
Abstract
Introduction
The numerous health benefits of physical activity (PA) for people with non-communicable diseases (NCDs) are well-documented. In Germany, there are limited data on whether adults with NCDs fulfill health-oriented PA recommendations. This study describes the prevalence of meeting PA recommendations among adults with select NCDs.
Method
Based on the national representative GEDA-2014/2015-EHIS (N = 24,016), the self-reported PA data of the European Health Interview Survey–Physical Activity Questionnaire (EHIS-PAQ) were classified with respect to fulfilling recommendations for health-enhancing aerobic activities (≥ 150 min per week with at least moderate intensity) and muscle strengthening (≥ 2 times per week). These binary indicators were used to analyze the association between the prevalence of sufficient PA and the self-reported presence of certain NCDs and multiple NCDs to reflect multimorbidity.
Results
Compared to the general adult population, sufficient aerobic PA was lower for most NCDs, with the lowest level among people with diabetes mellitus, obesity, stroke, chronic obstructive pulmonary disease (COPD), and depression. Compared to the general adult population, sufficient muscle strengthening was lower for some NCDs (diabetes mellitus, obesity, depression), but it was higher in people with musculoskeletal diseases (osteoarthritis, lower back pain). Multimorbidity was negatively associated with sufficient PA levels.
Conclusion
The study specifies the need to promote PA among adults with select NCDs to counteract insufficient levels of health-enhancing PA and to reduce the individual and societal burden of NCDs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
For several decades, non-communicable diseases (NCDs) have dominated the causes of morbidity and mortality in western countries. In Germany, the 2017 Global Burden of Disease Report estimated that about 90% of mortality and disability-adjusted life years (DALY; i.e., years of life without health impairment) can be attributed to NCDs (Institute for Health Metrics and Evaluation, 2020). NCDs are distinguished from communicable infectious diseases and are characterized by their chronic, long-lasting nature (WHO, 2014). Of particular importance for the NCD-related burden of disease in the German population are cardiovascular diseases (CVDs; 18.9% of DALY, including ischemic heart diseases [9.3%] and stroke [4.0%]), cancer (18.8%), musculoskeletal diseases (11.3%; including low back pain [6.6%] and neck pain [2.3%]), neurological diseases (8.4%), mental disorders (6.5%; including depression [2.2%]), chronic obstructive pulmonary disease (COPD; 3.9%), and metabolic diseases like diabetes mellitus (2.9%).
For a multitude of NCDs, it is now well documented that physical activity (PA) has both preventive and therapeutic health effects. The most recent report of the Physical Activity Guidelines Advisory Committee (PAGAC, 2018) provides moderate to strong evidence that PA reduces the risk of developing various cardiovascular, metabolic, and neurological diseases and mental disorders as well as certain types of cancer. For people who are already affected by NCDs, many positive health effects of PA related to disease progression, symptoms, and the risk of morbidity and mortality are also empirically well-documented (Pedersen & Saltin, 2015; PAGAC, 2018). Moreover, depending on the health disorder, PA positively influences important risk factors for the chronicity of NCDs (e.g., obesity, high blood pressure), impaired body functions, and pain experiences (Pedersen & Saltin, 2015).
Based on this growing evidence, PA recommendations have been developed and updated since the 1980s, which describe a minimum level of PA required to achieve the health benefits (WHO, 2010). Such recommendations do also exist for people with NCDs for Germany (Geidl, Abu-Omar, Weege, Messing, & Pfeifer, 2020; Pfeifer & Geidl, 2017) and are comparable with national and international recommendations for the general adult population (Füzéki, Vogt, & Banzer, 2017; Rütten & Pfeifer, 2017; WHO, 2010). In terms of aerobic activities, a weekly minimum of 150 min of activity with moderate intensity, 75 min of activity with vigorous intensity, or a combination of these, is recommended. In addition, muscle strengthening is also advised at least twice a week. Indeed, the fulfillment of both recommendations for aerobic activity and muscle strengthening is associated with high risk reductions for all-cause and cause-specific mortality (Zhao, Veeranki, Magnussen, & Xi, 2020).
In Germany, however, the potential health benefits are not fully utilized due to PA levels that are insufficient to meet the current health-oriented PA recommendations (Finger, Mensink, Lange, & Manz, 2017). According to the findings of the nationwide representative German Health Update (GEDA-2014/2015-EHIS) in the general adult population, only 42.6% of women and 48.0% of men meet the recommendations for at least 150 min of moderate aerobic activity each week. For muscle strengthening, the percentages of adults who perform this type of PA at least twice a week are even lower at 27.6% in women and 31.2% in men (Finger et al., 2017).
Large international studies have indicated that PA may be significantly reduced in the subpopulation of people with NCDs. A study in the United States, for example, observed that more than the half of the individuals with no NCDs (~ 54%) met the recommended minimum of 150 min of at least moderate aerobic activity weekly. However, the prevalence of sufficient aerobic PA was lower for people with cancer and osteoarthritis (both ~ 45%) and was the lowest for people with stroke (~ 31%) and COPD (~ 26%) (Brawner, Churilla, & Keteyian, 2016). A further large epidemiological study in the United Kingdom also confirmed these findings that people with NCD were significantly less active, and trends between different types of diseases were again observed (Barker et al., 2019).
