
Abstract
Background
Antimicrobial resistance has decreased eradication rates for Helicobacter pylori infection worldwide. A sequential treatment schedule has been reported to be effective, but studies published to date were performed in Italy. We undertook this study to determine whether these results could be replicated in India.
Methods
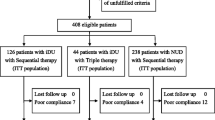
A randomized, open-labeled, prospective controlled trial comparing sequential vs. standard triple-drug therapy was carried out at Lokmanya Tilak Municipal General Hospital, Mumbai. Two hundred and thirty-one patients with dyspepsia were randomized to a 10-day sequential regimen (40 mg of pantoprazole, 1 g of amoxicillin, each administered twice daily for the first 5 days, followed by 40 mg of pantoprazole, 500 mg of clarithromycin, and 500 mg of tinidazole, each administered twice daily for the remaining 5 days) or to standard 14-day therapy (40 mg of pantoprazole, 500 mg of clarithromycin, and 1 g of amoxicillin, each administered twice daily).
Results
The eradication rate achieved with the sequential regimen was significantly greater than that obtained with the triple therapy. Per-protocol eradication rate of sequential therapy was 92.4 % (95 % CI 85.8–96.1 %) vs. 81.8 % (95 % CI 73.9–87.8 %) (p = 0.027) for standard drug therapy. Intention-to-treat eradication rates were 88.2 % (95 % CI 80.9–93.0 %) vs. 79.1 % (95 % CI 71.1–85.4 %), p = 0.029, respectively. The incidence of major and minor side effects between therapy groups was not significantly different (14.6 % in the triple therapy group vs. 23.5 % in sequential group, p = 0.12). Follow up was incomplete in 3.3 % and 4.7 % patients in standard and sequential therapy groups, respectively. Sequential therapy includes one additional antibiotic (tinidazole) that is not contained in standard therapy.
Conclusions
Sequential therapy was significantly better than standard therapy for eradicating H. pylori infection.

Similar content being viewed by others


References
Megraud F. Epidemiology of Helicobacter pylori. Gastroenterol Clin North Am. 1993;22:73–88.
Malfertheiner P, Megraud F, O'Morain CA, et al. European Helicobacter Study Group. Management of Helicobacter pylori infection—the Maastricht IV/Florence Consensus Report. Gut. 2012;61:646–64.
Miehlke S, Kirsch C, Schneider-Brachert W, et al. A prospective, randomized study of quadruple therapy and high dose dual therapy for treatment of Helicobacter pylori resistant to both metronidazole and clarithromycin. Helicobacter. 2003;8:310–9.
Vakil N, Lanza F, Schwartz H, et al. Seven-day therapy for Helicobacter pylori in the United States. Aliment Pharmacol Ther. 2004;20:99–107.
Malfertheiner P, Megraud F, O'Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III consensus report. Gut. 2007;56:772–81.
Chiba N, Van Zanten SJ, Sinclair P, Ferguson RA, Escobedo S, Grace E. Treating Helicobacter pylori infection in primary care patients with uninvestigated dyspepsia: the Canadian adult dyspepsia empiric treatment-Helicobacter pylori positive (CADET-Hp) randomised controlled trial. BMJ. 2002;324:1012–6.
Zullo A, Rinaldi V, Winn S, et al. A new highly effective short-term therapy schedule for Helicobacter pylori eradication. Aliment Pharmacol Ther. 2000;14:715–8.
De Francesco V, Zullo A, Hassan C, et al. Two new treatment regimens for Helicobacter pylori eradication: a randomised study. Dig Liver Dis. 2001;33:676–9.
Zullo A, Vaira D, Vakil N, et al. High eradication rates of Helicobacter pylori with a new sequential treatment. Aliment Pharmacol Ther. 2003;17:719–26.
Vaira D, Zullo A, Vakil N, et al. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: a randomized trial. Ann Intern Med. 2007;146:556–63.
