
Abstract
Physical inactivity is a global public health challenge. At the same time, the societal transformation toward a sustainable and active lifestyle can be observed. Active travel (AT) is one physical activity (PA) domain and combines healthy and sustainable daily behavior. However, it is still unclear whether assumed associations between AT and health are resilient for objective and subjective health outcomes. Since published research on AT has been growing during the last decade, this scoping review aimed to update and summarize the existing evidence. Therefore, a scoping review was conducted in PubMed, Web of Science, ScienceDirect, and Cochrane Library, following PRISMA guidelines. In all, 35 papers including 4,857,918 individuals (age range: 18–93 years old) were included. AT is strongly associated with health dimensions with a great body of knowledge showing strong associations between AT and reduced risks for noncommunicable diseases (NCD), especially in comparison to non-AT. Thus, AT can play an important role to prevent the increasing prevalence of NCD. There is a limited amount of research available on health-promoting factors and subjective health. Extracted studies suggest positive connections with AT. Mostly, cycling as a form of AT seems to have a more significant positive association with health compared to walking. Longitudinal studies further support and reinforce these findings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Physical inactivity is a major public health challenge. In high-income countries, noncommunicable diseases (NCD), e.g., ischemic heart disease and diabetes, are the leading causes of mortality and morbidity. For physical activity (PA) recommendations (WHO, 2020), minimum PA levels for achieving health-promoting and disease-preventing effects have been formulated based on scientific evidence. Accordingly, adults (≥ 18 years) should engage in at least 150–300 min of moderate-intensity aerobic PA or 75–150 min of vigorous-intensity aerobic PA or an equivalent combination of moderate- and vigorous-intensity PA throughout the week (MVPA), for substantial health benefits, and at least 2 days/week of muscle-strengthening exercise (MSE) for additional health benefits. However, the health-promoting potential of exercise (Warburton & Bredin, 2017) is not yet fully exploited in societies. Approximately two-thirds of adults meet the MVPA guidelines globally (Garcia-Hermoso et al., 2022). A higher and continuously increasing prevalence of insufficient MVPA exists in high-income countries (37%: Guthold, Stevens, Riley, & Bull, 2018; specifically for Germany reaching almost 55%: Bennie, de Cocker, & Tittlbach, 2021). PA cannot “only” represent a healthy behavior but plays a significant role in building a healthy and sustainable lifestyle (Nigg & Nigg, 2021). When discussing PA promotion, different dimensions of PA are analyzed: leisure-time PA (LTPA), sports, occupational PA, and active travel (AT). This paper will focus on the latter due to the mobility turnaround toward more sustainable and healthier behaviors, and subsequent increase in the popularity of cycling and walking as AT (Hoor, 2023).
AT, meaning muscle powered and non-motorized locomotion, such as walking, cycling, inline skating, or scootering, is further defined as travel in which the sustained physical exertion of the traveler directly contributes to their motion (Cook, Stevenson, Aldred, Kendall, & Cohen, 2022). Human-powered locomotion can increase health parameters, e.g., heart rate and blood pressure (Larouche, Faulkner, & Tremblay, 2016), activate the whole musculoskeletal system to enhance physical performance (Henriques-Neto et al., 2020), and challenges cognitive parameters (Phansikar & Mullen, 2019). Consequently, a sustainable and active lifestyle comes together in AT (Fröberg & Lundvall, 2021; Maltese, Gatta, & Marcucci, 2021; Nigg & Nigg, 2021; Ribeiro & Fonseca, 2022).
In a review of previous literature examining the associations between AT and health outcomes, it becomes obvious that there is a strong focus on children and youth (e.g., Lubans, Boreham, Kelly, & Foster, 2011; Voulgaris, Smart, & Taylor, 2019). When examining adults, selected physical health outcomes, in the sense of disease prevention, are the main focus (e.g., cardiovascular disease [CVD] mortality) (Hamer & Chida, 2008). Research in adults reports potential positive health effects, but also still inconsistent findings on whether AT contributes robustly to better and comprehensive health outcomes (Dinu, Pagliai, Macchi, & Sofi, 2019). In addition, there is a lack of thorough examination of subjective and mental health measures in terms of holistic health. The importance of health promotion factors, i.e., subjective health assessment as well as mental health, are highlighted from a salutogenic health perspective (Keyes, 2014). Comprehensive reviews on the associations between AT and health promoting factors, respectively mental health, cannot be found.