In Germany, no nationwide representative information regarding PA behavior in people who have NCDs is available to date. However, such knowledge is necessary to more precisely assess the potential need for action to promote PA and also to create a better source of information for targeted interventions for the vulnerable subpopulation of people with NCDs. Therefore, the aim of this study was to characterize patterns of prevalence for fulfilling health-oriented PA recommendations in people with NCDs using a nationally representative survey of the German Health Update (GEDA-2014/2015-EHIS; Lange et al., 2017). The main questions were whether the PA behavior of adults with NCDs differs from that of the general adult population and whether, on average, there are differences in people with a certain NCD. It also includes the question whether people with multiple NCDs, as international studies have shown (Brawner et al., 2016), are particularly vulnerable to not achieving the PA recommendations.
Methods
This study report is written in accordance with the guidelines for reporting observational studies (STROBE Statement, von Elm et al., 2008). The checklist of items for cross-sectional studies is included in the Supplementary Material.
Design and sample
We used the Scientific Use File of the GEDA 2014/2015-EHIS from the Robert Koch Institute (2018). The GEDA 2014/2015-EHIS is a health survey that was conducted among adults as part of the Federal Health Monitoring System in Germany (Lange et al., 2017; Saß et al., 2017). The survey was based on self-administered questionnaires delivered either electronically via the internet or as a paper questionnaire sent by postal mail. The data collection was carried out from November 2014 through July 2015.
A detailed description of the sampling and response rates can be found in the original study description by Lange et al. (2017). In brief, it was a nationally representative sample of adults aged 18 years or older. The sample was assembled with a two-stage cluster sampling approach: First, 301 communities were randomly selected (stratified by region and community size). Second, people with permanent residence in the communities were randomly chosen from the local population registers. A total of 24,016 people (10,872 men and 13,144 women) participated in the voluntary survey (44.6% via the web, 55.4% via paper surveys that were mailed). Written informed consent was obtained from all participants after they had been informed about the study objectives and contents, as well as the data protection regulations according to the approved study protocol. The response rate was 26.9%, which was within the typically expected low range for population-based health surveys (Saß et al., 2017).
Measures
Physical activity
In the GEDA-2014/2015-EHIS, the European Health Interview Survey-Physical Activity Questionnaire (EHIS-PAQ) was applied for the first time to estimate PA levels within the federal health monitoring surveys. The EHIS-PAQ is a short survey instrument used to assess PA in different domains relevant to public health (work, transportation, and leisure time). An important goal in the development of the questionnaire was to enable survey-based estimates of the proportion of the population that meets current health-oriented PA recommendations (Finger et al., 2015). Therefore, the area of leisure-time PA contained questions on both aerobic activities and muscle strengthening. The first question in this section asked about sports, fitness, and recreational activities that lead to at least a slight increase in breathing and heart rate (e.g., [nordic] walking, ball games, jogging, cycling, swimming, aerobics, rowing, or badminton). The respondents indicated how many days in a typical week they were active for at least 10 min and how much time they spent on these activities per week in their leisure time. This assessment was in line with the definition of aerobic activities with at least a moderate intensity used for the PA recommendation of the WHO (2010). Due to negative experiences in piloting the EHIS-PAQ, no further differentiation was made between moderate and vigorous aerobic activities (Finger et al., 2015). For muscle strengthening, the frequency in a typical week was asked for, and examples were given, including strength training or strengthening exercises performed using weights, elastic bands, or one’s own body weight.
To assess transportation-related PA, the EHIS-PAQ contains two questions each on walking and cycling. The first question asked about the number of days in a typical week that people walked or cycled for transportation purposes. The second question assessed how long people walked or cycled on a typical day. This method allowed the estimation of the duration of walking and cycling for transportation for at least 10 min at a time in a typical week.
Based on this information, we used the three main indicators of the federal health monitoring system as follows:
-
Health-enhancing aerobic activity: This binary indicator describes whether people engage in at least 150 min of aerobic activity in bouts of 10 min or more each week using information on cycling for transportation as well as on time spent participating in sports, fitness, and recreational activities with at least a moderate intensity.
-
Muscle strengthening: This binary indicator describes the fulfillment of recommendations for at least two sessions of muscle-strengthening activities per week.
These indicators have demonstrated an acceptable validity and reliability in previous validation studies (Baumeister et al., 2016; Finger et al., 2015) and have already been used in publications that employed the EHIS-PAQ for health-monitoring purposes (Finger et al., 2017) or research (Finger et al., 2019). In addition, we considered a third indicator by referring to the fulfillment of both recommendations on health-enhancing aerobic activity and muscle strengthening (Finger et al., 2017).
For the purpose of our sensitivity analyses, we also used the indicator for health-enhancing aerobic activity, which includes information on transportation-related walking. Because transportation-related walking might not reflect activity with at least a moderate intensity, the weekly duration was multiplied by 0.5 (Baumeister et al., 2016; Finger et al., 2015).