Zullo A, De Francesco V, Hassan C, Morini S, Vaira D. The sequential therapy regimen for Helicobacter pylori eradication: a pooled-data analysis. Gut. 2007;56:1353–7.
Chaudhuri S, Chowdhury A, Datta S, et al. Anti-Helicobacter pylori therapy in India: differences in eradication efficiency associated with particular alleles of vacuolating cytotoxin (vacA) gene. J Gastroenterol Hepatol. 2003;18:190–5.
Valooran GJ, Kate V, Jagdish S, et al. Sequential therapy versus standard triple drug therapy for eradication of Helicobacter pylori in patients with perforated duodenal ulcer following simple closure. Scand J Gastroenterol. 2011;46:1045–50.
Francavilla R, Lionetti E, Castellaneta SP, et al. Improved efficacy of 10-day sequential treatment for Helicobacter pylori eradication in children: a randomized trial. Gastroenterology. 2005;129:1414–9.
Hassan C, De Francesco V, Zullo A, et al. Sequential treatment for Helicobacter pylori eradication in duodenal ulcer patients: improving the cost of pharmacotherapy. Aliment Pharmacol Ther. 2003;18:641–6.
Amarapurkar D, Makesar M, Amarapurkar A, Das HS. Helicobacter pylori eradication: efficacy of conventional therapy in India. Trop Doct. 2004;34:101–2.
Kumar D, Ahuja V, Dhar A, et al. Randomized trial of a quadruple-drug regimen and a triple-drug regimen for eradication of Helicobacter pylori: long-term follow-up study. Indian J Gastroenterol. 2001;20:191–4.
Thyagarajan SP, Ray P, Das BK, et al. Geographical difference in antimicrobial resistance pattern of Helicobacter pylori clinical isolates from Indian patients: multicentric study. J Gastroenterol Hepatol. 2003;18:1373–8.
Datta S, Chattopadhyay S, Patra R, et al. Most Helicobacter pylori strains of Kolkata in India are resistant to metronidazole but susceptible to other drugs commonly used for eradication and ulcer therapy. Aliment Pharmacol Ther. 2005;22:51–7.
Ramakrishna BS. Helicobacter pylori infection in India: the case against eradication. Indian J Gastroenterol. 2006;25:25–8.
Moayyedi P, Soo S, Deeks J, et al. Eradication of Helicobacter pylori for non-ulcer dyspepsia. Cochrane Database Syst Rev. 2005;1, CD002096.
Talley NJ, Vakil N. Guidelines for the management of dyspepsia. Am J Gastroenterol. 2005;100:2324–37.
Bhasin DK, Sharma BC, Ray P, Pathak CM, Singh K. Comparison of seven and fourteen days of lansoprazole, clarithromycin, and amoxicillin therapy for eradication of Helicobacter pylori: a report from India. Helicobacter. 2000;5:84–7.
Bhatia V, Ahuja V, Das B, Bal C, Sharma MP. Use of imidazole-based eradication regimens for Helicobacter pylori should be abandoned in North India regardless of in vitro antibiotic sensitivity. J Gastroenterol Hepatol. 2004;19:619–25.
Bapat MR, Abraham P, Bhandarkar PV, Phadke AY, Joshi AS. Acquisition of Helicobacter pylori infection and reinfection after its eradication are uncommon in Indian adults. Indian J Gastroenterol. 2000;19:172–4.
Nanivadekar SA, Sawant PD, Patel HD, Shroff CP, Popat UR, Bhatt PP. Association or peptic ulcer with Helicobacter pylori and the recurrence rate. A three year follow up study. J Assoc Physicians India. 1990;38 Suppl 1:703–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nasa, M., Choksey, A., Phadke, A. et al. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: A randomized study. Indian J Gastroenterol 32, 392–396 (2013). https://doi.org/10.1007/s12664-013-0357-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-013-0357-7