
Abstract
Congenital disorders (CD) remain an unprioritized health care issue in South Africa with national surveillance underreporting by > 95%. This lack of empiric data contributes to an underestimation of the CD disease burden, resulting in a lack of services for those affected. Modelling offers estimated figures for policymakers to plan services until surveillance is improved. This study applied the Modell Global Database (MGDb) method to quantify the South African CD disease burden in 2012. The MGDb combines birth prevalence data from well-established registries with local demographic data to generate national baseline estimates (birth prevalence and outcomes) for specific early-onset, endogenous CDs. The MGBd was adapted with local South African demographic data to generate baseline (no care) and current care national and provincial estimates for a sub-set of early-onset endogenous CDs. Access to care/impact of interventions was quantified using the infant mortality rate as proxy. With available care in 2012, baseline birth prevalence (27.56 per 1000 live births, n = 32,190) decreased by 7% with 2130 less affected births, with 5400 (17%) less under-5 CD-related deaths and 3530 (11%) more survivors at 5 years, including 4720 (15%) effectively cured and 1190 (4%) less living with disability. Results indicate a higher proportion of CD-affected births than currently indicated by national surveillance. By offering evidence-based estimates, the MGDb may be considered a tool for policymakers until accurate empiric data becomes available. Further work is needed on key CD groups and costing of specific interventions.



Similar content being viewed by others


Data availability
All relevant study data is included in the article.
Notes
Congenital anomalies are defined as macroscopic morphological anomalies present at birth and represented by chapter XVII Congenital malformations, deformations and chromosomal abnormalities of the International Statistical Classification of Diseases and Related Health Problems 10th Revision ICD-10)(World Health Organization 1992, 2006).
Supplementary file TA01-Bottom-Line-WHO-2017-04.xlsx at https://discovery.ucl.ac.uk/id/eprint/1532179/
Serious birth defects cause death or disability in the absence of intervention (Christianson et al. 2006).
Baseline outcomes include fetal deaths/still births; live births; neonatal, infant and under-5 deaths (CD related); deaths from other causes; survivors with disability at age 5; and mean life expectancy.
In the MGDb context, optimal care is defined as the standard of care available in high-income settings with equitable access to services, at any given point in time.
Within the School of Clinical Medicine 2013-2019 and with the KwaZulu Natal Research Innovation and Sequencing Platform (KRISP), School of Laboratory Medicine and Medical Sciences from 2019 to 2020.
A wider review suggested that major differences are uncommon but the possibility should be considered.
For details on this calculation see Blencowe et al. 2018a.
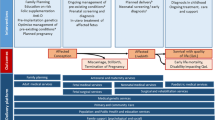
Primary prevention, e.g. folate fortification, genetic counselling etc. resulting in the prevention of affected conceptions.
Secondary preventions, e.g. PND, genetic counselling, option of TOP resulting in the avoidance of affected births.
Tertiary prevention (care) includes newborn screening, diagnosis, therapeutic and surgical interventions, rehabilitation and palliative care, mitigating the impact of affected births and improving outcomes.
University of Cape Town/Groote Schuur Hospital/Red Cross War Memorial Children’s Hospital; Stellenbosch University/Tygerburg Hospital; University of the Free State/Universitas Hospital; University of KwaZulu-Natal/Inkhosi Albert Luthuli Central Hospital (pending registration); National Health Laboratory Service/University of the Witwatersrand
Congenital abnormalities are considered equivalent to congenital anomalies (Pillay-Van Wyk et al. 2014).
