai Q, Bao P, Wu J, Wen W, Ye F, Zheng W, Zheng Y, Shu X-O. Long-term soy consumption and tumor tissue microRNA and gene expression in triple negative breast cancer. Cancer. 2016;122:2544–51. https://doi.org/10.1002/cncr.29981.
Zhang Z, Atwell LL, Farris PE, Ho E, Shannon J. Associations between cruciferous vegetable intake and selected biomarkers among women scheduled for breast biopsies. Public Health Nutr. 2016;19:1288–95. https://doi.org/10.1017/S136898001500244X.
Greenlee H, Ogden Gaffney A, Aycinena AC, Koch P, Contento I, Karmally W, Richardson JM, Shi Z, Lim E, Tsai W-Y, et al. Long-term diet and biomarker changes after a short-term intervention among Hispanic breast cancer survivors: The ¡Cocinar Para Su Salud! Randomized Controlled Trial. Cancer Epidemiol.Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am Soc Prev Oncol. 2016;25:1491–502. https://doi.org/10.1158/1055-9965.EPI-15-1334.
Teixeira LL, Costa GR, Dörr FA, Ong TP, Pinto E, Lajolo FM, Hassimotto NMA. Potential antiproliferative activity of polyphenol metabolites against human breast cancer cells and their urine excretion pattern in healthy subjects following acute intake of a polyphenol-rich juice of Grumixama (Eugenia brasiliensis Lam.). Food Funct. 2017;8:2266–74. https://doi.org/10.1039/c7fo00076f.
Cassidy A, Minihane A-M. The role of metabolism (and the microbiome) in defining the clinical efficacy of dietary flavonoids1. Am J Clin Nutr. 2017;105:10–22. https://doi.org/10.3945/ajcn.116.136051.
Kubatka P, Uramova S, Kello M, Kajo K, Kruzliak P, Mojzis J, Vybohova D, Adamkov M, Jasek K, Lasabova Z, et al. Antineoplastic effects of clove buds (Syzygium aromaticum L.) in the model of breast carcinoma. J Cell Mol Med. 2017;21:2837–51. https://doi.org/10.1111/jcmm.13197.
Murota K, Nakamura Y, Uehara M. Flavonoid metabolism: the interaction of metabolites and gut microbiota. Biosci Biotechnol Biochem. 2018;82:600–10. https://doi.org/10.1080/09168451.2018.1444467.
Vogiatzoglou A, Mulligan AA, Lentjes MAH, Luben RN, Spencer JPE, Schroeter H, Khaw K-T, Kuhnle GGC. Flavonoid intake in European adults (18 to 64 years). PLoS ONE 2015;10(5):e0128132. https://doi.org/10.1371/journal.pone.0128132.
Galati G, O’Brien PJ. Potential toxicity of flavonoids and other dietary phenolics: significance for their chemopreventive and anticancer properties. Free Radic Biol Med. 2004;37:287–303. https://doi.org/10.1016/j.freeradbiomed.2004.04.034.
Jones D, Caballero S, Davidov-Pardo G. Bioavailability of nanotechnology-based bioactives and nutraceuticals. Adv Food Nutr Res. 2019;88:235–73. https://doi.org/10.1016/bs.afnr.2019.02.014.
Xu X, Ho W, Zhang X, Bertrand N, Farokhzad O. Cancer nanomedicine: from targeted delivery to combination therapy. Trends Mol Med. 2015;21:223–32. https://doi.org/10.1016/j.molmed.2015.01.001.
Kim B, Park J-E, Im E, Cho Y, Lee J, Lee H-J, Sim D-Y, Park W-Y, Shim B-S, Kim S-H. Recent advances in nanotechnology with nano-phytochemicals: molecular mechanisms and clinical implications in cancer progression. Int J Mol Sci. 2021;22:3571. https://doi.org/10.3390/ijms22073571.
Yao K, Chen W, Song F, McClements DJ, Hu K. Tailoring zein nanoparticle functionality using biopolymer coatings: impact on curcumin bioaccessibility and antioxidant capacity under simulated gastrointestinal conditions. Food Hydrocoll. 2018;79:262–72. https://doi.org/10.1016/j.foodhyd.2017.12.029.
Mughees M, Wajid S. Herbal based polymeric nanoparticles as a therapeutic remedy for breast cancer. Anticancer Agents Med Chem. 2021;21:433–44. https://doi.org/10.2174/1871520620666200619171616.
Liu C-H, Wong SH, Tai C-J, Tai C-J, Pan Y-C, Hsu H-Y, Richardson CD, Lin L-T. Ursolic acid and its nanoparticles are potentiators of oncolytic measles virotherapy against breast cancer cells. Cancers. 2021;13:E136. https://doi.org/10.3390/cancers13010136.
