
Abstract
Objectives
Self-compassion has been proposed as a mechanism of change in mindfulness-based programmes (MBPs). The current study systematically reviewed the evidence for the effect of MBPs on self-compassion, in randomised controlled trials addressing broad mental health outcomes (depression, anxiety and stress) in nonclinical populations, and statistically synthesisesd these findings in a meta-analysis.
Methods
Three databases were systematically searched, and pre-post programme between group effect sizes (Hedges g) were calculated and synthesised using meta-analytic procedures. Correlation between change in self-compassion and distress (r) was also assessed. Moderator analyses were conducted and publication bias was assessed.
Results
Twenty-six studies met inclusion criteria (n = 598). A significant medium effect of pre-post change on self-compassion was found for MBPs compared to control conditions (g = 0.60, 95% CI = 0.41 to 0.80, p < 0.001). There was significant heterogeneity in the study sample, and no differences found for any of the moderators tested. There was no strong evidence for publication bias. Meta-analysis of correlation between change in self-compassion and distress was underpowered and found no significant effect. The improvement in self-compassion following MBI was not always consistent with improvements in depression or anxiety.
Conclusions
The results suggest that MBPs can increase self-compassion in nonclinical populations, though the moderators of this effect remain unknown. Methodological limitations include small sample sizes, over-reliance on wait-list control conditions and limitations in how self-compassion is measured. Theoretical and clinical implications of the review, and future research directions, are also discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Self-compassion has been shown to correlate negatively with depression, anxiety and stress in both clinical (e.g. Costa and Pinto-gouveia 2011; Van Dam et al. 2011) and nonclinical (e.g. Gilbert et al. 2011; Körner et al. 2015; Roemer et al. 2009) populations. Whilst there is ongoing debate around the definition of self-compassion (Gilbert 2009; Neff 2003a, b; Strauss et al. 2016), one self-report measure (the Self-Compassion Scale, Neff 2003b) has been predominantly used to measure this construct across a large number of studies. One meta-analysis (MacBeth and Gumley 2012) found a large overall effect size (r = − 0.54) for the relationship between psychopathology and self-compassion in both clinical and nonclinical studies. However, many of the studies included in the review were predominantly cross sectional and correlational, providing little information about whether there is a causal link between self-compassion and mental health outcomes, and indeed the direction of this link. Other studies have focused on the positive effects of self-compassion, showing for example positive correlations between self-compassion and wellbeing (Zessin et al. 2015) as well as happiness, optimism and positive affect (Neff et al. 2007). Taken together, these findings illustrate the potential benefits of enhancing self-compassion in nonclinical populations, where high-stress environments and sub-clinical levels of psychological distress exist (e.g. Garlow et al. 2008; Schaufeli et al. 2009).
Self-compassion has also been implicated as one of the processes of change in mindfulness-based programmes (MBPs). Mindfulness is commonly defined as “a practice of awareness that emerges through paying attention on purpose, in the present moment, non-judgementally to things as they are” (Kabat-Zinn 1994, p.4). The format of manualized, 8-week group-based sessions focusing on meditation, psychoeducation and experiential inquiry-led facilitation of insight and understanding originates from Mindfulness-Based Stress Reduction (MBSR: Kabat-Zinn 1990) and has been adapted and applied to a variety of diagnoses and manifestations of psychological distress such as depression (MBCT: Segal et al. 2002), substance abuse (MBSR: Bowen et al. 2014) and psychosis (PBCT: Chadwick 2006). Reviews of MBPs have found them efficacious for stress (Chiesa and Serretti 2009), depressive relapse (Kuyken et al. 2016) and current depression (Strauss et al. 2014), although results have been more equivocal for anxiety (Hofmann et al. 2010; Strauss et al. 2014). There is also increasing evidence that MBPs reduce psychological distress and increase wellbeing in nonclinical populations. This has been found in both standard 8-week group-delivered formats as well as brief (as short as 2-week) online self-help programmes (Cavanagh et al. 2013; Chiesa and Serretti 2009; Eberth and Sedlmeier 2012; Gu et al. 2018; Lever Taylor et al. 2014).
Interestingly, compassion meditations and psychoeducation around self-compassion are not routinely included in many MBPs in their standard format. In their paper defining the common ingredients of MBPs, Crane et al. (2016) specified compassion as one of the positive qualities that is promoted to enhance attentional, emotional and behavioural self-regulation. Reviews have highlighted how programmes such as MBSR and MBCT implicitly engender an attitude of compassion towards experience in the stance of the trainer and in the way participants are encouraged to relate to their experiences through inquiry (Feldman and Kuyken 2011). Kabat-Zinn also argued that MBSR brings about mindfulness via an attitude of acceptance, kindness, compassion, openness, patience, nonstriving, equanimity, curiosity and nonevaluation (Kabat-Zinn 1994, 1996). Therefore, it appears that many authors view self-compassion as being developed implicitly through attitudes cultivated in MBPs. Addressing compassion more broadly, Gilbert and Choden (2015) viewed mindfulness as a context through which compassion is achieved, necessary for both the motivation to engage with suffering and skill to alleviate it (Gilbert 2009). Thus, it may be that increasing mindfulness skills fosters greater self-compassion.
A small number of empirical studies have investigated self-compassion as a possible mechanism of change in MBPs. As part of a large randomised controlled trial (RCT) of MBCT for participants in remission from three or more major depressive episodes, Kuyken et al. (2010) found that self-compassion and mindfulness mediated the effect of treatment on depressive symptoms at the 15-month follow-up. Further, self-compassion moderated the treatment effect of uncoupling of cognitive reactivity and depressive symptoms. In a community sample, self-compassion mediated the relationship between mindfulness and wellbeing following MBSR (Evans et al. 2018). However, this pilot study did not demonstrate the temporal order of change and did not use a control group. A further quasi-experimental study investigating mediation of mindfulness and self-compassion on trait anxiety in students following an MBSR-based programme (Bergen-Cico and Cheon 2014) found that mindfulness, but not self-compassion, was a significant mediator of the effect of MBSR on anxiety. However, group assignment was based on elective course choice; therefore, the treatment group may have been differently motivated to complete the MBSR course and baseline measures were not reported. Despite the variation of analysis methods between these studies, Bergen-Cico and Cheon (2014) suggested that the lack of mediation effect found for self-compassion in their study may have been due to differences between clinical and nonclinical populations. It is also important to note that this study focused on anxiety rather than depression and could be a further reason for their findings.
Systematic reviews investigating the mechanisms through which MBPs such as MBSR and MBCT improve mental health and overall wellbeing (Alsubaie et al. 2017; Gu et al. 2015) concluded that further evidence would be needed to support the role of self-compassion as a mediating factor. At the time of these reviews, only one robust study of the mediating role of self-compassion had been conducted (Kuyken et al. 2010). This assessed depressive symptoms and relapse in a clinical sample who participated in MBCT; therefore, it is unclear if the findings in this study apply outside of samples in remission from chronic depression and for other MBPs. Despite the low number of methodologically robust studies examining self-compassion as a mediator of change in MBPs, other RCTs have included self-compassion as an outcome measure. Chiesa and Serretti (2009) reviewed the effect of MBSR on stress and other secondary outcomes in nonclinical populations and found one study showing an increase in self-compassion (Shapiro et al. 2005). Eberth and Sedlmeier (2012) reviewed and analysed MBSR and meditation programmes, assessing self-compassion as part of a broader factor of “self-concept”, finding a small to medium overall effect (r = 0.23). Since these reviews, a larger number of studies assessing broad mental health outcomes following MBPs in nonclinical populations have also measured self-compassion. One meta-analysis of compassion-based programmes on self-compassion has been conducted, finding a medium effect size (d = 0.7) (Kirby et al. 2017). However, this review included compassion-based programmes with limited mindfulness components and was not assessing MBPs with less compassion focus. Another meta-analysis of third-wave interventions (including MBPs) on self-compassion in clinical and sub-clinical populations found a medium effect size (g = 0.52) (Wilson et al. 2019), also showing no difference between explicit compassion programmes when compared with MBPs. However, this review did not include studies in nonclinical populations.
Despite the preceding assertions that MBPs foster increased self-compassion, there has to date been no synthesis of the effect of MBPs targeting broad mental health outcomes (anxiety, depression and stress) on self-compassion in nonclinical populations. Additionally, explicit compassion and loving-kindness meditations are on occasion incorporated into MBPs based on the standard MBSR format (e.g. Baer et al. 2012). It is unclear if the addition of these more compassion-specific components to MBPs increases self-compassion to a greater degree.