References
African Children Policy Forum (2011) Children with disabilities in South Africa: The hidden reality. ACP Forum. https://www.africanchildforum.org/index.php/en/component/com_sobipro/Itemid,0/pid,2/sid,144/. Accessed 25 October 2011
Alwan A, Modell B (2003) Recommendations for introducing genetics services in developing countries. Nat Rev Genet 4(1):61–68. https://doi.org/10.1038/nrg978
Baird PA, Anderson TW, Newcombe HB, Lowry RB (1988) Genetic disorders in children and young adults: a population study. Am J Med Genet 42(5):677
Bamford L, McKerrow N, Barron P, Aung Y (2018) Child mortality in South Africa: Fewer deaths, but better data are needed. S Afr Med J 108(3):25–32. https://doi.org/10.7196/samj.2017.v108i3b.12779
Bittles A, Black ML (2015) Global Patterns and Tables of Consanguinity. Table 1. Consanguineous Marriage in Africa. http://consang.net. Accessed 15 August 2017
Bittles AH, Neel JV (1994) The costs of human inbreeding and their implications for variations at the DNA level. Nat Genet 8(2):117–121. https://doi.org/10.1038/ng1094-117
Blencowe H, Moorthie S, Darlison MW, Gibbons S, Modell B (2018a) Methods to estimate access to care and the effect of interventions on the outcomes of congenital disorders. J Community Genet 9(4):363–376. https://doi.org/10.1007/s12687-018-0359-3
Blencowe H, Moorthie S, Petrou M, Hamamy H, Povey S, Bittles A, Gibbons S, Darlison M, Modell B (2018b) Rare single gene disorders: estimating baseline prevalence and outcomes worldwide. J Community Genet 9(4):397–406. https://doi.org/10.1007/s12687-018-0376-2
Boyle B, Addor M-C, Arriola L, Barisic I, Bianchi F, Csáky-Szunyogh M, de Walle HE, Dias CM, Draper E, Gatt M (2018) Estimating Global Burden of Disease due to congenital anomaly: an analysis of European data. Arch Dis Child Fetal Neonatal Ed 103(1):F22–F28. https://doi.org/10.1136/archdischild-2016-311845
Bundey S, Alam H (1993) A five-year prospective study of the health of children in different ethnic groups, with particular reference to the effect of inbreeding. Eur J Hum Genet 1(3):206–219. https://doi.org/10.1159/000472414
Carter C (1977) Monogenic disorders. J Med Genet 14(5):316–320. https://doi.org/10.1136/jmg.14.5.316
Center for Disease Control and Prevention (2012) CDC's Vision for Public Health Surveillance in the 21st Century. http://www.cdc.gov/mmwr/pdf/other/su6103.pdf. Accessed 1 November 2016
Centers for Disease Control (1986) Comprehensive plan for epidemiologic surveillance. U.S. Department of Health and Human Services, CDC, Atlanta
Christianson A (2012) Medical genetic services for the care and prevention of birth defects. Child Health for All. A manual for southern Africa. ed Oxford University Press Southern Africa, Cape Town, pp 231–241
Christianson A, Modell B (2004) Medical Genetics in Developing Countries. Ann Rev Genomics Hum Genet 5:219–265. https://doi.org/10.1146/annurev.genom.5.061903.175935
Christianson A, Venter P, Modiba J, Nelson M (2000) Development of a primary health care clinical genetic service in rural South Africa–The Northern Province experience, 1990–1996. J Community Genet 3(2):77–84. https://doi.org/10.1159/000051108