Vemuri SK, Banala RR, Mukherjee S, Uppula P, Gpv S, Gurava Reddy AV, Malarvilli T. Novel biosynthesized gold nanoparticles as anti-cancer agents against breast cancer: synthesis, biological evaluation, molecular modelling studies. Mater Sci Eng C Mater Biol Appl. 2019;99:417–29. https://doi.org/10.1016/j.msec.2019.01.123.
Gregoriou Y, Gregoriou G, Yilmaz V, Kapnisis K, Prokopi M, Anayiotos A, Strati K, Dietis N, Constantinou AI, Andreou C. Resveratrol loaded polymeric micelles for theranostic targeting of breast cancer cells. Nanotheranostics. 2021;5:113–24. https://doi.org/10.7150/ntno.51955.
Raj Preeth D, Shairam M, Suganya N, Hootan R, Kartik R, Pierre K, Suvro C, Rajalakshmi S. Green synthesis of copper oxide nanoparticles using sinapic acid: an underpinning step towards antiangiogenic therapy for breast cancer. J Biol Inorg Chem JBIC Publ Soc Biol Inorg Chem. 2019;24:633–45. https://doi.org/10.1007/s00775-019-01676-z.
Khoobchandani M, Katti KK, Karikachery AR, Thipe VC, Srisrimal D, Dhurvas Mohandoss DK, Darshakumar RD, Joshi CM, Katti KV. New approaches in breast cancer therapy through green nanotechnology and nano-Ayurvedic medicine – pre-clinical and pilot human clinical investigations. Int J Nanomedicine. 2020;15:181–97. https://doi.org/10.2147/IJN.S219042.
Golubnitschaja O, Baban B, Boniolo G, Wang W, Bubnov R, Kapalla M, Krapfenbauer K, Mozaffari MS, Costigliola V. Medicine in the early twenty-first century: paradigm and anticipation - EPMA Position Paper 2016. EPMA J. 2016;7:23. https://doi.org/10.1186/s13167-016-0072-4.
Crigna AT, Link B, Samec M, Giordano FA, Kubatka P, Golubnitschaja O. Endothelin-1 axes in the framework of predictive, preventive and personalised (3P) medicine. EPMA J. 2021;12(3):1–41. https://doi.org/10.1007/s13167-021-00248-z.
Koklesova L, Mazurakova A, Samec M, Biringer K, Samuel SM, Büsselberg D, Kubatka P, Golubnitschaja O. Homocysteine metabolism as the target for predictive medical approach, disease prevention, prognosis, and treatments tailored to the person. EPMA J. 2021;12(4):1–29. https://doi.org/10.1007/s13167-021-00263-0.
Koklesova L, Samec M, Liskova A, Zhai K, Büsselberg D, Giordano FA, Kubatka P, Golunitschaja O. Mitochondrial impairments in aetiopathology of multifactorial diseases: common origin but individual outcomes in context of 3P medicine. EPMA J. 2021;12(1):1–14. https://doi.org/10.1007/s13167-021-00237-2.
Zhan X, Li J, Guo Y, Golubnitschaja O. Mass spectrometry analysis of human tear fluid biomarkers specific for ocular and systemic diseases in the context of 3P medicine. EPMA J. 2021;12:449–75. https://doi.org/10.1007/s13167-021-00265-y.
Bubnov R, Polivka J, Zubor P, Konieczka K, Golubnitschaja O. “Pre-metastatic niches” in breast cancer: are they created by or prior to the tumour onset? “Flammer Syndrome” Relevance to Address the Question. EPMA J. 2017;8:141–57. https://doi.org/10.1007/s13167-017-0092-8.
Liskova A, Samec M, Koklesova L, Brockmueller A, Zhai K, Abdellatif B, Siddiqui M, Biringer K, Kudela E, Pec M, et al. Flavonoids as an effective sensitizer for anti-cancer therapy: insights into multi-faceted mechanisms and applicability towards individualized patient profiles. EPMA J. 2021;12(2):155–176. https://doi.org/10.1007/s13167-021-00242-5.
Kejík Z, Kaplánek R, Dytrych P, Masařík M, Veselá K, Abramenko N, Hoskovec D, Vašáková M, Králová J, Martásek P, et al. Circulating tumour cells (CTCs) in NSCLC: from prognosis to therapy design. Pharmaceutics. 1879;2021:13. https://doi.org/10.3390/pharmaceutics13111879.
Zaorsky NG, Zhang Y, Tchelebi LT, Mackley HB, Chinchilli VM, Zacharia BE. Stroke among cancer patients Nat Commun. 2019;10:5172. https://doi.org/10.1038/s41467-019-13120-6.
Polivka J Jr, Polivka J, Pesta M, Rohan V, Celedova L, Mahajani S, Topolcan O, Golubnitschaja O. Risks associated with the stroke predisposition at young age: facts and hypotheses in light of individualized predictive and preventive approach. EPMA J. 2019;10(1):81–99. https://doi.org/10.1007/s13167-019-00162-5.