Increased PA is identified as the most important determinant of health benefits of AT in adults (Mueller et al., 2015). Until recently, it was not completely clear whether AT contributes to increasing PA levels or whether other forms of LTPA may be substituted (Saunders, Green, Petticrew, Steinbach, & Roberts, 2013). The systematic review of Wanjau et al. (2023) has shown that the vast majority of studies reveal no displacement of PA in other domains. Rarely (if at all) could small amounts of compensatory reduction in PA in other domains be found. This means that AT can positively increase overall levels of PA. Dual-mode travelers (walking + cycling) especially met, or were close to meeting, the recommended PA levels of at least 150 min/week, while ‘cyclists only’ met the guidelines only during spring–fall period (Stigell & Schantz, 2015). Also, combining AT with the use of public transport (PT) can help to meet the PA recommendations (Rissel, Curac, Greenaway, & Bauman, 2012; Lachapelle, Frank, Saelens, Sallis, & Conway, 2011).
Oriented to the research gaps listed, and due to the fact that published research on AT has been growing during the last decade, this scoping review aimed to update and summarize the existing evidence to answer the question whether AT is associated with positive—objective and subjective—health parameters.
Methods
A literature search following the Extension for Scoping Reviews of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR) guidelines (Tricco et al., 2018) was carried out to answer the research questions.
Inclusion and exclusion criteria
The inclusion criteria for eligibility were as follows:
-
1.
Study design: cross-sectional and longitudinal epidemiological studies or reviews,
-
2.
Considered modes of AT: Covering distances necessary in everyday life through cycling, walking, scootering or inline-skating,
-
3.
Outcome: any health aspects (e.g., obesity, mortality, physical fitness, mental health),
-
4.
Data analysis: analysis of the association between AT behavior and health,
-
5.
Sample: male and female adults (≥ 18 years) in Western industrialized countries with urban infrastructure and lifestyles comparable to Europe, to limit the potential of unknown cultural influences on activity behavior,
-
6.
Language: published in English or German, and
-
7.
Publication date: The importance of research into AT has risen sharply and has been intensively researched in the last few years. Therefore, the publication dates for this review have been restricted to the previous decade, hence, 2013 until 2023.
Exclusion criteria were as follows:
-
8.
Papers not meeting all the inclusion criteria (1)–(7),
-
9.
Study sample n < 100,
-
10.
Analysis of impact on health solely through air pollution caused by traffic,
-
11.
Studies dealing exclusively with people aged ≥ 80 years of age, and
-
12.
Exclusive focus on e‑biking.
The last search update was on 1 September 2023.
Search strategy
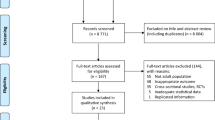
The review was embedded in an extensive literature review with several research questions, namely on the associations of AT with health and PA, AT’s environmental effects, its socioecological determinants, and participatory intervention options for increasing AT behavior. Therefore, the initial search strategy refers to all of these aspects (see steps identification, screening, and eligibility in Fig. 1). However, in this paper, the review presents results for only the associations of AT with health.

Flowchart of the identified studies investigating associations of active travel (AT) and health
The electronic databases PubMed, Web of Science, ScienceDirect, and The Cochrane Library were searched using predefined combinations of keywords sought in the title and abstracts of the papers. See Appendix (Tables 3, 4, 5 and 6) for the detailed listing of all search terms. The research was complemented by a manual search (snowball system).
The review protocol was registered in Open Science Framework (OSF; https://doi.org/10.17605/OSF.IO/2NPRM).
Internal validity
To avoid potential bias and reduce the risk of excluding studies that met inclusion criteria, three investigators independently screened titles, abstracts (S.T., A.B., S.K.), and full texts (S.T., S.K.) for eligibility. Disagreements were resolved by consensus.
Results
Search results and study characteristics
Figure 1 provides a flowchart summarizing the included and excluded papers. The literature search resulted in 35 papers including 4,857,918 individuals. The 16 cross-sectional and 12 longitudinal studies were performed in the US (8), the UK (7), Sweden (2), Finland (3), China (2), the Netherlands (2), and several European cities (Denmark, Norway, Switzerland, Ireland; each 1). In seven of the found papers, three reviews included cross-sectional and longitudinal studies, two included longitudinal studies only, and two included cross-sectional studies only. The studies included in these reviews were conducted mainly in Europe, Australia, China, Japan, Canada, and the US. Participants of the included studies are mostly 18+ years old, with some starting at 16 years old. Except for one study (men only, Vaara, Vasankari, Fogelholm, Koski, & Kyröläinen, 2020), all studies investigated male and female adults. Investigated modes of travel were walking and cycling (30 papers), walking only (2), or cycling only (3) in comparison to non-active travel modes. In addition, 16 of the 28 single studies and five of the reviews compared AT to car travel or motorized private transport, respectively, or made specific comparisons to PT. In the other papers, it is not clear to what extent AT is differentiated from other mobility modes. Besides walking and cycling, there were no other ways of AT investigated in the eligible papers.