Christianson A, Howson C, Modell B (2006) March of Dimes: Global Report on Birth Defects, the Hidden Toll of Dying and Disabled Children. March of Dimes Birth Defects Foundation. http://www.marchofdimes.org/materials/global-report-on-birth-defects-the-hidden-toll-of-dying-and-disabled-children-full-report.pdf Accessed 17 November 2016
Christianson A, Zimmern R, Kristoffersson U, Schmidtke J, Kent A, Raouf R, Barreiro C, Nippert I (2013) Health needs assessment for medical genetic services for congenital disorders in middle-and low-income nations. J Community Genet 4(3):297–308. https://doi.org/10.1007/s12687-013-0150-4
Cousens S, Blencowe H, Stanton C, Chou D, Ahmed S, Steinhardt L, Creanga AA, Tunçalp Ö, Balsara ZP, Gupta S (2011) National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. The Lancet 377(9774):1319–1330. https://doi.org/10.1016/S0140-6736(10)62310-0
Czeizel A (1997) First 25 years of the Hungarian congenital abnormality registry. Teratology 55(5):299–305. https://doi.org/10.1002/(SICI)1096-9926(199705)55:5<299::AID-TERA1>3.0.CO;2-V
Czeizel A, Sankaranarayanan K (1984) The load of genetic and partially genetic disorders in man I. Congenital anomalies: estimates of detriment in terms of years of life lost and years of impaired life. Mutat 128(1):73–103. https://doi.org/10.1016/0027-5107(84)90049-6
Czeizel A, Sankaranarayanan K, Szondy M (1990) The load of genetic and partially genetic diseases in man III. Mental retardation. Mutat Res-Fund Mol M 232(2):291–303. https://doi.org/10.1016/0027-5107(90)90136-R
Czeizel A, Intôdy Z, Modell B (1993) What proportion of congenital abnormalities can be prevented? Br Med J 306:499–503. https://doi.org/10.1136/bmj.306.6876.499
Debas HT, Donkor P, Gawande A, Jamison DT, Kruk ME, Mock CN (2015) Disease Control Priorities, Third Edition : Volume 1. Essential Surgery, World Bank, Washington DC
Declich S, Carter AO (1994) Public health surveillance: historical origins, methods and evaluation. B World Health Organ 72(2):285
Department of Health National Health Insurance: Towards Universal Health Coverage. White Paper on National Health Insurance. Government Gazette (No. 1230) 11 December 2015. Pretoria 2015 Accessed 12 May 2016
Dobbie M, Masebe L, Nhlapo M (2007) The coverage and quality of birth registration data in South Africa, 1998-2005 SS Africa. Accessed 28 October 2016
Dorrington R, Moultrie T (2015) Understanding recent fertility in South Africa. In: 7th African Population Conference. Johannesburg, South Africa
Dorrington R, Bradshaw D, Laubscher R, Nannan N (2020) Rapid Mortality Surveillance Report 2018. https://www.samrc.ac.za/reports/rapid-mortality-surveillance-report-2018. Accessed 18 March 2020
EUROCAT (2009) Special Report: Congenital Heart Defects in Europe 2000-2005. http://www.eurocat-network.eu/content/Special-Report-CHD.pdf. Accessed
EUROCAT (2015) EUROCAT Prevlence Tables. https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data_en. Accessed January 2015
Garenne M, Collinson MA, Kabudula CW, Gómez-Olivé FX, Kahn K, Tollman S (2016) Completeness of birth and death registration in a rural area of South Africa: the Agincourt health and demographic surveillance, 1992–2014. Global Health Action 9:32795. https://doi.org/10.3402/gha.v9.32795
Global Burden of Disease Collaborative Network (2018) Global Burden of Disease Study 2017 (GBD 2017). Institute for Health Metrics and Evaluation (IHME). Seattle, USA.