The current study aims to systematically review the effect of MBPs (including both brief online programmes as well as “standard” MBSR/MBCT protocols) on self-compassion, in RCTs addressing broad mental health outcomes (depression, anxiety and stress) in nonclinical populations, and to statistically synthesise these findings in a meta-analysis. The study will address three key research questions: (1) Compared to control conditions, what are the effects of MBPs on self-compassion in the nonclinical population? (2) Does the effect on self-compassion vary depending on whether the MBP includes additional compassion components? (3) Does change in self-compassion always co-occur with change in depression, anxiety and stress symptoms?
Method
Search Strategy
Titles and abstracts from three online databases (PsycINFO, PubMed and Web of Science) up to 26th January 2020 were systematically searched using the terms [(Mindful* OR MBCT OR MBSR OR medit* OR “compassionate mind” OR “compassion focused” OR CFT OR ACT OR “acceptance and commitment” OR DBT OR “dialectical behaviour therapy”) combined with (depres* OR anx* OR stress OR wellbeing OR “well-being” OR “well being” OR “mental health” OR “psychological health”) combined with (“self-compassion” OR “self compassion” OR compassion) combined with random*]. All abstracts identified were screened by the first author. Full texts from the screen were reviewed and assessed for eligibility. A subset (12 studies) of screened full texts were reviewed by a second reviewer, and any disagreements were resolved by discussion. Cohen’s kappa could not be calculated for inter-rater reliability; however, the two raters agreed on 11 studies with the exception of one inclusion where discussion was required.
The manual search was conducted by the first author who hand-searched the reference lists of all eligible studies at the full-text screening stage. If inclusion could not be determined via details in the published study, authors were contacted directly by the researcher for further information. Where studies were part of wider trials, or linked to other published articles, these were consulted when further information was required.
Inclusion and Exclusion Criteria
Studies were included for review according to the following criteria: (1) RCTs; (2) participants were aged 18 or over; (3) programme was mindfulness-based, which for this review was specified as a programme encouraging home practice for at least 2 weeks duration (as to encompass brief interventions but exclude “one-off” practices), and at least half the practices consisting of mindfulness meditation; (4) data included validated psychometric subjective measures of self-compassion pre- and post-programme; and (5) data included validated psychometric subjective measures of one or more of state depression, anxiety or stress. Exclusion criteria were as follows: (1) participants recruited on the basis of a diagnosable mental or physical health problem via either a clinical setting or meeting clinical threshold on standardized measures and (2) not published in the English language.
Data Extraction
Extraction of the following data was conducted: (1) participants, including number, method of recruitment, inclusion/exclusion criteria and other demographic characteristics; (2) intervention, including format (e.g. MBSR, MBCT, compassion-based), duration, amount of home practice encouraged and delivery method (e.g. group, self-help); (3) control group details; (4) programme adherence; (5) outcomes, including primary outcomes of interest and measures used; and (6) statistical findings regarding self-compassion and measures of depression, anxiety or stress were extracted. For the SCS, effect sizes for total scores were calculated for inclusion in the meta-analysis. Correlations between change in self-compassion and distress post-MBP were also extracted. Subscale scores were extracted if available. Authors were contacted for required data if not reported directly in the text (this was not possible with unpublished studies).
Statistical Analysis
A meta-analysis was conducted for self-compassion outcomes, using the statistical software program Review Manager version 5.3 (The Cochrane Collaboration 2014). Effect sizes for total self-compassion scores were calculated using Hedges g (pre-post change for the MBP group minus the pre-post change for the control group, divided by the pre-programme standard deviation multiplied by Hedges correction factor (Carlson and Schmidt 1999; Hedges 1981; Morris 2008)). This effect size has been found to provide a better estimate in terms of bias, precision, and heterogeneity of variance, and takes into account baseline differences between groups (Morris 2008). Effect sizes were interpreted as 0.2 = small, 0.5 = medium and 0.8 = large (Cohen 1992). Effect sizes for studies with a design that randomized participants to three groups were calculated by combining mean, standard deviation and sample size for either MBP (where two MBP conditions were delivered) or control groups (where two different control conditions were used) to provide a weighted mean and estimated standard deviation. This is preferable to entering multiple comparisons for a single study, to avoid unit-of-analysis error resulting from unaddressed correlations between the estimated programme effects from multiple comparisons (The Cochrane Collaboration 2011).
A random-effects model was selected to examine the difference in pre-post self-compassion scores between the MBP group and control group in each study, resulting in an overall effect size based on weighted averages of the effect sizes. This model was chosen over a fixed-effects model due to the different populations sampled in the review and the degree of heterogeneity of MBPs included, which fits with the model’s assumptions that observed estimates of effect size may vary systematically across studies (Borenstein et al. 2009; Field and Gillett 2010). A random-effects model also allows for findings to be generalized beyond the subset of included studies. A forest plot was created for a visual representation of effect sizes for each study and allowed for inspection of outliers.
Heterogeneity of effect sizes was assessed using Cochran’s Q statistic (χ2) to investigate whether there was significant variation between studies, and the I2 index to measure the magnitude of heterogeneity. A significant Q statistic (p < 0.05) indicates that the variance of the results may be due to varying effect sizes, resulting from possible sampling or methodological variance across the included studies. I2 is interpreted as the degree of variability among effect sizes across studies due to heterogeneity rather than chance/sampling error, reported as a percentage. This can be interpreted as 0% indicates homogeneity; 25% indicates small levels of heterogeneity; 50% is medium; and 75% is large (Huedo-Medina et al. 2006).
Post hoc subgroup analyses were performed, to investigate potential sources of heterogeneity. As there were no pre-specified hypotheses regarding potential moderating variables that would impact on the effect on self-compassion, these analyses were considered exploratory. The moderating effects of explicit compassion components (MBP with no added compassion/kindness meditations or focus vs. MBP with additional compassion/kindness components), psychological distress as a participation inclusion criterion (minimum distress threshold measure vs. no threshold) and type of control group (wait-list vs. active control) were investigated. This was assessed by categorizing the studies according to the proposed moderator variable (or if applicable, categorizing experimental groups within a study) and comparing their separately pooled effect sizes, using a between-group heterogeneity statistic Qbetween (Hedges and Olkin 1985). A significant moderator effect is indicated by a statistically significant Qbetween.
A meta-regression was not indicated due to the number of studies that were available for analysis (The Cochrane Collaboration 2011); however, effect sizes for the association between self-compassion and distress were calculated using Fisher’s Z transformation for correlation coefficient r to avoid underestimation of effect (Borenstein et al. 2009) and weighted according to sample size with standard error 1/ √ (N − 3) and entered into a random-effects model. This was then back-transformed to r values for ease of reporting. Effect sizes were interpreted as small = 0.1, medium = 0.3 and large = 0.5 (Cohen 1992).
Publication bias was assessed by creating a funnel plot of effect sizes against standard error and visually inspecting the plot for signs of asymmetry. Asymmetry could be due to potential bias due to the under-reporting of negative or null results. Orwin’s (1983) failsafe N was calculated to determine the number of studies with null results (set at d = 0) needed to reduce the effect size to a negligible level (set at d = 0.1). This statistic was chosen due to the ability to select a nonzero effect size for the missing studies. The trim and fill method (Duval and Tweedie 2000) was considered to impute missing studies and compute an adjusted mean effect size taking missing studies into account; however, this method was not used due to the bias introduced by the heterogeneity found in the analysed studies, which has been found to affect the validity of this method (Peters et al. 2007; Terrin et al. 2003). This analysis strategy was used for total SCS scores both immediately post-programme and at follow-up in separate models to avoid unit-of-analysis error (The Cochrane Collaboration 2011). It was also hoped to synthesise effect sizes for SCS subscales; however, calculation and reporting of scores in the negative subscales (self-judgement, isolation and overidentification) varied between studies (using reversed items vs. nonreversed) and precluded any estimate of overall effect across the studies.