The main characteristics of the studies are presented in Tables 1 and 2 and summarized below.
The associations between AT and health parameters have been intensively researched. However, there was not a balanced distribution between objective and subjective health parameters. Nineteen studies and seven reviews assessed associations with objective parameters, i.e., cardiovascular respectively cardiometabolic diseases and diabetes (3, 6, 9, 10, 23–25, 27, 28, 30, 32–34)Footnote 1, obesity and body composition (3, 4, 5, 7, 14, 16, 17, 19, 24, 25, 27, 29, 31, 35), mortality (20, 22), cancer (22, 30), chronic diseases in general (5), and physical fitness (6, 27, 31). Only eight studies and one review assessed subjective health parameters, e.g., mental and self-rated health (1, 2, 7, 13, 15, 16, 18, 26, 33).
Associations of AT and disease-preventing parameters
In general, positive associations could be found between AT and chronic diseases (5). When looking at specific disease-preventing parameters, strong associations between AT (walking and cycling) and reduced risk for cardiovascular and cardiometabolic diseases were found (3, 6, 9–11, 21, 23–25, 27, 28, 30, 32, 33). Cycling as AT revealed health advantages in some studies (3, 24, 30, 33), while walking was not inversely associated with clustered cardiometabolic risk (27) but helped to lower blood pressure and hypertension (24). The existing longitudinal studies and reviews strengthen the hypothesis of the health advantage of cycling as AT. They showed significant impacts of cycling on cardiovascular and cardiometabolic diseases (10, 11, 30, 33) as well as on more critical objective health parameters, such as lower risks of mortality (all-cause 20%, CVD 24%, cancer 16%) and cancer (11%) (20, 22, 30). In longitudinal studies, walking as AT was found to be associated with reduced risk of mortality as well, but the risk reduction was much lower than in cycling (all-cause mortality 8%, CVD 9%, cancer 7%) (22, 30). Regarding the distance, AT walkers covered between 0.4 km (short-term) and 9.7 km (long-term) on average, and cyclists covered 1.3 km (short-term) and 10.8 km (long-term) (22). Hazard ratios suggested commensurate effects on health in favor of distance but not mode (7, 22).
Compared to these parameters, the association of AT with overweight/obesity is not as clear. The majority of the papers (12 papers) showed small but positive associations between AT (walking and/or cycling) and parameters of body composition, in particular lowering the risk of obesity (3, 4, 8, 11, 14, 17, 19, 24, 25, 27, 33, 35). This was especially apparent in comparison to non-AT modes, e.g., travel with car/motor vehicle/PT. However, four papers showed no clear associations, especially when looking at being overweight in general opposed to being obese (7, 16, 29, 32) and one paper (13) showed no association between AT and being overweight or obesity respective, which means that the evidence for an effect of AT on obesity is still inconclusive (29), and it could not be determined whether walking or cycling are more powerful as AT. Some longitudinal studies showed that walking could reduce waist circumference and the risk of abdominal obesity (32), while others showed that cycling as AT may reduce the risk of obesity (33). Other studies found positive effects of AT on BMI for both travel modes (8), but no rehabilitative effect for obese people. Furthermore, being overweight or obese was assumed to decrease bicycle use (7). Finally, walking distance has a positive impact on BMI, as indicated by a study where individuals who walked at least 3 km per day were less likely to be obese compared to non-active commuters (15). Among individuals who cycled exclusively, there was a correlation between commuting distance and body fat, but not for walking (16).
Associations of AT and health-promoting parameters
Both walking and cycling were associated with greater cardiovascular (6) and physical fitness (6, 27) and this relationship was particularly visible in the case of cycling as AT (27, 31). No longitudinal studies were identified which support this outcome. Most of the studies assessing subjective health parameters indicated a positive association with AT (2, 8, 12). In particular, cycling was linked with positive mental health cross-sectionally (26) as well as longitudinally (1, 18), and only one study could not find any associations between AT and self-rated health (16). The health promotion significance of cycling as AT, increasing with distance, also becomes clear (7). Other investigations gathering distance data did not draw any conclusions with regard to health (31).
Discussion
This review investigated the existing literature over the last decade (2013–2023) that examined associations between AT and general health parameters. Our review reveals both a growing interest in the health impact of AT but also an inconsistent landscape in terms of research methods and designs. On the one hand, there has been a noticeable increase in longitudinal research and reviews over the past decade, with 12 longitudinal studies and seven systematic reviews identified. In addition, there are three reviews that combine longitudinal and cross-sectional studies. However, it is worth noting that cross-sectional studies continue to be prevalent, with 16 conducted in the same time frame. In response to the research question, data largely indicate that AT has significant associations with several health parameters, but the associations are partly dependent on travel mode and/or type of health parameter.