Non-communicable diseases
The selection of noncommunicable diseases (NCDs) for this study (Table 1) was mainly based on the listing of the 10 most important causes of the burden of disease in adult men or women in Germany (Plass et al., 2014). In addition, obesity was considered as a major risk factor for various NCDs (WHO, 2014). The survey questionnaire (Journal of Health Monitoring, 1/2017, Supplement) contained further NCDs (e.g., allergies, kidney disease), but these were not included in any analyses of the present study.
Participants were asked to self-report whether they had experienced any diseases or health problems in the last 12 months (12-month prevalence). For this purpose, a list of diseases and health problems was queried. In the present analyses, the definitions of indicators for NCDs were used wherever possible, as they are also used by the Robert Koch Institute for reporting the 12-month prevalence. In this case, appropriate references are provided in Table 1; otherwise, we refer to the specific wording in the applied list of diseases and health problems. In addition, further self-report measures were used to classify obesity and depressive symptoms (Table 1).
In order to capture multimorbidity, we calculated the sum of the NCDs that affected the participants. For this purpose, low back pain and neck pain were combined into one to achieve greater differentiation between the accumulated NCDs. The sum score for the NCDs under study could therefore range from 0–9.
Sociodemographic variables
To consider potential confounders of the associations between NCDs and PA levels, the main analyses included age, sex, education level, and socioeconomic status (SES) as covariates. These sociodemographic variables are known to be associated with the prevalence of NCDs (see also Table 1), the prevalence of sufficient PA levels (e.g., Finger et al., 2017; Abu-Omar et al., in print), or with both. To classify these characteristics, we used data on participants’ sex (male or female) and age group (18–29 years, 30–44 years, 45–64 years, and 65 years or older), as well as categories based on those in the International Standard Classification of Education (ISCED) to characterize the education level of participants. A three-part distinction between a low, medium, and high education level was made (see Lange et al., 2017). Similarly, the SES distinguished between the three categories of low, medium, and high SES. The SES indicator was based on education, income, and occupational status (see Lampert, Kroll, Lippe, von der Müters, & Stolzenberg, 2013). For both variables, the lower category corresponded to the bottom quintile, while the upper category included the top quintile.
Statistical analyses
The statistical analyses were conducted using the complex samples module of the Statistical Package for the Social Sciences (SPSS, version 25, IBM, Armonk, NY, USA). This approach allowed us to account for the cluster design of the multi-stage sampling procedure. Further, a weighting factor was applied to correct deviations of the realized sample from the population structure (Lange et al., 2017). In concrete terms, the sample composition was adjusted to the official German population statistics (as of 31 December 2014) with regard to sex, age, region, and education.
The NCD-specific prevalence rates for fulfilling of PA recommendations were derived using general linear modeling, in which adjusted estimates were calculated separately for each NCD. For the adjustment, we used the four sociodemographic variables described above (sex, age group, education level, and SES). For descriptive purposes, we compared NCD-specific prevalence rates with data on PA prevalence in the general adult population taken directly from the GEDA-2014/2015-EHIS main reports (Finger et al., 2017). Accordingly, this data from the general adult population (reference population) referred to the total survey sample, including adults with and without NCDs. Substantial differences between the NCD-specific prevalence rates and the prevalence in the reference population were described when the 95% confidence intervals (CIs) did not overlap.
To test the differences between people with and without each NCD, separate logistic regression analyses were conducted for each combination of the various binary NCD indicator (NCD reported vs. not reported) and the binary PA indicator (recommendation fulfilled vs. not fulfilled). Therefore, for the main analyses, we calculated 10 (each NCD served as a single independent variable) × 3 (each PA indicator served as dependent variable) regression analyses in all. In each analysis, the four sociodemographic variables served as covariates in order to control their potential confounding effects on the association between NCDs and PA levels. By doing this, we determined the multivariable adjusted odds ratios (ORs) and the 95% CIs for the binary dependent variables regarding fulfillment of PA recommendations. If the 95% CIs of the ORs did not include the value 1, a statistically significant difference was assumed.
An estimate of the PA prevalence rates depending on multimorbidities was also derived using general linear modelling. The prevalence estimates were calculated for six categories using the number of self-reported NCDs (0, 1, 2, 3, 4, ≥ 5) while controlling for the four sociodemographic variables: sex, age group, education level, and SES. For all the analyses, the participants were included if no data were missing for them for the respective analysis (complete case analysis).
Results
Sample descriptions
Table 1 provides sociodemographic information on the total sample (general adult population) and detailed information on the participants who reported having a certain NCD (cases). The highest prevalence was observed for low back pain and neck pain, while stroke was the least reported NCD. Most NCDs were almost equally distributed between men and women. As expected, there were comparatively large age differences for different NCDs.
Prevalence of sufficient PA in people with NCDs
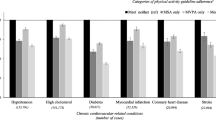
Table 2 summarizes the adjusted prevalence of the different PA indicators among participants who reported having one or more NCD. Compared to the general adult population in Germany, the prevalence of at least 150 min of moderate aerobic activity per week was lower among participants with NCDs for almost all NCDs. The lowest values were observed for depressive symptoms (32.7% [95% CI 30.2–35.2%]), COPD (33.0% [95% CI 29.9–36.1%]), obesity (33.4% [95% CI 31.6–37.6%]), stroke (34.0% [95% CI 27.8–40.1%]), and diabetes mellitus (34.6% [31.6–37.6%]). In contrast, there were no substantial differences from the general adult population in both people with cancer and with osteoarthritis.