Methodological Quality Assessment
Studies meeting the criteria for review were assessed for methodological quality using an adapted version of the Quality Assessment Tool for Quantitative Studies (National Collaborating Centre for Methods and Tools 2008). The use of this checklist was modified for the purposes of the current study by (1) omitting an overall score, given the questions around the suitability of their application (Centre for Reviews and Dissemination 2009); (2) altering the weighting of scores in the Selection Bias component, where self-referral rating was changed from “weak” to “moderate”, as the nature of voluntary psychological programmes such as MBPs is more likely to produce studies that recruit via self-referral; (3) altering the Study Design component to include power calculation and removing use of a RCT design as a criterion for “strong”, as only RCTS were being assessed in the current review; (4) focusing on the outcomes of interest for the current review when assessing for quality of data collection methods; and (5) developing ratings for the Intervention Integrity and Analysis components, with a particular focus on the analysis of self-compassion outcomes rather than the study’s primary outcomes. This resulted in a set of 16 questions comprising eight components: (Selection Bias, Design, Confounders, Blinding, Data Collection Methods, Withdrawals and Dropouts, Intervention Integrity, Analysis) with each of these components receiving a “strong”, “moderate” or “weak” rating. No studies were removed based on quality assessment, as this can lead to overexclusion, therefore potentially limiting the validity of the results (Meline 2006).
Results
Study Inclusion
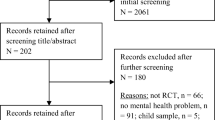
Figure 1 illustrates the process of study selection according to PRISMA guidelines (Moher et al. 2009). The literature search yielded 849 articles, of which 307 were duplicates. After removal of duplicates, 598 titles and abstracts were screened and 141 articles were reviewed based on the full text. This resulted in the final selection of 26 studies, published between the years 2005 and 2020, conducted in the USA (n = 12), UK (n = 4), Spain (n = 2), Australia (n = 1), Belgium (n = 1), Canada (n = 1), Hong Kong (n = 1), the Netherlands (n = 1), Norway (n = 1), Romania (n = 1) and Sweden (n = 1). A summary of study characteristics can be found in Table 1.

PRISMA flowchart for selection process of studies in systematic review and meta-analysis
Sample Characteristics
All but one (which used random sampling) of the studies recruited using opportunity sampling, with 13 recruiting from universities and 13 recruiting from the community, reflecting an overrepresentation of the student population. A number of the studies sampling from the community targeted specific groups from a variety of sources, such as mothers, carers and specific workplaces. While most of the studies had no specific inclusion criteria in terms of psychological distress, seven of the studies only recruited participants with a minimum score on a measure of interest (e.g. neuroticism, perfectionism, stress). The total number of participants included across the studies was 2025, with sample sizes ranging from 13 to 83 for an MBP group and between 13 and 100 for a control group, reflecting a large range of sample sizes with many that were pilot studies and/or underpowered. A large range of ages with predominantly female participants comprised the studies’ participant sample; weighted mean age was 35.2 years across the 22 studies that reported age and mean percentage female was 78% (range 46–100%).
Study Design
Of the included RCTs, 11 were labelled as pilot studies; these studies represented the smallest sample sizes; however, some of the RCTs were also underpowered. In 23 of the studies, participants were randomized into one of two groups (MBP vs control) and in three studies, a three-group randomized design was used (either two different MBPs vs control, or MBP vs active control and wait-list). The majority (21) of the included studies used wait-list control groups; however, five studies used other evidence-based psychological programmes for the target problem for their active control condition (CBT-based self-help, psychoeducational self-help, relaxation response programme, progressive muscle relaxation) and another study used an activity matched for duration and relaxing auditory content (classical music listening). Self-compassion was not a sole primary outcome in any of the studies, but was listed alongside other measures of mindfulness and psychological symptoms as primary outcomes in seven of the studies. One study only analysed self-compassion as a mediating factor but also reported pre-post-programme scores. As well as measuring self-compassion (and other variables, including depression, anxiety or stress) at baseline and post-programme, nine studies took follow-up measures (between 8 weeks and 1 year post-programme). The current sample of studies therefore favoured wait-list control in their RCT design and were primarily interested in indices of distress alongside self-compassion following MBPs, rather than assessing the association between the two.
Measures of Interest
All of the included studies used the SCS in either the long (n = 15) or short (n = 11) form to measure self-compassion. The majority of studies (24) used total score (either average or summed) as an index of self-compassion, and one study used only the positive subscales (Self-Kindness, Common Humanity and Mindfulness) of the SCS as a composite score. Another study presented the subscales of the SCS (which were also detailed in seven other studies) without reporting a total score. In terms of general measures of psychological distress, stress was measured in the majority of the studies (21), while depression was investigated in 14 and anxiety in 13; nine measured all three.
Type of MBP
The majority (23) of the included studies described the MBP as MBSR- or MBCT-based, the remaining three studies used a 2-week (Gu et al. 2018) or 8-week (Huberty et al. 2019) self-help MBP or “brief integrated practice” group-delivered mindfulness programme (Arredondo et al. 2017). Of these studies, 11 described the MBP used as MBSR/MBCT adapted for their target population and eight incorporated additional kindness and compassion components. Group format was the dominant delivery method of MBP across the sample of studies (19 delivered weekly sessions, one study delivered sessions twice weekly and one study had twice weekly sessions in the first 2 weeks followed by weekly). For the group-based programmes, session duration ranged from 75 to 120 min, and total number of sessions ranged from three to nine (median number of sessions = 8). Although the majority of studies described their MBP as adapted MBCT/MBSR, only a small number incorporated a retreat into their programme (one half day, two full days and one with two full days). Total contact time ranged from 4.5 to 16 h (median = 16 h). Of the 21 group-delivered programmes, 15 reported facilitators with specific training in delivering MBPs (one who was a peer facilitator); the remaining studies described facilitators as being trained in CBT and had experience of mindfulness (n = 1), staff from a university counselling service (n = 2), licenced psychologists (n = 1) and one of the authors of the paper (n = 1), or did not report the expertise or training of facilitators (n = 2). A smaller number of studies investigated MBPs delivered through self-help (three with access to a website, one via a mobile app and one through a book), all of which provided extra information (either via psychoeducation webpages or book chapters) and encouraged daily home practice. Duration of self-help programmes ranged from 2 to 8 weeks. Home practice was reported as part of the MBP in 23 of the included studies, with 16 detailing frequency and duration of recommended formal practice. All but one of these studies stipulated daily practice with minimum durations ranging from 10 to 45 min (median = 20 min). MBPs based around the MBSR or MBCT group-delivered format with required home practice dominate the current sample of studies, with many adopting content for their selected sample. However, use of the retreat day was limited and not all studies reported using trained facilitators to deliver the MBP.
Intervention Adherence
Twenty-two studies reported adherence to the MBPs (and active control condition if applicable) delivered, and definitions of adherence were wide ranging: from attending at least half of the sessions (or completing half of the self-help content) to attending seven out of eight sessions. These studies reported adherence rates of 48–100%, median = 80%. Although home practice was incorporated into the majority of programmes used in the studies, measures of duration or frequency of home practice were not always reported. When detailed, self-report of home practice showed a wide range across the studies; 14 studies reported average duration (mean or median) of home practice ranging from 15 to 120 min weekly and frequency between 2 and 7 days per week. Only two studies (Armstrong and Rimes 2016; Potharst et al. 2019) statistically investigated the link between adherence and self-compassion, both finding a significant association between either amount of home practice or number of sessions attended with SCS scores.
Self-Compassion and Psychological Distress
We were also interested in the consistency of significant change in self-compassion and psychological distress (depression, anxiety, stress). Of the 19 studies that found a statistically significant post-programme increase in self-compassion, two studies found no significant change in depression or anxiety (stress was not measured in either of these studies) and one study found no significant change in stress (however, the same study found significant improvements in depression and anxiety). Of the six studies that found no significant difference in self-compassion pre- and post-programme, two found significant change in one of depression, anxiety or stress. Four studies (Benn et al. 2012; Gu et al. 2018; Shapiro et al. 2005; Ștefan et al. 2018) formally assessed self-compassion as a mediating factor in psychological distress (indexed as stress in all of the studies). Three of these studies found a significant mediating effect of self-compassion on stress; however, one study did not report such an effect. Only two of these studies examined change in self-compassion that temporally preceded change in stress by using either mid-programme self-compassion (Gu et al. 2018) or post-programme self-compassion with follow-up stress (Benn et al. 2012). Overall, the majority of studies found increases in both self-compassion and distress; however, this was not a consistent picture. When investigated, there was inconsistent support for self-compassion as a mediating factor in change for MBPs, with variation in how mediation was assessed.