Most of the studies target objective parameters, e.g., cardiovascular and cardiometabolic risks, particularly diseases which are of central importance for public health (Zemedikun, Gray, Khunti, Davies, & Dhalwani, 2018). In this review AT proved to have inversed associations with both cardiovascular and cardiometabolic risks.
The available longitudinal studies make clear that cycling has stronger disease-preventing effects than walking (Dinu et al., 2019; Peruzzi et al., 2020; Patterson et al., 2020; Mytton, Panter, & Ogilvie, 2016a). This is physiologically explicable since cycling evokes a higher cardiovascular load and therefore leads to a higher MVPA (Vaara et al., 2020). Thus, engaging in PA of sufficient duration and intensity can lead to improvement in cardiometabolic health, which is not given in walking only.
However, walking may have some beneficial health effects. If certain conditions are met, walking can have significant impact on disease prevention. Reduction of cardiovascular diseases through AT is shown longitudinally regardless of mode and dose, when investigating individuals with sedentary work lifestyles, inconsistent exercise routines, a history of being overweight or obese, and low physical fitness levels (Eriksson et al., 2020).
However, when summarizing the information out of cross-sectional and longitudinal studies about the prevention of obesity, the associations with and impacts of AT on obesity prevention are weak and inconsistent, so no robust conclusion can be drawn. Also, the inverse effect does exist, meaning that increased overweight is negatively connected to bicycle use (de Haas, Kroesen, Chorus, Hoogendoorn-Lanser, & Hoogendoorn, 2021) and BMI does have a negative influence on walking behavior and later levels of AT (Kroesen & de Vos, 2020).
AT does also provide benefits to reduce even more serious health problems like cancer or mortality risks. Inversed associations between AT and chronic diseases like diabetes were observed (Bopp, Kaczynski, & Campbell, 2013; Dinu et al., 2019; Saunders et al., 2013). Regarding mortality and cancer, cycling evokes stronger effects than walking only (Patterson et al., 2020; Dinu et al., 2019), which is in line with previous research (Shepard, 2008).
Besides the risk reduction of diseases, AT is strongly associated with health-promoting parameters like physical fitness (Bopp, Bopp, & Schuchert, 2015; Riiser, Solbraa, Jenum, Birkeland, & Andersen, 2018; Vaara et al., 2020; Henriques-Neto et al., 2020). Only cross-sectional studies could be found on this health outcome, and additionally, the question, whether walking or cycling have a stronger relationship with fitness has not yet been consistently answered.
Fewer subjective than objective perspectives were gathered, but an increase of papers during the last five years is notable. The literature could confirm lower feelings of loneliness, more time spent with family and friends, and higher vitality after AT (Avila-Palencia et al., 2018; Tamminen et al., 2020), but the research was not fully consistent. Longitudinal effects of AT on self-rated health were found for cycling only (de Haas et al., 2021; Mytton, Panter, & Ogilvie, 2016b). Also, the authors highlighted that the effect of cycling on self-rated health is stronger than the reverse effect, and that those effects increased with travel distance. Avila-Palencia et al. (2018) also found positive associations of car travel on lower feelings of loneliness and Masterson and Phillips (2022) did not find any associations between AT and self-rated health.
Strengths and limitations
The strengths of this scoping review include the large databases searched, the large samples, and the holistic health approaches. Due to the variety and distribution of participants included in this review, risks of selection bias—which often occurs in intervention trials—are not expected to be present. Our scoping review can therefore help to give a broad overview and identify trends and research gaps. The extracted longitudinal studies help to foster such trends and allow inference of causal directions, i.e., the impact of AT on health, with the use of large sample sizes.
The scoping review also has some limitations. Including cross-sectional data is the main limitation since only associations and hints on evidence can be revealed. Based on the cross-sectional data, this review cannot answer the question if AT leads to improved health or if rather healthier individuals are more inclined to travel in an active mode (Kroesen & de Vos, 2020). Also, we identified some measurement and methodological issues. Numerous self-reported measurement tools such as questionnaires were used, which minimizes the objectiveness of the outcomes to a certain extent. No research gathered data of types of AT other than walking or cycling. Furthermore, there were inconsistencies in how AT was compared to non-active modes of travel, i.e., car or other motorized travel, or PT, and the categorization of AT across different studies (i.e., yes/no vs. minutes of AT with certain thresholds).
Conclusion
Active travel (AT), e.g., walking and cycling, can enhance several health parameters such as lowering the risk of obesity or result in greater cardiovascular and physical fitness. Therefore, AT can serve as a contribution to enhancing public health.