Hall HI, Correa A, Yoon PW, Braden CR (2012) Lexicon, definitions, and conceptual framework for public health surveillance. MMWR CDC Surveill Summ 61(Suppl):10–14
Hlongwa P, Levin J, Rispel LC (2019) Epidemiology and clinical profile of individuals with cleft lip and palate utilising specialised academic treatment centres in South Africa. PLoS One 14(5). https://doi.org/10.1371/journal.pone.0215931
Johnson LF, Chiu C, Myer L, Davies M-A, Dorrington RE, Bekker L-G, Boulle A, Meyer-Rath G (2016) Prospects for HIV control in South Africa: a model-based analysis. Global Health Action 9:1–12. https://doi.org/10.3402/gha.v9.30314
Joubert J, Rao C, Bradshaw D, Dorrington RE, Vos T, Lopez AD (2012) Characteristics, availability and uses of vital registration and other mortality data sources in post-democracy South Africa. Global health action 5:1–19. https://doi.org/10.3402/gha.v5i0.19263
Kabudula CW, Joubert JD, Tuoane-Nkhasi M, Kahn K, Rao C, Gmez-Oliv FX, Mee P, Tollman S, Lopez AD, Vos T (2014) Evaluation of record linkage of mortality data between a health and demographic surveillance system and national civil registration system in South Africa. Population Health Metrics 12(1):1. https://doi.org/10.1186/s12963-014-0023-z
Kahn K, Garenne ML, Collinson MA, Tollman SM (2007) Mortality trends in a new South Africa: Hard to make a fresh start1. Scand J Public Healt 35(69 suppl):26–34. https://doi.org/10.1080/14034950701355668
Kromberg J, Jenkins T (1982) Prevalence of albinism in the South African Negro. S Afr Med J 61:383–386
Lebese L, Aldous C, Malherbe H (2016) South African congenital disorders data, 2006 - 2014. S Afr Med J 106(10):992–995. https://doi.org/10.7196/samj.2016.v106i10.11314
Liu L, Cousens S, Lawn JE, Black RE (2012) Global regional and national causes of child mortality–Authors' reply. The Lancet 380(9853):1556–1557. https://doi.org/10.1016/s0140-6736(12)61879-0
Lopez AD, Mathers CD (2006) Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann Trop Med Parasitol 100(5-6):481–499. https://doi.org/10.1179/136485906x97417
Luquetti DV, Koifman RJ (2011) Surveillance of birth defects: Brazil and the US. Ciência & Saúde Coletiva 16:777–785. https://doi.org/10.1590/s1413-81232011000700008
Maart S, Amosun S, Jelsma J (2019) Disability prevalence-context matters: A descriptive community-based survey. Afr J Disabil 8:1–8. https://doi.org/10.4102/ajod.v8i0.512
Malherbe HL, Christianson AL, Aldous C (2015) Need for services for the care and prevention of congenital disorders in South Africa as the country's epidemiological transition evolves. S Afr Med J 105(3):186–188. https://doi.org/10.7196/samj.9136
Malherbe H, Aldous C, Woods D, Christianson A (2016) The contribution of congenital disorders to child mortality in South Africa. In: South African Health Review 2017. ed Health Systems Trust, Durban, pp 137–152
Malherbe HL, Christianson A, Woods D, Aldous C (2018a) Contribution congenital disorders to neonatal mortality in South Africa. S Afr Med J 108(7). https://doi.org/10.7196/samj.2018.v108i7.13393
Malherbe HL, Christianson AL, Woods D, Aldous C (2018b) Under-5 mortality and the contribution of congenital disorders in South Africa. S Afr Med J 108(6):447–448. https://doi.org/10.7196/samj.2018.v108i6.13331
Matthews T, MacDorman M, Thoma M (2015) Infant Mortality Statistics From the 2013 Period Linked Birth/Infant Death Data Set. Vital National Statistics Reports; vol 64 no 9. . https://stacks.cdc.gov/view/cdc/32752. Accessed 19 September 2016
Mocumbi AO, Lameira E, Yaksh A, Paul L, Ferreira MB, Sidi D (2011) Challenges on the management of congenital heart disease in developing countries. Int J Cardiol 148(3):285–288
Modell B (2017) The Modell Global Database of Congenital Disorders. http://mgdb.info. Accessed 15 Jan 2018
Modell B, Modell M (1992) Towards a healthy baby: Congenital disorders and the new genetics in primary health care. Oxford University Press, New York
Modell B, Berry RJ, Boyle CA, Christianson A, Darlison M, Dolk H, Howson CP, Mastroiacovo P, Mossey P, Rankin J (2012) Global regional and national causes of child mortality. The Lancet 380(9853):1556. https://doi.org/10.1016/S0140-6736(12)61878-9
Modell B, Darlison M, Moorthie S, Blencowe H, Petrou M, Lawn J (2016) Epidemiological methods in community genetics and the Modell Global Database of Congenital Disorders (MGDb).