Meta-Analysis Findings
Four studies (Arredondo et al. 2017; Hwang et al. 2019; O’Donnell 2017; Shapiro et al. 2005) did not report sufficient data for inclusion in the meta-analysis (pre- and post-programme mean, pre-programme standard deviation and sample size were all required); therefore, effect sizes from 22 studies were calculated. Three studies required calculation to combine MBP groups (Bayot et al. 2020; Mistretta et al. 2018) and control groups (Gu et al. 2018). The forest plot (Fig. 2) shows effect sizes (Hedges g for MBP vs control pre-post difference in self-compassion scores) for each study. The analysis revealed a medium effect size on self-compassion (g = 0.60, 95% CI = 0.41 to 0.80, p < 0.001). Tests for heterogeneity revealed a significant amount of medium to large heterogeneity (Q(21) = 65.97, p < 0.001, I2 = 68%).

Forest plot for post-programme self-compassion. Note that mean here refers to mean difference between pre- and post-programme scores, and SD represents pre-programme standard deviation. (a)—weighted mean and SD combining two MBP groups, (b)—weighted mean and SD combining two control groups. *Estimated marginal means reported, **ITT means reported
Given the significant amount of medium to large heterogeneity found, post-hoc assessment of potential moderators for self-compassion was conducted. Comparing “standard” MBPs (n = 17, g = 0.53, 95% CI 0.30 to 0.77) with MBPs incorporating additional compassion/kindness components (n = 6, g = 0.78, 95% CI 0.58 to 0.98) revealed no significant difference in self-compassion between the two groups (Qbetween(1) = 2.46, p = 0.12). For this subgroup analysis only, the data from the standard mindfulness and compassion-added groups in Bayot et al.’s (2020) study were entered separately. Comparing studies that used a minimum threshold for psychological distress as a participation inclusion criterion (n = 6, g = 0.76, 95% CI 0.21 to 1.31) with studies that used no distress threshold (n = 16, g = 0.55, 95% CI 0.37 to 0.74), no significant difference was found (Qbetween(1) = 0.50, p = 0.48). Comparing studies that used an active control condition (n = 5, g = 0.61, 95% CI 0.07 to 1.14) to those that used a wait-list control condition (n = 17, g = 0.61, 95% CI 0.41 to 0.79), no significant difference was found (Qbetween(1) < 0.01, p = 0.97). For this subgroup comparison only, the data from Gu et al.’s (2018) study were separated into the active and the wait-list control groups.
Visual inspection of the funnel plot (Fig. 3) indicated possible asymmetry, with larger studies showing a tendency towards a lower effect size and a lack of smaller studies showing a lower effect. However, Orwin’s failsafe N revealed that a total of 110 studies with a null effect size would need to be located to reduce the mean effect size to below 0.1. It is unlikely that such a number of studies with a null result exist, suggesting that the mean effect size found would be robust to publication bias. Due to heterogeneity, trim and fill analysis was not performed.

Funnel plot of effect sizes by standard error for post-programme self-compassion
Seven studies provided sufficient follow-up data for inclusion in the meta-analysis. Effect sizes are shown in the forest plot in Fig. 4. The analysis revealed a medium effect size (g = 0.53, 95% CI = 0.21 to 0.85, p = 0.001). Tests for heterogeneity revealed a significant amount of medium heterogeneity (Q(5) = 17.83, p = 0.007, I2 = 66%). The small number of studies made interpretation of the funnel plot (Fig. 5) difficult; however, it appeared to have reasonable symmetry. Orwin’s failsafe N found a total of 30 studies with a null effect size would need to be located to reduce the mean effect size to below 0.1.

Forest plot for follow-up self-compassion. Note that mean here refers to mean difference between pre-programme and follow-up scores, and SD represents pre-programme standard deviation. *Estimated marginal means reported

Funnel plot of effect sizes by standard error for follow-up self-compassion
Six studies provided correlations between change in self-compassion and stress, two studies reported correlations for change in self-compassion and depression and one study for anxiety. Only the correlations with stress were entered into a meta-analysis. Correlation coefficient r ranged from − 0.61 to − 0.41. The effect size found was not significant (r = − 0.52, CI − 0.99 to 0.88, p = 0.57).
Methodological Quality Assessment
Ratings for each of the categories for all studies can be found in Table 2. Of the 26 studies included, four were rated as weak on none of the categories, five in one category, 12 in two categories, four in three categories and one in four categories. In terms of Selection Bias, the studies that were rated as weak were due to a low percentage of recruited participants taking up the study (n = 8), insufficient information or evidence of unrepresentative sampling (n = 3) or both (n = 1). For Study Design, only one study was rated as weak, due to inappropriate randomisation introducing possible bias (allocation to wait-list or programme was based on enrolment in the programme in either the autumn or the summer). Five studies did not measure potential confounders, and three did not control for the confounding factors identified, resulting in a weak rating for the Confounders category. All studies scored either moderate or strong for Blinding and Data Collection Methods, reflecting the use of sufficiently valid and reliable self-report measures. Two studies were rated as weak for Withdrawal and Dropouts, due to reporting 40% or more dropout. For Intervention Integrity, studies were rated weak due to lack of description of programme integrity (n = 4) or less than 60% adherence to the programme (n = 5). The rating of the category was complicated by the variation of criteria for programme adherence between the studies, where described the authors’ own criteria were used. Thirteen studies lacked sufficient power to detect possible effects and were therefore rated weak for the Analysis category. Of these, six studies were described as pilot studies.
Discussion
The aim of the review was to examine the effect of MBPs on self-compassion in the nonclinical population, examine whether this effect varies if the MBP includes explicit compassion components and determine whether changes in self-compassion accompany changes in depression, anxiety and stress. The meta-analysis found a significant medium effect of MBPs on pre- to post-programme change in self-compassion when compared to controls, and at follow-up. However, both analyses revealed significant heterogeneity to a medium to large degree, indicating that this effect was not consistent across studies. Post hoc subgroup analyses attempted to locate possible moderating effects that could generate further questions around variance in effect size across the studies; however, no significant differences between groups were found based on MBP content (solely MBSR focused vs. additional explicit compassion components), recruitment strategy (minimum psychological symptom threshold vs no threshold) or type of control group used (active vs wait-list). This heterogeneity complicated interpretation of tests for publication bias; however, it appeared that the effect size found for post-programme self-compassion was not heavily influenced by publication bias.
Meta-analysis of association between change in self-compassion and distress post-MBP was limited by the small number of studies with available data, and no significant effect was found between self-compassion and stress. This does not, however, provide strong evidence for a lack of effect; due to the small sample sizes used, there is a strong likelihood that a significant effect may have been missed (The Cochrane Collaboration 2011). Examination of the associations between self-compassion and both depression and anxiety was precluded by lack of available data. Review of statistical significance of self-compassion alongside depression, anxiety and stress showed mixed results, with the majority of studies showing improvement in both self-compassion and a measure of psychological distress. However, this was not a consistent pattern, with two studies showing an increase in self-compassion without a significant decrease in depression or anxiety, and two studies exhibiting the opposite pattern. Three of the four studies that investigated mediation found a significant mediating effect of self-compassion on change in stress levels. No pattern in terms of sample, sample size, outcome measure or programme (duration, format) could be found to account for the heterogeneity in these study outcomes. However, it may be that the relationship between self-compassion and stress in MBPs is more robust, as the two studies showing an increase in self-compassion without a concomitant reduction in distress did not measure stress. These findings also need to be interpreted with caution, as “vote counting” (reviewing only statistical significance) does not take study sample size into account and does not review effect size (Centre for Reviews and Dissemination 2009).
This review indicates that MBPs in nonclinical groups can increase self-compassion; however, there is variability in the extent to which this is the case, and as yet unaccounted moderating factors behind this. One area that has been recommended for further investigation is facilitator effects (Van Dam et al. 2018), which was not explored in the current meta-analysis. Facilitators may focus on self-compassion to difference degrees, or level of facilitator training may influence any or all of self-compassion, depression, anxiety or stress. There may also be further individual differences within study samples that could influence results.
While this review synthesised the effect of MBPs on self-compassion in nonclinical populations, meta-analyses of compassion-based programmes found a similar medium effect size for self-compassion in studies assessing both clinical (Kirby et al. 2017; Wilson et al. 2019) and sub-clinical samples (Kirby et al. 2017). Although difficult to definitively conclude due to the overlap in content between MBPs and compassion-based programmes, this indicates that MBPs and compassion-based programmes may both increase self-compassion to a similar degree. A moderating effect when comparing MBPs with or without explicit compassion components in the current review also did not reach significance, adding further support to this suggestion. However, there was a trend towards compassion-added programmes showing greater increases in self-compassion and these null results were from an analysis with small sample sizes. Therefore, this analysis was underpowered and should be interpreted with caution, as significant effects may have been missed. Further investigation with larger sample sizes is required; however, this could indicate that self-compassion increases following MBSR/MBCT-based programmes as well as those that target compassion more explicitly. Also of interest are the three studies that implemented self-help MBPs, all of which showed an increase in self-compassion, indicating that facilitators or post-exercise inquiry may not be necessary to effect change in self-compassion (c.f. Feldman and Kuyken 2011; Gilpin 2008). Although further replication would be required, one of these studies did not add any explicit compassion/kindness meditations or psychoeducation. This provides further support for the idea that meditation instructions themselves implicitly engender self-compassion (Hölzel et al. 2011).