Still, not enough research has been done to disentangle which mode of AT is the best for health, but cycling does appear favorable when it comes to health benefits. It is also unclear whether health-promoting parameters or subjective health can be influenced in the same way as disease-preventing factors. Further longitudinal research is strongly recommended. Nonetheless, in times of increasing prevalence of noncommunicable diseases (NCD), world inactivity, and the need for societal transformation toward more sustainability, AT can play an important role in addressing these challenges.
References
Avila-Palencia, I., Int Panis, L., Dons, E., Gaupp-Berghausen, M., Raser, E., Götschi, T., Gerike, R., Brand, C., de Nazelle, A., Orjuela, J. P., Anaya-Boig, E., Stigell, E., Kahlmeier, S., Iacorossi, F., & Nieuwenhuijsen, M. J. (2018). The effects of transport mode use on self-perceived health, mental health, and social contact measures: a cross-sectional and longitudinal study. Environment International, 120, 199–206. https://doi.org/10.1016/j.envint.2018.08.002.
Barajas, J. M., & Braun, L. M. (2021). Are cycling and walking good for all? Tracking differences in associations among active travel, socioeconomics, gentrification, and self-reported health. Journal of Transport & Health, 23, 101246. https://doi.org/10.1016/j.jth.2021.101246.
Bennie, J. A., de Cocker, K., & Tittlbach, S. (2021). The epidemiology of muscle-strengthening and aerobic physical activity guideline adherence among 24,016 german adults. Scandinavian Journal of Medicine & Science in Sports, 31(5), 1096–1104. https://doi.org/10.1111/sms.13922.
Berger, A., Qian, X., & Pereira, M. (2018). Associations between bicycling for transportation and cardiometabolic risk factors among minneapolis—saint Paul area commuters: a cross-sectional study in working-Age adults. American Journal of Health Promotion, 32(3), 631–637. https://doi.org/10.1177/0890117117710735.
Berglund, E., Lytsy, P., & Westerling, R. (2016). Active traveling and its associations with self-rated health, BMI and physical activity: a comparative study in the adult Swedish population. International Journal of Environmental Research and Public Health, 13(5), 455. https://doi.org/10.3390/ijerph13050455.
Bopp, M., Kaczynski, A. T., & Campbell, M. E. (2013). Health-related factors associated with mode of travel to work. Journal of Environmental and Public Health. https://doi.org/10.1155/2013/242383.
Bopp, M., Bopp, C. M., & Schuchert, M. (2015). Active transportation to and on campus is associated with objectively measured fitness outcome among college students. Journal of Physical Activity and Health, 12(3), 418–423. https://doi.org/10.1123/jpah.2013-0332.
Brown, V., Moodie, M., Mantilla Herrera, A. M., Veerman, J. L., & Carter, R. (2017). Active transport and obesity prevention—A transportation sector obesity impact scoping review and assessment for Melbourne, Australia. Preventive Medicine, 96, 49–66. https://doi.org/10.1016/j.ypmed.2016.12.020.
Cook, S., Stevenson, L., Aldred, R., Kendall, M., & Cohen, T. (2022). More than walking and cycling: what is ‘active travel’? Transport Policy, 126, 151–161. https://doi.org/10.1016/j.tranpol.2022.07.015.
Dinu, M., Pagliai, G., Macchi, C., & Sofi, F. (2019). Active commuting and multiple health outcomes: a systematic review and meta-analysis. Sports Medicine, 49(3), 437–452. https://doi.org/10.1007/s40279-018-1023-0.
Echeverría, L., Gimenez-Nadal, J. I., & Molina, J. A. (2023). Active commuting and the health of workers. Journal of Transport & Health, 31, 101626. https://doi.org/10.1016/j.jth.2023.101626.
Eriksson, J. S., Ekblom, B., Kallings, L. V., Hemmingsson, E., Andersson, G., Wallin, P., Ekblom, Ö., & Ekblom-Bak, E. (2020). Active commuting in Swedish workers between 1998 and 2015—Trends, characteristics, and cardiovascular disease risk. Scandinavian Journal of Medicine & Science in Sports, 30(2), 370–379. https://doi.org/10.1111/sms.13581.
Fan, M., Lv, J., Guo, Y., Bian, Z., Yang, S., Yang, L., Chen, Y., Huang, Y., Chen, B., Fan, L., Chen, J., Chen, Z., Qi, L., Li, L., & & China Kadoorie Biobank Collaborative Group. (2019). Associations between active commuting and incident cardiovascular diseases in Chinese: a prospective cohort study. Journal of the American Heart Associations, 8(20), e12556. https://doi.org/10.1161/JAHA.119.012556.