Modell B, Darlison M, Malherbe H, Moorthie S, Blencowe H, Mahaini R, El-Adawy M (2018a) Congenital disorders: epidemiological methods for answering calls for action. J Community Genet 9(4):335–340. https://doi.org/10.1007/s12687-018-0390-4
Modell B, Darlison MW, Lawn JE (2018b) Historical overview of development in methods to estimate burden of disease due to congenital disorders. J Community Genet 9(4):341–345. https://doi.org/10.1007/s12687-018-0382-4
Modell B, Darlison MW, Malherbe H, Moorthie S, Blencowe H, Mahaini R, El-Adawy M (2018c) Congenital disorders: epidemiological methods for answering calls for action. J Community Genet 9:335–340. https://doi.org/10.1007/s12687-018-0390-4
Moorthie S, Blencowe H, Darlison MW, Gibbons S, Lawn JE, Mastroiacovo P, Morris JK, Modell B (2018a) Chromosomal disorders: estimating baseline birth prevalence and pregnancy outcomes worldwide. J Community Genet 9(4):377–386. https://doi.org/10.1007/s12687-017-0336-2
Moorthie S, Blencowe H, Darlison MW, Lawn J, Morris JK, Modell B, Bittles A, Blencowe H, Christianson A, Cousens S (2018b) Estimating the birth prevalence and pregnancy outcomes of congenital malformations worldwide. J Community Genet 9(4):387–396. https://doi.org/10.1007/s12687-018-0384-2
Moorthie S, Blencowe H, Darlison MW, Lawn JE, Mastroiacovo P, Morris JK, Modell B (2018c) An overview of concepts and approaches used in estimating the burden of congenital disorders globally. J Community Genet 9(4):347–362. https://doi.org/10.1007/s12687-017-0335-3
Morris JK, Alberman E, Scott C, Jacobs P (2008) Is the prevalence of Klinefelter syndrome increasing? Eur J Hum Genet 16(2):163–170. https://doi.org/10.1038/sj.ejhg.5201956
Mossey PA, Little J (2002) Cleft lip and Palate: From Origin to Treatment. Epidemiology of oral clefts: an international perspective. ed. Oxford University Press, New York, pp 127–158
Nannan N, Dorrington R, Bradshaw D (2019) Estimating completeness of birth registration in South Africa, 1996 - 2011. Bull World Health Organ 97(7):468–476. https://doi.org/10.2471/BLT.18.222620
National Perinatal Morbidity, Mortality Committee (2017) Saving Babies 2014-2016. Triennial report on perinatal mortality in South Africa. https://www.westerncape.gov.za/assets/departments/health/napemmco_triennial_report_2014-2016_saving_babies.pdf. Accessed 9 May 2015
Nippert I, Christianson A, Gribaldo L, Harris H, Horovitz D, Randa K, Kent A, Kristoffersson U, Padilla C, Penchaszadeh V (2013) Genetic Testing in Emerging Economies (GenTEE). Summary Report. Publications Office of the European Union. https://ec.europa.eu/jrc/en/publication/eur-scientific-and-technical-research-reports/genetic-testing-emerging-economies-gentee. Accessed 12 May 2016
Ozgediz D, Langer M, Kisa P, Poenaru D (2016) Pediatric surgery as an essential component of global child health. Semin Pediatr Surg 25(1):3–9. https://doi.org/10.1053/j.sempedsurg.2015.09.002
Pillay-Van Wyk V, Laubscher R, Msemburi W, Dorrington R, Groenewald P, Vos T, Matzopoulos R, Prinsloo M, Nojilana B, Nannan N, Somdyala N, Sithole N, Neethling I, Nicol E, Rossouw A, Joubert J, Bradshaw D (2014) Second South African National Burden of Disease Study: Data cleaning, validation and SA NBD List. http://www.mrc.ac.za/bod/reports.htm. Accessed 1 June 2016
Republic of South Africa Births and Deaths Registration Act No. 51 (1992) Government Gazette 13953 6 May https://www.gov.za/documents/births-and-deaths-registration-act. Accessed 28 October 2016
Republic of South Africa Births and Deaths Registration Amendment Act No.18 (2010) Government Gazette 33851 7 December https://www.gov.za/documents/births-and-deaths-registration-amendment-act-3. Accessed 28 October 2016
Republic of South Africa Choice on Termination of Pregnancy Act No. 92 (1996) Government Gazette 17602 22 November http://www.gov.za/sites/www.gov.za/files/Act92of1996.pdf. Accessed 25 May 2016