The findings of this review also have theoretical implications. The results showing that MBPs have a significant impact on self-compassion are consistent with the assertion that compassion is encompassed in effective mindfulness programmes (Crane et al. 2016; Feldman and Kuyken 2011; Kabat-Zinn 1994, 1996), and go some way to supporting theories and findings suggesting that self-compassion may be a mediator of change in MBPs (Allen et al. 2009; Hölzel et al. 2011; Kuyken et al. 2010). Three of the studies reviewed also demonstrated a mediation effect statistically (Gu et al. 2018; Shapiro et al. 2005; Ștefan et al. 2018). Previously, this had been an assertion based on theoretical reports and a limited number of studies (Alsubaie et al. 2017; Bergen-Cico and Cheon 2014; Evans et al. 2018; Gu et al. 2015). This review assessed the overall effect in a larger number of RCT studies measuring self-compassion. Although the current review findings cannot speak to the temporal ordering of change in both self-compassion and psychological distress, nor address mediation directly, the significant overall effect at post-programme and follow-up provides further support for its potential role as a mediating factor.
Although nine of the included studies measured at least three timepoints, only four studies (Benn et al. 2012; Gu et al. 2018; Shapiro et al. 2005; Ștefan et al. 2018) directly assessed for mediation, with varying results. Further, only two assessed the temporal precedence of self-compassion change. Albeit a far less statistically robust method of assessing effects, comparing significant change in self-compassion versus psychological distress (depression, anxiety or stress) within studies also showed a complicated picture. Some studies reported significant improvement in psychological distress without a significant change in self-compassion and vice versa. These results need to be interpreted with caution as studies were not given different weights based on sample size; however, the conclusions that can be drawn from the meta-analysis of self-compassion and distress correlation (stress) are also limited due to the small sample size.
Strengths and Limitations of the Studies
In reviewing the methodological quality of the studies, a number of strengths and weaknesses were identified. Most studies relied on opportunity sampling, introducing potential bias such as recruiting participants who had a positive attitude towards MBPs. However, any MBP in a nonresearch setting would also be open to invitation, therefore likely reflecting uptake in the real world. Females were overrepresented in most of the samples, therefore making it difficult to generalise the findings to men. As the studies were RCTs, there were low numbers of confounding factors, reducing the risk of selection bias. Most of the studies used wait-list control groups. While these are particularly helpful when testing a programme in a new population, as was the case in a number of the included studies, it remains unclear whether increased self-compassion was a result of MBPs specifically or other therapeutic components (e.g. group membership, psychoeducation). Although exploratory, one counter to this could be the lack of significant difference in effect size when comparing studies with a wait-list or active control. In terms of blinding, researchers were often not blinded to the condition which potentially introduced investigator effects in procedures such as communication with participants; however, the use of self-report measures minimises the effect when compared with researcher-conducted interviews or observational ratings. Commonly, participants were blinded to the hypotheses of the study; however, the nature of the studies precluded being blinded to condition, leading to possible social desirability bias in self-report responses. Most of the studies reported reasonable adherence to the programmes, suggesting that the MBPs used were feasible and acceptable to the participants; however, few investigated any link between adherence and self-compassion. One particular weakness identified in the studies was a lack of power due to small sample sizes that may have missed potential effects and analyses that did not take into account dropouts, which may have exaggerated the effects of MBPs. However, a number of underpowered studies were pilot studies. Both of these issues may have contributed to the heterogeneity found in the study sample.
All the studies used the SCS, which is one of the only validated and most commonly used measure of self-compassion (Neff 2003b, however see Gilbert et al. 2017). There have been a number of issues identified with this measure; for example, Williams et al. (2014) re-assessed the factor structure with meditators, nonmeditators and those in remission from repeat episodes of depression and could not find evidence for an overarching single factor of self-compassion, suggesting that reporting the six factors is preferable. Another study has questioned the validity of combining the positive (Self-Kindness, Mindfulness, Common Humanity) and negative (Overidentification, Isolation, Self-Judgement) aspects of the SCS (Costa et al. 2016). Neff (2016) suggested that either the single (particularly in the case of SCS-SF) or the six-factor items should be reported; however, this does not account for the issue that a person could score high on both negative and positive elements and receive the same score (Gilbert et al. 2017). Further, the overlap of mindfulness and self-compassion in the SCS may complicate the findings, as noted by MacBeth and Gumley (2012). This leaves unclear whether an increase in self-compassion following MBPs is driven by an increase in the mindfulness subscale much more than the other factors. Considering these issues, it may be beneficial for all future studies to report the six subscales of the SCS, or for a more psychometrically robust measure of self-compassion to be developed (Williams et al. 2014; Gilbert et al. 2017).
Limitations and Future Research Directions
This review contributes further to evidence regarding the influence of MBPs on self-compassion and was able to produce a quantitative synthesis that summarised effect sizes across studies. However, a relatively small sample size for the meta-analysis precluded further investigation of the heterogeneity of effects found through methods such as meta-regression. Further, all of the post hoc subgroup analyses consisted of unbalanced small groups and were consequently underpowered; therefore, clear conclusions regarding the lack of significant difference between potential moderating factors are not possible. Meta-analysis of self-compassion and distress associations was similarly affected by very low sample sizes. Considering the inclusion criteria, there was no exclusion based on sample size or pilot study status. This may have resulted in inclusion of studies with limited power to detect effects; however, a number of the pilot studies included were sufficiently powered. Broader inclusion criteria regarding format, content and length of programme may have enabled further investigation of more diverse programmes. For example, programmes that draw on mindfulness but may have another focus (e.g. Acceptance and Commitment Therapy, Compassionate Mind Training), or single-dose meditations may provide further information about how mindfulness influences self-compassion. Confining results to studies that also measured state depression, anxiety or stress may also have restricted the number of studies that measured self-compassion in different contexts (particularly those that targeted community samples and measured psychological processes rather than symptoms). The focus on RCTs facilitated statistical analysis of overall effect and reduced the risk of bias from noncontrolled study designs; however, this excluded a number of studies that investigated self-compassion and its change over time in MBPs. The findings from this review revealed a number of potentially beneficial avenues for future research. We propose the following specific recommendations:
Studies assessing self-compassion (and other potential mechanistic outcomes) would benefit from further investigation into the link between self-compassion and psychological wellbeing following MBPs. This could take the form of reporting correlations or partial correlations between self-compassion and measures of psychological distress/wellbeing, or preferably taking follow-up or mid-intervention measures and conducting mediation analyses. This would enable future meta-regressions of such results.
While the current review found that MBPs with additional compassion components did not reach statistical significance in improving self-compassion, the low number of studies preclude firm conclusions. Further studies that directly compare MBPs with or without explicit compassion material are needed.
More studies should determine which “ingredients” of MBPs influence difference outcomes. Given theoretical suggestions about how self-compassion comes about during MBP participation (Feldman and Kuyken 2011; Kabat-Zinn 1994, 1996), particular attention should be paid to the attitude of the facilitator, perhaps utilising independent raters to determine compassionate responses during group sessions. Also of interest would be to compare programmes that do or do not contain inquiry, for example, programmes that are facilitated as opposed to other formats (e.g. self-help book, Internet, mobile app). Content of meditations (e.g. attention versus attitude) could also be examined and compared with self-compassion and other outcomes in mind.
Other measures of self-compassion should be investigated. All of the studies in the current review used versions of the SCS; however, given the debate around the conceptualisation of self-compassion, it would be useful to explore more recent tools, such as the Compassion Engagement and Action Scale (Gilbert et al. 2017). Reporting subscales of the SCS would also enable researchers to potentially tease out results based on varying conceptualisations of self-compassion (e.g. positive and negative subscales).