Fröberg, A., & Lundvall, S. (2021). The distinct role of physical education in the context of agenda 2030 and sustainable development goals: an explorative review and suggestions for future work. Sustainability, 13(21), 11900. https://doi.org/10.3390/su132111900.
Garcia-Hermoso, A., López-Gil, J. F., Ramírez-Vélez, R., Alonso-Martínez, A. M., Izquierdo, M., & Ezzatvar, Y. (2022). Adherence to aerobic and muscle-strengthening activities guidelines: A systematic review and meta-analysis of 3.3 million participants across 32 countries. British Journal of Sports Medicine. https://doi.org/10.1136/bjsports-2022-106189.
Guthold, R., Stevens, G. A., Riley, L. M., & Bull, F. C. (2018). Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. The Lancet Global Health, 6(10), e1077–e1086. https://doi.org/10.1016/S2214-109X(18)30357-7.
de Haas, M., Kroesen, M., Chorus, C., Hoogendoorn-Lanser, S., & Hoogendoorn, S. (2021). Causal relations between body-mass-index, self-rated health and active travel: An empirical study based on longitudinal data. Journal of Transport & Health, 22, 101113. https://doi.org/10.1016/j.jth.2021.101113.
Hamer, M., & Chida, Y. (2008). Active commuting and cardiovascular risk: a meta-analytic review. Preventive Medicine, 46(1), 9–13. https://doi.org/10.1016/j.ypmed.2007.03.006.
Henriques-Neto, D., Peralta, M., Garradas, S., Pelegrini, A., Pinto, A. A., Sánchez-Miguel, P. A., & Marques, A. (2020). Active commuting and physical fitness: a systematic review. International Journal of Environmental Research and Public Health, 17(8), 2721. https://doi.org/10.3390/ijerph17082721.
Hoor, M. (2023). Public mobility and a new mobility culture: foundations, developments and paths to a cultural transport turnaround. In O. Schwedes (Ed.), Public mobility (pp. 149–175). Wiesbaden: Springer. https://doi.org/10.1007/978-3-658-39579-7_7.
Kaiser, M., Bauer, J. M., Otterbach, S., Reisch, L. A., & Sousa-Poza, A. (2023). The association between commuting and cardiovascular disease: A biomarker-based analysis of cross-sectional cohort data from the UK Biobank. Preventive Medicine, 172, 107521. https://doi.org/10.1016/j.ypmed.2023.107521.
Kalliolahti, E., Aalto, V., Salo, P., Lanki, T., Ervasti, J., & Oksanen, T. (2023). Associations between commute mode use and self-rated health and work ability among Finnish public sector employees. Scandinavian Journal of Public Health. https://doi.org/10.1177/14034948231159212.
Keyes, C. L. M. (2014). Mental health as a complete state: how the Salutogenic perspective completes the picture. In G. F. Bauer & O. Hämmig (Eds.), Bridging occupational, organizational and public health (pp. 179–192). Netherlands: Springer. https://doi.org/10.1007/978-94-007-5640-3_11.
Kroesen, M., & de Vos, J. (2020). Does active travel make people healthier, or are healthy people more inclined to travel actively? Journal of Transport & Health, 16, 100844. https://doi.org/10.1016/j.jth.2020.100844.
Lachapelle, U., Frank, L., Saelens, B. E., Sallis, J. F., & Conway, T. L. (2011). Commuting by public transit and physical activity: where you live, where you work, and how you get there. Journal of Physical Activity and Health, 8(S1), S72–S82. https://doi.org/10.1123/jpah.8.s1.s72.
Larouche, R., Faulkner, G., & Tremblay, M. S. (2016). Active travel and adults’ health: The 2007-to-2011 Canadian Health Measures Surveys. Health Reports—Statistics Canada, 27(4), 10–18.
Liao, Y., Tsai, H.-H., Wang, H.-S., Lin, C.-P., Wu, M.-C., & Chen, J.-F. (2016). Travel mode, transportation-related physical activity, and risk of overweight in Taiwanese adults. Journal of Transport & Health, 3(2), 220–225. https://doi.org/10.1016/j.jth.2016.02.012.
Lorenzo, E., Szeszulski, J., Shin, C.-N., Todd, M., & Lee, R. E. (2020). Relationship between walking for active transportation and cardiometabolic health among adults: a systematic review. Journal of Transport & Health, 19(1), 100927. https://doi.org/10.1016/j.jth.2020.100927.
Lubans, D. R., Boreham, C. A., Kelly, P., & Foster, C. E. (2011). The relationship between active travel to school and health-related fitness in children and adolescents: A systematic review. International Journal of Behavioral Nutrition and Physical Activity, 8(1), 5. https://doi.org/10.1186/1479-5868-8-5.