Sartorius BK, Sartorius K, Chirwa TF, Fonn S (2011) Infant mortality in South Africa-distribution, associations and policy implications, 2007: an ecological spatial analysis. Int J Health Geogr 10(1):61. https://doi.org/10.1186/1476-072x-10-61
Sayed AR, Bourne D, Pattinson R, Nixon J, Henderson B (2008) Decline in the prevalence of neural tube defects following folic acid fortification and its cost-benefit in South Africa. Birth Defects Res A Clin Mol Teratol 82(4):211–216. https://doi.org/10.1002/bdra.20442
Sitkin NA, Farmer DL (2016) Congenital anomalies in the context of global surgery. Semin Pediatr Surg 25(1):15–18. https://doi.org/10.1053/j.sempedsurg.2015.09.004
Sitkin NA, Ozgediz D, Donkor P, Farmer DL (2015) Congenital anomalies in low-and middle-income countries: the unborn child of global surgery. World J Surg 39(1):36–40
Statistics South Africa (2012) Cause of death vital registration data for congenital anomalies 2012. http://nesstar.statssa.gov.za:8282/webview/. Accessed 9 July 2020
Statistics South Africa (2014) Census 2011. Profile of persons with disabilities in South Africa. http://www.statssa.gov.za/?p=3180. Accessed 5 September 2014
Stevens GA, Alkema L, Black RE, Boerma JT, Collins GS, Ezzati M, Grove JT, Hogan DR, Hogan MC, Horton R (2016) Guidelines for accurate and transparent health estimates reporting: The GATHER statement. PLoS Med 13(6):e1002056. https://doi.org/10.1371/journal.pmed.1002056
Stevenson AC (1959) The load of hereditary defects in human populations. Radiation Research Supplement 1:306–325. https://doi.org/10.2307/3583647
Stevenson AC, Johnston HA, Stewart M, Golding DR (1966) Congenital malformations. A report of a study of series of consecutive births in 24 centres. B World Health. Organ 34(Suppl):9
Tennant PW, Pearce MS, Bythell M, Rankin J (2010) 20-year survival of children born with congenital anomalies: a population-based study. The lancet 375(9715):649–656. https://doi.org/10.1016/s0140-6736(09)61922-x
Trimble BK, Doughty JH (1974) The amount of hereditary disease in human populations. Ann Hum Genet 38(2):199–223. https://doi.org/10.1111/j.1469-1809.1974.tb01951.x
United Nations Department of Economic and Social Affairs PD (2019) World Population Prospects 2019. https://population.un.org/wpp/. Accessed 7 April 2020
United Nations Sustainable Development Goal 3: Ensure Healthy Lives and Promote Wellbeing for All and at All Ages. http://www.un.org/sustainabledevelopment/health/. Accessed 13 January 2016
Visootsak J, Graham JM (2006) Klinefelter syndrome and other sex chromosomal aneuploidies. Orphanet J Rare Dis 1(1):42. https://doi.org/10.1186/1750-1172-1-42
Walani SR, Biermann J (2017) March of Dimes Foundation: leading the way to birth defects prevention. Public Health Rev 38:12. https://doi.org/10.1186/s40985-017-0058-3
Wellesley D, Dolk H, Boyd PA, Greenlees R, Haeusler M, Nelen V, Garne E, Khoshnood B, Doray B, Rissmann A (2012) Rare chromosome abnormalities, prevalence and prenatal diagnosis rates from population-based congenital anomaly registers in Europe. Eur J Hum Genet 20(5):521–526. https://doi.org/10.1038/ejhg.2011.246
World Health Assembly (2010) Sixty-Third World Health Assembly - Resolution 63.17. Birth Defects. http://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_R17-en.pdf. Accessed 2 September 2014
World Health Organization (1985) Community approaches to the control of hereditary diseases. Report of a WHO Advisory Group, Geneva, 3-5 October 1985. World Health Organization. https://apps.who.int/iris/handle/10665/62324. Accessed 12 May 2016
World Health Organization (1992) International Statistical Classification of Diseases and Related Health Problems. 10th revision. https://icd.who.int/browse10/2016/en. Accessed 1 June 2016