Given the wide range of programme adherence and home practice reported across the studies in this review, future studies may benefit from assessing how this relates to self-compassion (and other outcomes). For example, is there a minimum amount of practice that influences outcomes and is any relationship between these factors linear? Further, a more consistent method of reporting programme adherence in MBPs would be advantageous: for example, a score that incorporates a proportion of participants attending a sufficient number of group sessions and amount of home practice. Alternatively, an adherence score could be calculated for individual participants and either covaried for in analyses or testing for associations between adherence and outcome.
Considering the minority of studies using self-help MBPs that measured self-compassion, further work assessing this method of delivery is recommended, particularly given the emerging evidence of its efficacy (Blanck et al. 2018; Cavanagh et al. 2014; Spijkerman et al. 2016) and accessibility of mindfulness via books, websites and apps (e.g. Shore et al. 2018). This would enable future moderator analyses to compare self-help MBPs with more traditional group formats.
Use of active control conditions is recommended. Given the inconclusive moderator analysis in the current review, it is of interest to determine which other interventions do or do not increase self-compassion, for example CBT or relaxation programmes. This is of particular interest given the theoretical links between mindfulness and compassion.
Studies with more rigorous analytic strategies are needed. This would involve conducting power analyses and adequately accounting for dropout when determining sample size, taking baseline measures into account when analysing post-programme change and use of ITT analysis.
Self-compassion has been measured in a number of studies that were predominantly investigating effects of MBPs on psychological distress in nonclinical populations. A meta-analysis suggested that MBPs significantly improve self-compassion. However, this was not a consistent effect across all studies and reasons for this heterogeneity require further investigation. Further work assessing self-compassion as a mediating factor of change in psychological distress following MBPs would benefit theory and practice of MBPs.
References
Allen, M., Bromley, A., Kuyken, W., & Sonnenberg, S. J. (2009). Participants’ experiences of mindfulness-based cognitive therapy: It changed me in just about every way possible. Behavioural and Cognitive Psychotherapy, 37(4), 413–430. https://doi.org/10.1017/S135246580999004X.
Alsubaie, M., Abbott, R., Dunn, B., Dickens, C., Keil, T. F., Henley, W., & Kuyken, W. (2017). Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: a systematic review. Clinical Psychology Review, 55, 74–91. https://doi.org/10.1016/J.CPR.2017.04.008.
Armstrong, L., & Rimes, K. A. (2016). Mindfulness-based cognitive therapy for neuroticism (stress vulnerability): a pilot randomized study. Behavior Therapy, 47(3), 287–298. https://doi.org/10.1016/j.beth.2015.12.005.
Arredondo, M., Sabate, M., Valveny, N., Langa, M., Dosantos, R., Moreno, J., & Botella, L. (2017). A mindfulness training program based on brief practices (M-PBI) to reduce stress in the workplace: a randomised controlled pilot study. International Journal of Occupational and Environmental Health, 23(1), 40–51. https://doi.org/10.1080/10773525.2017.1386607.
Baer, R. A., Lykins, E. L. B., & Peters, J. R. (2012). Mindfulness and self-compassion as predictors of psychological wellbeing in long-term meditators and matched nonmeditators. Journal of Positive Psychology, 7(3), 230–238. https://doi.org/10.1080/17439760.2012.674548.
Bayot, M., Vermeulen, N., Kever, A., & Mikolajczak, M. (2020). Mindfulness and empathy: differential effects of explicit and implicit Buddhist teachings. Mindfulness, 11, 5–17. https://doi.org/10.1007/s12671-018-0966-4.
Benn, R., Akiva, T., Arel, S., & Roeser, R. W. (2012). Mindfulness training effects for parents and educators of children with special needs. Developmental Psychology, 48(5), 1476–1487. https://doi.org/10.1037/a0027537.
Bergen-Cico, D., & Cheon, S. (2014). The mediating effects of mindfulness and self-compassion on trait anxiety. Mindfulness, 5, 505–519. https://doi.org/10.1007/s12671-013-0205-y.
Blanck, P., Perleth, S., Heidenreich, T., Kröger, P., Ditzen, B., Bents, H., & Mander, J. (2018). Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: systematic review and meta-analysis. Behaviour Research and Therapy, 102, 25–35. https://doi.org/10.1016/j.brat.2017.12.002.
Borenstein, M., Hedges, L., Higgins, J., & Rothstein, H. (2009). Introduction to meta-analysis. John Wiley & Sons.
Bowen, S., Witkiewitz, K., Clifasefi, S. L., Grow, J., Chawla, N., Hsu, S. H., & Carroll, H. A. (2014). Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention, and treatment as usual for substance use disorders: a randomized clinical trial. JAMA Psychiatry, 71, 547–556. https://doi.org/10.1001/jamapsychiatry.2013.4546.Relative.
Carlson, K. D., & Schmidt, F. L. (1999). Impact of experimental design on effect size: findings from the research literature on training. Journal of Applied Psychology, 84, 851–862.
Cavanagh, K., Strauss, C., Cicconi, F., Griffiths, N., Wyper, A., & Jones, F. (2013). A randomised controlled trial of a brief online mindfulness-based intervention. Behaviour Research and Therapy, 51(9), 573–578. https://doi.org/10.1016/j.brat.2013.06.003.
Cavanagh, K., Strauss, C., Forder, L., & Jones, F. (2014). Can mindfulness and acceptance be learnt by self-help?: a systematic review and meta-analysis of mindfulness and acceptance-based self-help interventions. Clinical Psychology Review, 34(2), 118–129. https://doi.org/10.1016/j.cpr.2014.01.001.
Centre for Research and Dissemintation. (2009). Systematic reviews: CRD’s guidance for undertaking reviews in health care. York, UK: University of York.
Chadwick, P. (2006). Person-based cognitive therapy for distressing psychosis. Wiley.
Chiesa, A., & Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. Journal of Alternative and Complementary Medicine, 15(5), 593–600. https://doi.org/10.1089/acm.2008.0495.
Cohen, J. (1992). Quantitative methods in psychology. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037/0033-2909.112.1.155.
Costa, J., & Pinto-gouveia, J. (2011). Acceptance of pain, self-compassion and psychopathology: using the chronic pain acceptance questionnaire to identify patients’ subgroups. Clinical Psychology and Psychotherapy, 18, 292–302. https://doi.org/10.1002/cpp.718.
Costa, J., Marôco, J., Pinto-Gouveia, J., Ferreira, C., & Castilho, P. (2016). Validation of the psychometric properties of the self-compassion scale. Testing the factorial validity and factorial invariance of the measure among borderline personality disorder, anxiety disorder, eating disorder and general populations. Clinical Psychology and Psychotherapy, 23(5), 460–468. https://doi.org/10.1002/cpp.1974.
Crane, R. S., Brewer, J., Feldman, C., Kabat-Zinn, J., Santorelli, S., Williams, J. M. G., & Kuyken, W. (2016). What defines mindfulness-based programs? The warp and the weft. Psychological Medicine, 47, 990–999. https://doi.org/10.1017/S0033291716003317.
Danilewitz, M., Bradwejn, J., & Koszycki, D. (2016). A pilot feasibility study of a peer-led mindfulness program for medical students. Canadian Medical Education Journal, 7(1), e31–e37. https://doi.org/10.36834/CMEJ.36643.
Dundas, I., Binder, P., Hansen, T. G. B., & Stige, S. H. (2017). Does a short self-compassion intervention for students increase healthy self-regulation? A randomized control trial. Scandinavian Journal of Psychology, 58, 443–450. https://doi.org/10.1111/sjop.12385.
Duval, S., & Tweedie, R. (2000). Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56, 455–463.
Dvořáková, K., Kishida, M., Li, J., Elavsky, S., Broderick, P. C., Agrusti, M. R., & Greenberg, M. T. (2017). Promoting healthy transition to college through mindfulness training with first-year college students: pilot randomized controlled trial. Journal of American College Health, 65(4), 259–267. https://doi.org/10.1080/07448481.2017.1278605.
Eberth, J., & Sedlmeier, P. (2012). The effects of mindfulness meditation: a meta-analysis. Mindfulness, 3(3), 174–189. https://doi.org/10.1007/s12671-012-0101-x.
Erogul, M., Singer, G., McIntyre, T., & Stefanov, D. G. (2014). Abridged mindfulness intervention to support wellness in first-year medical students. Teaching and Learning in Medicine, 26(4), 350–356. https://doi.org/10.1080/10401334.2014.945025.
Evans, S., Wyka, K., Blaha, K. T., & Allen, E. S. (2018). Self-compassion mediates improvement in well-being in a mindfulness-based stress reduction program in a community-based sample. Mindfulness, 9(4), 1280–1287. https://doi.org/10.1007/s12671-017-0872-1.