Maltese, I., Gatta, V., & Marcucci, E. (2021). Active travel in sustainable Urban mobility plans. An Italian overview. Research in Transportation Business & Management, 40, 100621. https://doi.org/10.1016/j.rtbm.2021.100621.
Martin, A., Goryakin, Y., & Suhrcke, M. (2014). Does active commuting improve psychological wellbeing? Longitudinal evidence from eighteen waves of the British Household Panel Survey. Preventive Medicine, 69, 296–303. https://doi.org/10.1016/j.ypmed.2014.08.023.
Masterson, A. M., & Phillips, C. M. (2022). Active commuting associations with BMI and self-related health: a cross-sectional analysis of the health ireland survey. Journal of Public Health. https://doi.org/10.1007/s10389-022-01752-w.
Mueller, N., Rojas-Rueda, D., Cole-Hunter, T., De Nazelle, A., Dons, E., Gerike, R., Götschi, T., Int Panis, L., Kahlmeier, S., & Nieuwenhuijsen, M. (2015). Health impact assessment of active transportation: a systematic review. Preventive Medicine, 76, 103–114. https://doi.org/10.1016/j.ypmed.2015.04.010.
Mytton, O. T., Panter, J., & Ogilvie, D. (2016a). Longitudinal associations of active commuting with body mass index. Preventive Medicine, 90, 1–7. https://doi.org/10.1016/j.ypmed.2016.06.014.
Mytton, O. T., Panter, J., & Ogilvie, D. (2016b). Longitudinal associations of active commuting with wellbeing and sickness absence. Preventive Medicine, 84, 19–26. https://doi.org/10.1016/j.ypmed.2015.12.010.
Mytton, O. T., Ogilvie, D., Griffin, S., Brage, S., Wareham, N., & Panter, J. (2018). Associations of active commuting with body fat and visceral adipose tissue: A cross-sectional population based study in the UK. Preventive Medicine, 106, 86–93. https://doi.org/10.1016/j.ypmed.2017.10.017.
Nigg, C., & Nigg, C. R. (2021). It’s more than climate change and active transport—Physical activity’s role in sustainable behavior. Translational Behavioral Medicine, 11(4), 945–953. https://doi.org/10.1093/tbm/ibaa129.
Østergaard, L., Jensen, M. K., Overvad, K., Tjønneland, A., & Grøntved, A. (2018). Associations between changes in cycling and all-cause mortality risk. American Journal of Preventive Medicine, 55(5), 615–623. https://doi.org/10.1016/j.amepre.2018.06.009.
Panter, J., Mytton, O., Sharp, S., Brage, S., Cummins, S., Laverty, A. A., Wijndaele, K., & Ogilvie, D. (2018). Using alternatives to the car and risk of all-cause, cardiovascular and cancer mortality. Heart, 104(21), 1749–1755. https://doi.org/10.1136/heartjnl-2017-312699.
Patterson, R., Panter, J., Vamos, E. P., Cummins, S., Millett, C., & Laverty, A. A. (2020). Associations between commute mode and cardiovascular disease, cancer, and all-cause mortality, and cancer incidence, using linked Census data over 25 years in England and Wales: A cohort study. The Lancet Planetary Health, 4(5), E186–E194. https://doi.org/10.1016/S2542-5196(20)30079-6.
Peruzzi, M., Sanasi, E., Pingitore, A., Marullo, A. G., Carnevale, R., Sciarretta, S., Sciarra, L., Frati, G., & Cavarretta, E. (2020). An overview of cycling as active transportation and as benefit for health. Minerva Cardioangiologica, 68(2), 81–97. https://doi.org/10.23736/S0026-4725.20.05182-8.
Peterman, J. E., Bassett, D. R., Harber, M. P., Whaley, M. H., Fleenor, B. S., & Kaminsky, L. A. (2021). Associations between active commuting and cardiovascular disease in the United States. Journal of Physical Activity and Health, 18(12), 1525–1531. https://doi.org/10.1123/jpah.2021-0245.
Phansikar, M., & Mullen, S. (2019). Exploring active travel and leisure-time physical activity relationships with cognition among older adults. Journal of Aging and Physical Activity, 28(4), 580–587. https://doi.org/10.1123/japa.2019-0125.
Ribeiro, P. J. G., & Fonseca, F. (2022). Students’ home-university commuting patterns: a shift towards more sustainable modes of transport. Case Studies on Transport Policy, 10(2), 954–964. https://doi.org/10.1016/j.cstp.2022.03.009.
Riiser, A., Solbraa, A., Jenum, A. K., Birkeland, K. I., & Andersen, L. B. (2018). Cycling and walking for transport and their associations with diabetes and risk factors for cardiovascular disease. Journal of Transport & Health, 11, 193–201. https://doi.org/10.1016/j.jth.2018.09.002.