The logistic regression analyses (Fig. 1) that controlled for sex, age group, education level, and SES showed a comparable picture for reporting at least 150 min of aerobic activity per week. While there were no differences between participants with cancer and those with osteoarthritis compared to participants without these NCDs, the recommendations were reached less frequently by participants having one of the other NCDs under study. The strongest associations were again found for depressive symptoms (ORadj. = 0.53 [0.47–0.60]), obesity (ORadj. = 0.54 [0.49–0.59]), COPD (ORadj. = 0.56 [0.48–0.65]), stroke (ORadj.= 0.59 [0.43–0.80]), and diabetes mellitus (ORadj. = 0.61 [0.53–0.70]).

Forest plots for multivariate adjusted odds ratios (OR; adjusted for sex, age group, educational level and socioeconomic status [SES]) and 95% confidence intervals (CI) for the fulfilment of recommendations for a health-enhancing aerobic activity (at least 150 min per week) and b muscle strengthening (at least 2 times per week) for different NCDs (reference category: certain NCD not reported). COPD chronic obstructive pulmonary disease
The prevalence of muscle strengthening at least twice a week in people with NCDs was generally less deviated from the reference population (Table 2). The lowest adjusted values were observed in people with obesity (21.7% [20.1–23.3%]), diabetes mellitus (22.6% [20.1–25.1%]), and depressive symptoms (24.4% [22.3–26.5%]). In contrast, a sufficient frequency of muscle strengthening was reported by people with osteoarthritis and was more frequent than that reported in the general adult population (34.8% [32.8–36.8%]). Logistic regression analyses (Fig. 1) revealed a significantly higher probability for the fulfillment of the recommendations for muscle strengthening by people with osteoarthritis (ORadj. = 1.34 [95% CI 1.21–1.48]) and also for people with low back pain (ORadj. = 1.09 [95% CI 1.02–1.17]). Similarly, the logistic regressions confirmed that the recommendations for muscle strengthening were less frequently reached by people with obesity (ORadj. = 0.58 [0.52–0.64]), diabetes mellitus (ORadj. = 0.65 [0.56–0.76]), and depressive symptoms (ORadj. = 0.72 [0.63–0.81]).
Combining both indicators for aerobic activity and muscle strengthening reinforced the lower fulfillment of PA recommendations for people with obesity (14.8% [13.5–16.1%]), depressive symptoms (16.5% [14.5–18.5%]), and diabetes mellitus (16.2% [14.0–18.3%]) compared to the general adult population. In contrast, people with osteoarthritis (26.1% [24.2–28.0%]) reported fulfilling both elements of PA recommendations more often than the general adult population (Table 2).
During the sensitivity analyses, similar associations were observed for both indicators of health-enhancing aerobic activity. The logistic regression analyses provided comparable results when the indicator for health-enhancing aerobic activity, including transportation-related walking, was used as a dependent variable (Supplementary Table 3 and Supplementary Fig. 1). Therefore, the findings can be viewed regardless of whether transportation-related walking was included as an aerobic activity.
Prevalence of fulfilling PA recommendations depending on multimorbidity
One-third of the participants reported either no (34.4%) or just one (34.8%) of the NCDs under study (Supplementary Table 4). About 18% reported two NCDs, and the remaining 13% reported three or more NCDs. The adjusted prevalence for fulfilling the recommendations for health-enhancing aerobic activity was lower for people who had multimorbidities (Fig. 2). In particular, when respondents reported three or more NCDs, the rate of reaching the recommended level of aerobic activity decrease substantially. The small group of people who reported five or more NCDs had the lowest rates, approximately 25% lower than people who reported none of the studied NCDs. In comparison, the differences for the muscle-strengthening recommendations were less pronounced. Only the group that reported five or more NCDs had rates of fulfilling these recommendations that were substantially lower than those who had none of the studied NCDs (∆ 8.2%).

Multivariate adjusted prevalence of adults who fulfill physical activity (PA) recommendations for health-enhancing aerobic activity and muscle strengthening depending on the number of reported non-communicable diseases (adjusted for sex, age groups education level and socioeconomic status; bars represent 95% confidence intervals of the estimated prevalence)
Discussion
The present study explored the role of people who had NCDs with respect to high rates of physical inactivity. In this regard, it provided the first findings on the rates at which people who have NCDs met health-oriented PA recommendations in Germany. Our results demonstrated that nearly all subgroups of people who have NCDs met the PA recommendations less frequently than did the general adult population. While it is largely accurate to state that NCDs are associated with insufficient PA, the association should not be over-generalized. Depending on the specific NCD and the type of activity, substantial differences were observed.
Specifying the need for promoting PA among people who have NCDs
The findings support the expert opinions reported in a Delphi consensus study that found a great need for target group-oriented strategies of PA promotion, such as in people having chronic diseases (Gohres & Kolip, 2017). To specify what actions are needed to promote PA among people who have NCDs, it is necessary to more closely examine the differences in prevalence rates by NCDs and type of activity.