Feldman, C., & Kuyken, W. (2011). Compassion in the landscape of suffering. Contemporary Buddhism, 12(1), 143–155. https://doi.org/10.1080/14639947.2011.564831.
Field, A. P., & Gillett, R. (2010). How to do a meta-analysis. British Journal of Mathematical and Statistical Psychology, 63, 665–694. https://doi.org/10.1348/000711010X502733.
Garlow, S. J., Rosenberg, J., Moore, J. D., Haas, A. P., Koestner, B., Hendin, H., & Nemeroff, C. B. (2008). Depression, desparation and suicidal ideation in college students: results from the American Foundations for Suicide Prevention college screening project at Emory University. Depression and Anxiety, 25, 482–488. https://doi.org/10.1002/da.20321.
Gilbert, P. (2009). The compassionate mind: a new approach to life’s challenges. London: Constable and Robinson Ltd.
Gilbert, P., & Choden. (2015). Mindful compassion. Robinson.
Gilbert, P., McEwan, K., Matos, M., & Rivis, A. (2011). Fears of compassion: development of three self-report measures. Psychology and Psychotherapy: Theory, Research and Practice, 84(3), 239–255. https://doi.org/10.1348/147608310X526511.
Gilbert, P., Catarino, F., Duarte, C., Matos, M., Kolts, R., Stubbs, J., Ceresatto, L., Duarte, J., Pinto-Gouveia, J., & Basran, J. (2017). The development of compassionate engagement and action scales for self and others. Journal of Compassionate Health Care, 4(1), 4. https://doi.org/10.1186/s40639-017-0033-3.
Gilpin, R. (2008). The use of Theravāda Buddhist practices and perspectives in mindfulness-based cognitive therapy. Contemporary Buddhism, 9(2), 227–251. https://doi.org/10.1080/14639940802556560.
Greeson, J. M., Juberg, M. K., Maytan, M., James, K., & Rogers, H. (2014). A randomized controlled trial of Koru: a mindfulness program for college students and other emerging adults. Journal of American College Health, 62(4), 222–233. https://doi.org/10.1080/07448481.2014.887571.
Gu, J., Strauss, C., Bond, R., & Cavanagh, K. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12. https://doi.org/10.1016/j.cpr.2015.01.006.
Gu, J., Cavanagh, K., & Strauss, C. (2018). Investigating the specific effects of an online mindfulness-based self-help intervention on stress and underlying mechanisms. Mindfulness, 9, 1245–1257. https://doi.org/10.1007/s12671-017-0867-y.
Hedges, L. (1981). Distribution theory for Glass’s estimator of effect size and related estimators. Journal of Educational Statistics, 6, 107–128.
Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. Academic Press.
Hofmann, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. Journal of Consulting and Clinical Psychology, 78(2), 169–183. https://doi.org/10.1037/a0018555.
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537–559. https://doi.org/10.1177/1745691611419671.
Hou, R. J., Wong, S. Y. S., Yip, B. H. K., Hung, A. T. F., Lo, H. H. M., Chan, P. H. S., Lo, C. S. L., Kwok, T. C. Y., Tang, W. K., Mak, W. W. S., Mercer, S. W., & Ma, S. H. (2014). The effects of mindfulness-based stress reduction program on the mental health of family caregivers: a randomized controlled trial. Psychotherapy and Psychosomatics, 83(1), 45–53. https://doi.org/10.1159/000353278.
Huberty, J., Green, J., Glissmann, C., Larkey, L., Puzia, M., & Lee, C. (2019). Efficacy of the mindfulness meditation mobile app “calm” to reduce stress among college students: randomized controlled trial. JMIR mHealth and uHealth, 7(6), e14273. https://doi.org/10.2196/14273.
Huedo-Medina, T. B., Sánchez-Meca, J., Marín-Martínez, F., & Botella, J. (2006). Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychological Methods, 11(2), 193–206. https://doi.org/10.1037/1082-989X.11.2.193.
Hwang, Y. S., Goldstein, H., Medvedev, O. N., Singh, N. N., Noh, J. E., & Hand, K. (2019). Mindfulness-based intervention for educators: effects of a school-based cluster randomized controlled study. Mindfulness, 10, 1417–1436. https://doi.org/10.1007/s12671-019-01147-1.
James, K., & Rimes, K. A. (2018). Mindfulness-based cognitive therapy versus pure cognitive behavioural self-help for perfectionism: a pilot randomised study. Mindfulness, 9(3), 801–814. https://doi.org/10.1007/s12671-017-0817-8.
Kabat-Zinn, J. (1990). Full catastrophe living: using the wisdom of your body and mind to face stress, pain and illness. Delacourt.
Kabat-Zinn, J. (1994). Wherever you go there you are. Hyperion.
Kabat-Zinn, J. (1996). Mindfulness meditation: what it is, what it isn’t, and its role in health care and medicine. In Y. Haruki, Y. Ishii, & M. Suzuki (Eds.), Comparative and psychological study on meditation (pp. 161–170). Eburon.
Kirby, J. N., Tellegen, C. L., & Steindl, S. R. (2017). A meta-analysis of compassion-based interventions: current state of knowledge and future directions. Behavior Therapy, 48(6), 778–792. https://doi.org/10.1016/j.beth.2017.06.003.
Körner, A., Coroiu, A., Copeland, L., Gomez-Garibello, C., Albani, C., Zenger, M., & Brähler, E. (2015). The role of self-compassion in buffering symptoms of depression in the general population. PLoS One, 10(10), e0136598. https://doi.org/10.1371/journal.pone.0136598.
Kuyken, W., Watkins, E., Holden, E., White, K., Taylor, R. S., Byford, S., Evans, A., Radford, S., Teasdale, J. D., & Dalgleish, T. (2010). How does mindfulness-based cognitive therapy work? Behaviour Research and Therapy, 48(11), 1105–1112. https://doi.org/10.1016/j.brat.2010.08.003.
Kuyken, W., Warren, F. C., Taylor, R. S., Whalley, B., Crane, C., Bondolfi, G., Hayes, R., Huijbers, M., Ma, H., Schweizer, S., Segal, Z., Speckens, A., Teasdale, J. D., Van Heeringen, K., Williams, M., Byford, S., Byng, R., & Dalgleish, T. (2016). Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse. JAMA Psychiatry, 73(6), 565–574. https://doi.org/10.1001/jamapsychiatry.2016.0076.
Lever Taylor, B., Strauss, C., Cavanagh, K., & Jones, F. (2014). The effectiveness of self-help mindfulness-based cognitive therapy in a student sample: a randomised controlled trial. Behaviour Research and Therapy, 63, 63–69. https://doi.org/10.1016/j.brat.2014.09.007.
MacBeth, A., & Gumley, A. (2012). Exploring compassion: a meta-analysis of the association between self-compassion and psychopathology. Clinical Psychology Review, 32(6), 545–552. https://doi.org/10.1016/j.cpr.2012.06.003.
Meline, T. (2006). Selecting studies for systematic review: inclusion and exclusion criteria. Contemporary Issues In Communication Science and Disorders, 33, 21–27.
Mistretta, E. G., Davis, M. C., Temkit, M., Lorenz, C., Darby, B., & Stonnington, C. M. (2018). Resilience training for work-related stress among health care workers. Journal of Occupational and Environmental Medicine, 60(6), 559–568. https://doi.org/10.1097/JOM.0000000000001285.
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses : the PRISMA statement. Journal of Clinical Epidemiology, 62, 1006–1012. https://doi.org/10.1016/j.jclinepi.2009.06.005.
Morris, S. B. (2008). Estimating effect sizes from pretest-posttest-control group designs. Organizational Research Methods, 11, 364–386.
Moss, A. S., Reibel, D. K., Greeson, J. M., Thapar, A., Bubb, R., Salmon, J., & Newberg, A. B. (2015). An adapted mindfulness-based stress reduction program for elders in a continuing care retirement community: quantitative and qualitative results from a pilot randomized controlled trial. Journal of Applied Gerontology, 34, 518–538. https://doi.org/10.1177/0733464814559411.
National Collaborating Centre for Methods and Tools (2008). Quality assessment tool for quantitative studies. http://dev.nccmt.ca/resources/search/14.
Neff, K. D. (2003a). Self-compassion: an alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2, 85–101. https://doi.org/10.1080/15298860309032.
Neff, K. D. (2003b). The development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250. https://doi.org/10.1080/15298860390209035.