Rissel, C., Curac, N., Greenaway, M., & Bauman, A. (2012). Physical activity associated with public transport use—A review and modelling of potential benefits. International Journal of Environmental Research and Public Health, 9(7), 2454–2478. https://doi.org/10.3390/ijerph9072454.
Saunders, L. E., Green, J. M., Petticrew, M. P., Steinbach, R., & Roberts, H. (2013). What are the health benefits of active travel? A systematic review of trials and cohort studies. PLoS ONE, 8(8), e69912. https://doi.org/10.1371/journal.pone.0069912.
Schauder, S. A., & Foley, M. C. (2015). The relationship between active transportation and health. Journal of Transport & Health, 2(3), 343–349. https://doi.org/10.1016/j.jth.2015.06.006.
Shepard, R. J. (2008). Is active commuting the answer to population health? Sports Medicine, 38(9), 751–758. https://doi.org/10.2165/00007256-200838090-00004.
Stigell, E., & Schantz, P. (2015). Active commuting behaviors in a nordic metropolitan setting in relation to modality, gender, and health recommendations. International Journal of Environmental Research and Public Health, 12, 15626–15648. https://doi.org/10.3390/ijerph12121.
Tamminen, N., Reinikainen, J., Appelqvist-Schmidlechner, K., Borodulin, K., Mäki-Opas, T., & Solin, P. (2020). Associations of physical activity with positive mental health: a population-based study. Mental Health and Physical Activity, 18, 100319. https://doi.org/10.1016/j.mhpa.2020.100319.
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., & Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850.
Vaara, J. P., Vasankari, T., Fogelholm, M., Koski, H., & Kyröläinen, H. (2020). Cycling but not walking to work or study is associated with physical fitness, body composition and clustered cardiometabolic risk in young men. BMJ Open Sport & Exercise Medicine, 6(1), e668. https://doi.org/10.1136/bmjsem-2019-000668.
Voulgaris, C. T., Smart, M. J., & Taylor, B. D. (2019). Tired of commuting? Relationships among journeys to school, sleep, and exercise among American teenagers. Journal of Planning Education and Research, 39(2), 142–154. https://doi.org/10.1177/0739456X17725148.
Wanjau, M. N., Dalugoda, Y., Oberai, M., Möller, H., Standen, C., Haigh, F., Milat, A., Lucas, P., & Veerman, J. L. (2023). Does active transport displace other physical activity? A systematic review of the evidence. Journal of Transport & Health, 31, 101631. https://doi.org/10.1016/j.jth.2023.101631.
Warburton, D., & Bredin, S. (2017). Health benefits of physical activity: a systematic review of current systematic reviews. Current Opinion in Cardiology, 32(5), 541–556. https://doi.org/10.1097/HCO.0000000000000437.
WHO (2020). WHO guidelines on physical activity and sedentary behaviour. World Health Organization.
Xu, H., Wen, L. M., & Rissel, C. (2013). The relationships between active transport to work or school and cardiovascular health or body weight: a systematic review. Asia Pacific Journal of Public Health, 25(4), 298–315. https://doi.org/10.1177/1010539513482965.
Zemedikun, D. T., Gray, L. J., Khunti, K., Davies, M. J., & Dhalwani, N. N. (2018). Patterns of multimorbidity in middle-aged and older adults: an analysis of the UK Biobank data. Mayo Clinic Proceedings, 93(7), 857–866. https://doi.org/10.1016/j.mayocp.2018.02.012.
Zwald, M. L., Fakhouri, T. H. I., Fryar, C. D., Whitfield, G., & Akinbami, L. J. (2018). Trends in active transportation and associations with cardiovascular disease risk factors among U.S. adults, 2007–2016. Preventive Medicine, 116, 150–156. https://doi.org/10.1016/j.ypmed.2018.09.008.
Funding
Funded by the Open Access Publishing Fund of the University of Bayreuth.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization: S. Tittlbach; methodology: S. Tittlbach, A. Brockfeld; analysis: S. Tittlbach, S. Kindig, A. Brockfeld; writing—original draft: S. Tittlbach, M. Herfet; writing—review & editing: S. Tittlbach, M. Herfet, S. Kindig, A. Brockfeld
Corresponding author
Ethics declarations
Conflict of interest
S. Tittlbach, A. Brockfeld, S. Kindig and M. Herfet declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Search terms
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tittlbach, S., Brockfeld, A., Kindig, S. et al. Maintaining health in daily life—is active travel the solution?. Ger J Exerc Sport Res 54, 121–134 (2024). https://doi.org/10.1007/s12662-023-00924-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12662-023-00924-4