Our analyses found that the presence of NCDs was associated with a lower probability of fulfilling PA recommendations. This association was more pronounced for aerobic activity than for muscle strengthening. Insufficient aerobic activity was particularly observed when people reported the presence of obesity, COPD, stroke, diabetes mellitus or depressive symptoms. Furthermore, respondents with cardiovascular diseases as well as back and neck pain also reported a lower prevalence of sufficient aerobic PA. These results are to a large extent comparable with the representative studies already available from the US (Brawner et al., 2016) and the UK (Barker et al., 2019), which have focused on the recommendations for aerobic PA. In fact, the order of prevalence estimates was almost identical for the seven NCDs explored both in this study and in the US study (with decreasing prevalence in cancer, osteoarthritis, CHD, diabetes mellitus, obesity, stroke, and COPD); estimates of prevalence were also similar.
Beyond the lower levels of aerobic PA in people with NCDs, four observations were remarkable. First, people with obesity, diabetes mellitus, or depressive symptoms reported not only the lowest levels of aerobic PA, but also lower rates of fulfilling the recommendations for muscle strengthening. Therefore, these subgroups are at a particularly high risk of inactivity across various activity types. This is important because meeting both recommendations is associated with greater reductions in the risk of mortality than meeting the recommendation for either aerobic activity or muscle strengthening alone (Zhao et al., 2020). Second, the number of NCDs present simultaneously was clearly associated with meeting the recommendations for aerobic PA, a finding that is in line with international data (Brawner et al., 2016). Given the increasing importance of multimorbidities to the German healthcare sector (Puth, Weckbecker, Schmid, & Münster, 2017), PA promotion strategies should focus on people who have multimorbidities. Third, and somewhat unexpectedly, people who had certain NCDs were more likely to meet the recommendations for muscle strengthening. This is particularly striking in the case of musculoskeletal disorders, for which disease-specific recommendations for muscle strengthening have been established (e.g., Fernandes et al., 2013). Fourth, in people who reported osteoarthritis and cancer, the levels of aerobic PA did not differ from the average for Germany’s adult population. This last finding is in line with the results of another recent German study showing that slightly more than half of those diagnosed with cancer reported meeting the recommendations for aerobic activity (Steindorf et al., 2020).
Our findings can be used as a data source when identifying subgroups particularly vulnerable to physical inactivity. Our analyses of subgroups having different NCDs controlled for sociodemographic characteristics in order to minimize the potential alternative explanations for the differences in PA levels among NCDs. However, differences in PA levels across various NCDs are certainly not attributable per se to the health disorder alone. According to the biopsychosocial health framework of the International Classification of Functioning, Disability, and Health (ICF; WHO, 2001) the effects of health disorders on physical activities greatly depend on various personal and environmental factors regarding the people who have NCDs. That means that individuals deal with health disorders based on the availability of physical and mental resources (e.g., knowledge, physical fitness, motivation regarding PA, and degree of coping with kinesiophobia) in conjunction with social and structural conditions (e.g., social support, availability of adapted PA) (Geidl, Semrau, & Pfeifer, 2014).
Against this background, our findings may encourage further studies seeking to explain the differences in PA behavior among those who have different NCDs, as the cross-sectional study design used provided only limited data on this point. Bearing this in mind, our study’s results indicate that, on average, a certain proportion of insufficient PA in those who have NCDs might be caused by the health disorder itself and its associated symptoms related to body functions. This statement is supported by various reviews and studies of barriers to and facilitators of PA behavior, which have shown that limitations in physical functioning or due to pain caused by diseases like stroke (Jackson, Mercer, & Singer, 2018; Nicholson et al., 2017), CVD (Stewart et al., 2013), osteoarthritis (Kanavaki et al., 2017), back pain (Boutevillain, Dupeyron, Rouch, Richard, & Coudeyre, 2017), or COPD (Thorpe, Johnston, & Kumar, 2012) are significant barriers to sufficient PA. In addition, one could argue that the pronounced physical inactivity of people who have depressive symptoms might be associated with the symptomatology of this mental disorder. Therefore, the general symptoms of depression, including lack of motivation or energy, may be directly related to limitations in physical activities (Glowacki, Duncan, Gainforth, & Faulkner, 2017).
Besides these symptom-related barriers to PA, future research should elaborate more on personal and environmental factors that could further explain the differences among the various NCDs. For example, regarding personal motivation to exercise, a nation-wide survey in German rehabilitation settings found that exercise therapists perceived substantial differences depending on the diseases and health problems they treated (Deprins, Geidl, Streber, Pfeifer, & Sudeck, 2019). In accordance with our findings, exercise therapists reported that patients in oncological rehabilitation programs had the lowest barriers to motivation for PA and the highest enjoyment of PA. In contrast, patients in rehabilitation programs for diabetes mellitus were perceived as having outstandingly high barriers to PA and low levels of concrete ideas regarding incorporating PA into their everyday lives (Deprins et al., 2019). Further elucidation of such disease-specific differences can enable targeted interventions to promote PA in those having a specific NCD.