Neff, K. D. (2016). The self-compassion scale is a valid and theoretically coherent measure of self-compassion. Mindfulness, 7(1), 264–274. https://doi.org/10.1007/s12671-015-0479-3.
Neff, K. D., Rude, S. S., & Kirkpatrick, K. L. (2007). An examination of self-compassion in relation to positive psychological functioning and personality traits. Journal of Research in Personality, 41, 908–916. https://doi.org/10.1016/j.jrp.2006.08.002.
O’Donnell, R. M. R. (2017). Pilot RCT of mindfulness-based stress reduction (MBSR) versus progressive muscle relaxation (PMR) to reduce symptoms of distress among elderly dementia caregivers: results at one year post-intervention. Dissertation abstracts international: Section B: The sciences and engineering. ProQuest Information & Learning, US. http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2017-43829-024&site=ehost-live.
Orwin, R. G. (1983). A fail-safe N for effect size in meta-analysis. Journal of Educational Statistics, 8, 157–159.
Perez-Blasco, J., Viguer, P., & Rodrigo, M. F. (2013). Effects of a mindfulness-based intervention on psychological distress, well-being, and maternal self-efficacy in breast-feeding mothers: results of a pilot study. Archives of Women’s Mental Health, 16(3), 227–236. https://doi.org/10.1007/s00737-013-0337-z.
Peters, J., Sutton, A. J., Jones, D. R., Abrams, K., & Rushton, L. (2007). Performance of the trim and fill method in the presence of publication bias and between-study heterogeneity. Statistics in Medicine, 26, 4544–4562. https://doi.org/10.1002/sim.
Potharst, E. S., Boekhorst, M. G. B. M., Cuijlits, I., van Broekhoven, K. E. M., Jacobs, A., Spek, V., Nyklíček, I., Bögels, S. M., & Pop, V. J. M. (2019). A randomized control trial evaluating an online mindful parenting training for mothers with elevated parental stress. Frontiers in Psychology, 10, 1550. https://doi.org/10.3389/fpsyg.2019.01550.
Roemer, L., Lee, J. K., Salters-Pedneault, K., Erisman, S. M., Orsillo, S. M., & Mennin, D. S. (2009). Mindfulness and emotion regulation difficulties in generalized anxiety disorder: preliminary evidence for independent and overlapping contributions. Behavior Therapy, 40, 142–154. https://doi.org/10.1016/j.beth.2008.04.001.
Schaufeli, W. B., Bakker, A. B., & Van Rhenen, W. (2009). How changes in job demands and resources predict burnout, work engagement, and sickness absenteeism. Journal of Organizational Behavior, 30(7), 893–917. https://doi.org/10.1002/job.595.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. (2002). Mindfulness-based cognitive therapy for depression: a new approach to preventing relapse. Guilford Press.
Sevinc, G., Hoelzel, B. K., Hashmi, J., Greenberg, J., McCallister, A., Treadway, M., Schneider, M. L., Dusek, J. A., Carmody, J., & Lazar, S. W. (2018). Common and dissociable neural activity after mindfulness-based stress reduction and relaxation response programs. Psychosomatic Medicine, 80(5), 439–451. https://doi.org/10.1097/PSY.0000000000000590.
Shapiro, S. L., Astin, J. A., Bishop, S. R., & Cordova, M. (2005). Mindfulness-based stress reduction for health care professionals: results from a randomized trial. International Journal of Stress Management, 12, 164–176. https://doi.org/10.1037/1072-5245.12.2.164.
Shapiro, S. L., Brown, K. W., Thoresen, C., & Plante, T. G. (2011). The moderation of mindfulness-based stress reduction effects by trait mindfulness: results from a randomized controlled trial. Journal of Clinical Psychology, 67(3), 267–277. https://doi.org/10.1002/jclp.20761.
Shore, R., Strauss, C., Cavanagh, K., Hayward, M., & Ellett, L. (2018). A randomised controlled trial of a brief online mindfulness-based intervention on paranoia in a non-clinical sample. Mindfulness, 9, 294–302. https://doi.org/10.1007/s12671-017-0774-2.
Smith, J. M., Bright, K. S., Mader, J., Smith, J., Afzal, A. R., Patterson, C., Dimitropolous, G., & Crowder, R. (2020). A pilot of a mindfulness based stress reduction intervention for female caregivers of youth who are experiencing substance use disorders. Addictive Behaviors, 103, 106223. https://doi.org/10.1016/j.addbeh.2019.106223.
Spijkerman, M. P. J., Pots, W. T. M., & Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: a review and meta-analysis of randomised controlled trials. Clinical Psychology Review, 45, 102–114. https://doi.org/10.1016/j.cpr.2016.03.009.
Ștefan, C. A., Căpraru, C., & Szilágyi, M. (2018). Investigating effects and mechanisms of a mindfulness-based stress reduction intervention in a sample of college students at risk for social anxiety. Mindfulness, 9, 1509–1521. https://doi.org/10.1007/s12671-018-0899-y.
Stjernswärd, S., & Hansson, L. (2017). Effectiveness and usability of a web-based mindfulness intervention for families living with mental illness. Mindfulness, 8(3), 751–764. https://doi.org/10.1007/s12671-016-0653-2.
Strauss, C., Cavanagh, K., Oliver, A., & Pettman, D. (2014). Mindfulness-based interventions for people diagnosed with a current episode of an anxiety or depressive disorder: a meta-analysis of randomised controlled trials. PLoS One, 9(4), e96110. https://doi.org/10.1371/journal.pone.0096110.
Strauss, C., Lever Taylor, B., Gu, J., Kuyken, W., Baer, R., Jones, F., & Cavanagh, K. (2016). What is compassion and how can we measure it? A review of definitions and measures. Clinical Psychology Review, 47, 15–27. https://doi.org/10.1016/j.cpr.2016.05.004.
Terrin, N., Schmid, C. H., Lau, J., & Olkin, I. (2003). Adjusting for publication bias in the presence of heterogeneity. Statistics in Medicine, 22, 2113–2126. https://doi.org/10.1002/sim.1461.
The Cochrane Collaboration. (2011). Cochrane handbook for systematic reviews of interventions version 5.1.0. (J. P. T. Higgins & S. Green, Eds.). http://www.handbook.cochrane.org.
The Cochrane Collaboration. (2014). Review Manager (RevMan) Version 5.3. The Nordic Cochrane Centre.
Van Dam, N. T., Sheppard, S. C., Forsyth, J. P., & Earleywine, M. (2011). Self-compassion is a better predictor than mindfulness of symptom severity and quality of life in mixed anxiety and depression. Journal of Anxiety Disorders, 25(1), 123–130. https://doi.org/10.1016/j.janxdis.2010.08.011.
Van Dam, N. T., Van Vugt, M. K., Vago, D. R., Schmalzl, L., Saron, C. D., Olendzki, A., Meissner, T., Lazar, S. W., Kerr, C. E., Gorchov, J., Fox, K. C. R., Field, B. A., Britton, W. B., Brefczynski-Lewis, J. A., & Meyer, D. E. (2018). Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13, 36–61. https://doi.org/10.1177/1745691617709589.
Williams, M. J., Dalgleish, T., Karl, A., & Kuyken, W. (2014). Examining the factor structures of the five facet mindfulness questionnaire and the self-compassion scale. Psychological Assessment, 26, 407–418. https://doi.org/10.1037/a0035566.
Wilson, A. C., Mackintosh, K., Power, K., & Chan, S. W. Y. (2019). Effectiveness of self-compassion related therapies: a systematic review and meta-analysis. Mindfulness, 10(6), 979–995. https://doi.org/10.1007/s12671-018-1037-6.
Zessin, U., Dickhauser, O., & Garbade, S. (2015). The relationship between self-compassion and well-being: a meta-analysis. Applied Psychology: Health and Wellbing, 7(3), 340–364. https://doi.org/10.1111/aphw.12051.
Author information
Authors and Affiliations
Contributions
HG: designed and executed the review, conducted the data analyses, wrote the first draft of the manuscript and provided revisions of the manuscript. JV: collaborated with the design and writing of the review. JK: collaborated with the writing of the review. LE: collaborated with the design and provided revisions of the manuscript. All of the authors approved the final version of the manuscript for submission.
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Golden, H.L., Vosper, J., Kingston, J. et al. The Impact of Mindfulness-Based Programmes on Self-Compassion in Nonclinical Populations: a Systematic Review and Meta-Analysis. Mindfulness 12, 29–52 (2021). https://doi.org/10.1007/s12671-020-01501-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-020-01501-8