Bang OY, Chung J-W, Lee MJ, Seo W-K, Kim G-M, Ahn M-J. Cancer-related stroke: an emerging subtype of ischemic stroke with unique pathomechanisms. J Stroke. 2020;22:1–10. https://doi.org/10.5853/jos.2019.02278.
Navi BB, Iadecola C. Ischemic stroke in cancer patients: a review of an underappreciated pathology. Ann Neurol. 2018;83:873–83. https://doi.org/10.1002/ana.25227.
Chen NC, Liao KM, Tian YF, Wu YC, Wang JJ, Ho CH, Hsu CC. Risk of stroke in patients with breast cancer and sleep disorders. J Cancer. 2021;12(22):6749–55. https://doi.org/10.7150/jca.63184.
Román GC, Jackson RE, Gadhia R, Román AN, Reis J. Mediterranean diet: the role of long-chain ω-3 fatty acids in fish; polyphenols in fruits, vegetables, cereals, coffee, tea, cacao and wine; probiotics and vitamins in prevention of stroke, age-related cognitive decline, and Alzheimer disease. Rev Neurol (Paris). 2019;175:724–41. https://doi.org/10.1016/j.neurol.2019.08.005.
Calis Z, Mogulkoc R, Baltaci AK. The roles of flavonols/flavonoids in neurodegeneration and neuroinflammation. Mini Rev Med Chem. 2020;20:1475–88. https://doi.org/10.2174/1389557519666190617150051.
Parrella E, Gussago C, Porrini V, Benarese M, Pizzi M. From preclinical stroke models to humans: polyphenols in the prevention and treatment of stroke. Nutrients. 2020;13:E85. https://doi.org/10.3390/nu13010085.
Sun L-P, Xu X, Hwang H-H, Wang X, Su K-Y, Chen Y-LS. Dichloromethane extracts of propolis protect cell from oxygen-glucose deprivation-induced oxidative stress via reducing apoptosis. Food Nutr Res. 2016;60:30081. https://doi.org/10.3402/fnr.v60.30081.
Parmenter BH, Dalgaard F, Murray K, Cassidy A, Bondonno CP, Lewis JR, Croft KD, Kyrø C, Gislason G, Scalbert A, et al. Habitual flavonoid intake and ischemic stroke incidence in the danish diet, cancer, and health cohort. Am J Clin Nutr. 2021;114:348–57. https://doi.org/10.1093/ajcn/nqab138.
Gao Q, Dong J-Y, Cui R, Muraki I, Yamagishi K, Sawada N, Iso H, Tsugane S. Consumption of flavonoid-rich fruits, flavonoids from fruits and stroke risk: a prospective cohort study. Br J Nutr. 2021;126:1717–24. https://doi.org/10.1017/S0007114521000404.
Zwicker JI, Schlechter BL, Stopa JD, Liebman HA, Aggarwal A, Puligandla M, Caughey T, Bauer KA, Kuemmerle N, Wong E, et al. Targeting protein disulfide isomerase with the flavonoid isoquercetin to improve hypercoagulability in advanced cancer. JCI Insight. 2019;4:e125851. https://doi.org/10.1172/jci.insight.125851.
Pathania AS, Prathipati P, Abdul BA, Chava S, Katta SS, Gupta SC, Gangula PR, Pandey MK, Durden DL, Byrareddy SN, Challagundla KB. COVID-19 and cancer comorbidity: therapeutic opportunities and challenges. Theranostics. 2021;11(2):731–53. https://doi.org/10.7150/thno.51471.
Funding
Open Access funding enabled and organized by Projekt DEAL. The present study was supported by the LISPER project (grant Nr. 313011V446) in bilateral agreement with the European Association for Predictive, Preventive and Personalised Medicine, EPMA, Brussels.
Author information
Authors and Affiliations
Contributions
A.M., P.K., and O.G. were responsible for the conception. The manuscript was drafted by A.M., L.K., M.S., P.K., V.M., V.S., S.H.C., and R.A.I and critically revised by D.B., E.K., K.B., M.A., K.S., K.K., and M.P. O.G. contributed with PPPM/3P medicine expertise and data interpretation in the framework of PPPM. P.K. provided skilled assistance and supervised the overall preparation of the manuscript. O.G., P.K., and F.A.G. contributed with concepts of primary, secondary, and tertiary care in breast cancer management. The figure was prepared by L.K. All the authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interest.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mazurakova, A., Koklesova, L., Samec, M. et al. Anti-breast cancer effects of phytochemicals: primary, secondary, and tertiary care. EPMA Journal 13, 315–334 (2022). https://doi.org/10.1007/s13167-022-00277-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13167-022-00277-2
Keywords
- Breast cancer
- Phytochemicals
- Evidence-based research data
- Individualized patient profiling
- Modifiable risk factors
- Health risk assessment
- Molecular patterns
- Predictive Preventive Personalized Medicine (PPPM/3PM)
- Primary secondary tertiary care
- Treated cancer
- Stroke
- COVID-19
- Translational research
- Plants
- Food
- Cost-effective disease management
- Improved individual outcomes