In terms of environmental factors, our findings merit further investigation into the role of disease-specific PA recommendations for people who have NCDs. We noted that people who had muscular-skeletal diseases (i.e., osteoarthritis and low back pain) more often reported fulfilling the muscle strengthening recommendations. Regarding promoting PA, we can cautiously conclude that disease-specific PA recommendations may be mirrored in the PA behaviors of certain subpopulations. Therefore, it is interesting to note that, for the first time, current WHO recommendations for health-oriented PA (Bull et al., 2020), specifically address people with chronic diseases, as Germany’s national PA recommendations already do (Pfeifer & Geidl, 2017). However, further clarification is required regarding, for example, how disease-specific recommendations are related to personal motivation, how they are integrated into medical advice or how they enhance the availability of exercise programs for people with NCDs (e.g., as part of disease-management programs or health-oriented offers by sports organizations). This latter point is likely to vary considerably among the NCDs, which may also contribute to the differences in prevalence rates depending on the NCD and the type of activity. Further clarification of this point will require research that appropriately considers environmental and policy-related determinants of PA at the national, regional, and local levels in Germany (e.g. Bauman et al., 2012).
Finally, various disease-specific reviews have illustrated that comorbidities represent a barrier to sufficient PA for people with NCDs (e.g., Kanavaki et al., 2017; Stewart et al., 2013); this conclusion was generally supported by the present findings regarding multimorbidity. In addition to the higher physical limitations that impair PA in the presence of multiple NCDs (Newsom et al., 2012; Stewart et al., 2013), increased attention must be paid to any accompanying depressive symptoms. For example, depressive symptoms have been identified as an additional PA barrier in people with obesity (Adachi-Mejia & Schifferdecker, 2016) and neck pain (Dimitriadis, Kapreli, Strimpakos, & Oldham, 2017). For future research, it would therefore be interesting to further analyze the specific patterns of multimorbidity (e.g., metabolic syndrome, depressive comorbidities) with regard to physical inactivity.
Strengths and limitations
The use of the Scientific Use File of the GEDA-2014/2015-EHIS enabled us to generate information on the PA levels of people with different NCDs in Germany on the basis of a nationally representative dataset. The application of the EHIS-PAQ allowed the explicit consideration of different elements of PA recommendations for both aerobic activities and muscle strengthening. For the indicators used, validation studies revealed that they allow the estimation of compliance with PA recommendations and have sufficient validity for use in surveillance studies and also to inform public policy (Baumeister et al., 2016; Finger et al., 2015). Nevertheless, the general limitations for self-report PA measurements (e.g., social desirability, overreporting, and recognition bias) and possible sources of misclassification specific to the questionnaire should be discussed for the EHIS-PAQ.
First, the indicator for health-oriented aerobic activity focuses on meeting the recommendations for at least 150 min of weekly aerobic activity of at least moderate intensity. Thus, an underestimation of the prevalence of achieving aerobic activity recommendations can occur when people complete a minimum of 75 min of vigorous aerobic activity or an equivalent combination of moderate and vigorous activity. Second, for the aerobic PA indicator only, cycling was considered regarding the domain of transportation-related PA. Validation studies of the EHIS-PAQ, which used accelerometer measurements, have pointed to the added value of the combined consideration of leisure-time PA and transportation-related PA (Baumeister et al., 2016). However, an overestimation of health-enhancing aerobic activity could result, as all cycling is considered to be at least of moderate intensity. In contrast, the prevalence of sufficient aerobic PA could be underestimated, as transportation-related walking with a potentially moderate intensity was not included in the main analyses. The sensitivity analyses have shown, however, that although the prevalence estimates were about 7–15% higher when transportation-related walking was included (Supplementary Table 3); this difference had no significant influence on answering the main questions of our study. Third, the indicator for muscle strengthening estimates the prevalence for fulfilling health-oriented recommendations based only on a weekly frequency. However, PA recommendations usually advise that all major muscle groups should be trained (WHO, 2010). The fact that such information was not assessed is likely to lead to an overestimation of sufficient levels of muscle strengthening.
The limitation of self-reports also applies to the assessment of NCDs. With respect to body mass index-based classifications of obesity, for instance, relevant deviations of self-reported height and weight compared to anthropometric measurements may occur (Nyholm et al., 2007). Furthermore, no differentiation between type 1 and type 2 diabetes mellitus was possible. Likewise, this study was unable to distinguish between different types of cancer. As a result, we could not account for the fulfillment of PA recommendations that may vary according to the type of cancer (Steindorf et al., 2020).
Moreover, the response rate of only 26.9% in the GEDA-2014/2015-EHIS has to be considered. It cannot be ruled out that physically active people were more likely to participate in the survey than inactive people, which would lead to a general overestimation of the PA prevalence.
Conclusion
The study has shown that people affected by one of the studied NCDs largely have a lower likelihood for sufficient PA. However, the presence of a medical diagnosis and physical limitations alone do not determine low PA levels. Rather, all phenomena from the increase and maintenance to the reduction of previous PA levels appear after the onset of health disorders (Gropper, John, Sudeck, & Thiel, 2020). To promote PA in people who have NCDs, it is therefore essential to foster PA-related health competences that enable the individual to realize and structure the PA in a way that is beneficial given the existing health disorder (Sudeck & Pfeifer, 2016; Carl, Sudeck, & Pfeifer, 2020). At the same time, organizational, environmental, and policy-related conditions of PA must be optimized to improve the opportunities for PA and their accessibility in this vulnerable subpopulation, especially in the community and the healthcare system. The Global Action Plan on Physical Activity 2018–2030 (WHO, 2018) outlines various strategies for this integration of individual- and environmental-oriented measures of PA promotion. In view of the present study results, these strategies should be implemented to a greater extent to counteract insufficient health-oriented PA of people who have NCDs.