World Health Organization (1993) Guidelines for the development of national programmes for monitoring birth defects. World Health Organization. https://apps.who.int/iris/handle/10665/61536. Accessed 25 September 2016
World Health Organization (1996) Control of hereditary diseases: report of a WHO scientific group 1993, Geneva, Switzerland. https://apps.who.int/iris/handle/10665/41846. Accessed 12 May 2016
World Health Organization (1999) Services for the Prevention and Management of Genetic Disorders and Birth Defects in Developing Countries. Report of a Joint WHO/WAOPBD Meeting, The Hague, 5-7 January 1999. World Health Organization. https://apps.who.int/iris/handle/10665/66501. Accessed 12 May 2016
World Health Organization (2006) Management of Birth Defects and Haemoglobin Disorders. Report of a Joint who-March of Dimes Meeting. Geneva, Switzerland, 17-19 May 2006. World Health Organization. http://www.who.int/genomics/publications/WHO-MODreport-final.pdf?ua=1. Accessed 20 February 2016
World Health Organization (2015) World Health Statistics 2015. World Health Organization. https://www.who.int/gho/publications/world_health_statistics/2015/en/. Accessed 14 February 2016
World Health Organization (2020) WHO Mortality Database. https://www.who.int/healthinfo/mortality_data/en/. Accessed 1 April 2020
Wren C, Irving CA, Griffiths JA, O’Sullivan JJ, Chaudhari MP, Haynes SR, Smith JH, Hamilton JL, Hasan A (2012) Mortality in infants with cardiovascular malformations. Eur J Pediatr 171(2):281–287. https://doi.org/10.1007/s00431-011-1525-3
Acknowledgements
Thank you to Prof Rob Dorrington, Centre for Actuarial Research (CARe), University of Cape Town, for providing demographic data for use in this study; Prof Debbie Bradshaw, Burden of Disease Unit, South African Medical Research Council for valuable advice; and Statistics South Africa (StatsSA) for providing 2012 vital registration data sets which, although not used in the final modelling process, were key in the decision-making process at the data-gathering stage of this study.
Code availability
Not applicable.
Funding
This research was funded by the University of KwaZulu Natal (UKZN), initially via PhD (2013–2016) and Post-Doctoral (2017–2019) bursaries awarded to HM by the College of Health Sciences, UKZN, and subsequently by UKZN APACHE Flagship Post-Doctoral Research Scholarship (2019—to date) via the KwaZulu Natal Research, Innovation and Sequencing Platform (KRISP).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Methodology and source material preparation: Bernadette Modell, Helen Malherbe, Arnold Christianson and Matthew Darlison. Data collection, modelling and analysis were performed by Helen Malherbe, Bernadette Modell and Colleen Aldous. The first draft of the manuscript was written by Helen Malherbe with detailed input by Bernadette Modell with all authors providing feedback on early versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This article does not contain any studies with human or animal subjects performed by any of the authors.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflicts of interest
Helen Malherbe was the Honorary Chair of Genetic Alliance South Africa (NPO: 001-029) until March 2020 and was appointed as a (Honorary) Director of Rare Diseases South Africa in April 2020. Colleen Aldous declares she has no conflict of interest. Arnold Christianson declares he has no conflict of interest. Matthew Darlison declares he has no conflict of interest. Bernadette Modell declares she has no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Malherbe, H.L., Aldous, C., Christianson, A.L. et al. Modelled epidemiological data for selected congenital disorders in South Africa. J Community Genet 12, 357–376 (2021). https://doi.org/10.1007/s12687-021-00513-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12687-021-00513-8