References
Abu-Omar, K., Messing, S., Sarshar, M., Gelius, P., Ferschl, S., Finger, J.D., Bauman, A. (in print). Sociodemographic correlates of physical activity and sport among adults in Germany: 1997–2018. German Journal of Exercise and Sport Research.
Adachi-Mejia, A. M., & Schifferdecker, K. E. (2016). A mixed-methods approach to assessing barriers to physical activity among women with class I, class II, and class III obesity. Public Health, 139, 212–215.
Barker, J., Smith Byrne, K., Doherty, A., Foster, C., Rahimi, K., Ramakrishnan, R., Dwyer, T., et al. (2019). Physical activity of UK adults with chronic disease: cross-sectional analysis of accelerometer-measured physical activity in 96 706 UK Biobank participants. International Journal of Epidemiology, 48(4), 1167–1174.
Bauman, A.E., Reis, R.S., Sallis, J.F., Wells, J.C., Loos, R.J.F., Martin, B.W. et al. (2012). Correlates of physical activity: why are some people physically active and others not? Lancet, 380, 258–271.
Baumeister, S. E., Ricci, C., Kohler, S., Fischer, B., Töpfer, C., Finger, J. D., & Leitzmann, M. F. (2016). Physical activity surveillance in the European Union: reliability and validity of the European Health Interview Survey-Physical Activity Questionnaire (EHIS-PAQ). The International Journal of Behavioral Nutrition and Physical Activity, 13, 61.
Boutevillain, L., Dupeyron, A., Rouch, C., Richard, E., & Coudeyre, E. (2017). Facilitators and barriers to physical activity in people with chronic low back pain: A qualitative study. PLOS One, 12(7), e179826.
Brawner, C. A., Churilla, J. R., & Keteyian, S. J. (2016). Prevalence of physical activity is lower among individuals with chronic disease. Medicine and Science in Sports and Exercise, 48(6), 1062–1067.
Bretschneider, J., Kuhnert, R., & Hapke, U. (2017). Depressive Symptomatik bei Erwachsenen in Deutschland. Journal of Health Monitoring, 2(3), 81–88.
Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., Willumsen, J. F., et al. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine, 54, 1451–1462.
Busch, M. A., & Kuhnert, R. (2017a). 12-Monats-Prävalenz einer koronaren Herzkrankheit in Deutschland. Journal of Health Monitoring, 2(1), 64–69.
Busch, M. A., & Kuhnert, R. (2017b). 12-Monats-Prävalenz von Schlag anfall oder chronischen Beschwerden infolge eines Schlaganfalls in Deutschland. Journal of Health Monitoring, 2(1), 70–76.
Carl, J., Sudeck, G., & Pfeifer, K. (2020). Competencies for a healthy physically active lifestyle—Reflections on the Model of Physical Activity-related Health Competence (PAHCO). Journal of Physical Activity and Health, 17, 688–697.
Deprins, J., Geidl, W., Streber, R., Pfeifer, K., & Sudeck, G. (2019). Konzeptionelle Grundlagen der Bewegungstherapie in der medizinischen Rehabilitation. Rehabilitation, 58(6), 366–375.
Dimitriadis, Z., Kapreli, E., Strimpakos, N., & Oldham, J. (2017). The association between the physical activity of patients with idiopathic chronic neck pain and their psychological state. Archives of Hellenic Medicine, 34(1), 100–103.
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., & Vandenbroucke, J. P. (2008). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Journal of Clinical Epidemiology, 61, 344–349.
Fernandes, L., Hagen, K. B., Bijlsma, J. W., Andreassen, O., Christensen, P., Conaghan, P. G., Vliet Vlieland, T. P., et al. (2013). EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Annals of the Rheumatic Diseases, 72, 1125–1135.
Finger, J. D., Tafforeau, J., Gisle, L., Oja, L., Ziese, T., Thelen, J., Lange, C., et al. (2015). Development of the European Health Interview Survey—Physical Activity Questionnaire (EHIS-PAQ) to monitor physical activity in the European Union. Archives of Public Health, 73, 59.
Finger, J. D., Varnaccia, G., Gabrys, L., Hoebel, J., Kroll, L. E., Krug, S., Leitzmann, M. F., et al. (2019). Area-level and individual correlates of active transportation among adults in Germany: A population-based multilevel study. Scientific Reports, 9, 16361.
Finger, J. D., Mensink, G. B. M., Lange, C., & Manz, K. (2017). Gesundheitsfördernde körperliche Aktivität in der Freizeit bei Erwachsenen in Deutschland. Journal of Health Monitoring, 2(1), 83–90.
Fuchs, J., Kuhnert, R., & Scheidt-Nave, C. (2017). 12-Monats-Prävalenz von Arthrose in Deutschland. Journal of Health Monitoring, 2(3), 55–60.
Füzéki, E., Vogt, L., & Banzer, W. (2017). Nationale Bewegungsempfehlungen für Erwachsene und ältere Erwachsene – Methodisches Vorgehen, Datenbasis und Begründung. Das Gesundheitswesen, 79(1), 20–28.
Geidl, W., Abu-Omar, K., Weege, M., Messing, S., & Pfeifer, K. (2020). German recommendations for physical activity and physical activity promotion in adults with noncommunicable diseases. The International Journal of Behavioral Nutrition and Physical Activity, 17(1), 12.
Geidl, W., Semrau, J., & Pfeifer, K. (2014). Health behaviour change theories: contributions to an ICF-based behavioural exercise therapy for individuals with chronic diseases. Disability & Rehabilitation, 36, 2091–2100.
Glowacki, K., Duncan, M. J., Gainforth, H., & Faulkner, G. (2017). Barriers and facilitators to physical activity and exercise among adults with depression: A scoping review. Mental Health and Physical Activity, 13, 108–119.
Gohres, H., & Kolip, P. (2017). Strukturen der Bewegungsförderung in Deutschland. Prävention und Gesundheitsförderung, 12, 203–210.
Gropper, H., John, J. M., Sudeck, G., & Thiel, A. (2020). The impact of life events and transitions on physical activity: a scoping review. PLOS One, 15(6), e234794.
Heidemann, C., Kuhnert, R., Born, S., & Scheidt-Nave, C. (2017). 12-Monats-Prävalenz des bekannten Diabetes mellitus in Deutschland. Journal of Health Monitoring, 2(1), 48–56.
Institute for Health Metrics and Evaluation (IHME) (2020). GBD Compare Data Visualization. Seattle, WA: IHME, Universatiy of Washington. https://vizhub.healthdata.org/gbd-compare/. Accessed August 2, 2020
Jackson, S., Mercer, C., & Singer, B. J. (2018). An exploration of factors influencing physical activity levels amongst a cohort of people living in the community after stroke in the south of England. Disability and Rehabilitation, 40(4), 414–424.
Kanavaki, A. M., Rushton, A., Efstathiou, N., Alrushud, A., Klocke, R., Abhishek, A., & Duda, J. L. (2017). Barriers and facilitators of physical activity in knee and hip osteoarthritis: a systematic review of qualitative evidence. BMJ Open, 7(12), e17042.
Kroenke, K., Strine, T. W., Spitzer, R. L., Williams, J. B. W., Berry, J. T., & Mokdad, A. H. (2009). The PHQ‑8 as a measure of current depression in the general population. Journal of Affective Disorders, 114, 163–173.
Lampert, T., Kroll, L. E., Lippe, E., von der Müters, S., & Stolzenberg, H. (2013). Sozioökonomischer Status und Gesundheit: Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz, 56, 814–821.
Lange, C., Finger, J. D., Allen, J., Born, S., Hoebel, J., Kuhnert, R., Ziese, T., et al. (2017). Implementation of the European health interview survey (EHIS) into the German health update (GEDA). Archives of public health, 75, 40.
Newsom, J. T., Huguet, N., McCarthy, M. J., Ramage-Morin, P., Kaplan, M. S., Bernier, J., Oderkirk, J., et al. (2012). Health behavior change following chronic illness in middle and later life. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 67(3), 279–288.
Nicholson, S. L., Greig, C. A., Sniehotta, F., Johnston, M., Lewis, S. J., McMurdo, M. E., Mead, E., et al. (2017). Quantitative data analysis of perceived barriers and motivators to physical activity in stroke survivors. The Journal of the Royal College of Physicians of Edinburgh, 47(3), 231–236.
Nyholm, M., Gullberg, B., Merlo, J., Lundqvist-Persson, C., Rastam, L., & Lindblad, U. (2007). The validity of obesity based on self-reported weight and height: implications for population studies. Obesity, 15, 197–208.
Pedersen, B. K., & Saltin, B. (2015). Exercise as medicine—evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian Journal of Medicine & Science in Sports, 25(Suppl 3), 1–72.
Pfeifer, K., & Geidl, W. (2017). Bewegungsempfehlungen für Erwachsene mit einer chronischen Erkrankung – Methodisches Vorgehen, Datenbasis und Begründung. Das Gesundheitswesen, 79(1), 29–35.
Physical Activity Guidelines Advisory Committee (PAGAC) (2018). 2018 physical activity guidelines advisory committee scientific report. Washington, DC: U.S. Department of Health and Human Services.
Plass, D., Vos, T., Hornberg, C., Scheidt-Nave, C., Zeeb, H., & Krämer, A. (2014). Entwicklung der Krankheitslast in Deutschland: Ergebnisse, Potenziale und Grenzen der Global Burden of Disease-Studie. Deutsches Ärzteblatt, 111(38), 629–638.
Puth, M.-T., Weckbecker, K., Schmid, M., & Münster, E. (2017). Prevalence of multimorbidity in Germany: impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health, 17(1), 826.
Robert Koch-Institut, Abteilung für Epidemiologie und Gesundheitsmonitoring (2018). Gesundheit in Deutschland aktuell 2014/2015-EHIS (GEDA 2014/2015-EHIS). Scientific Use File 1. Version. https://doi.org/10.7797/19-201415-1-1-1.
Rütten, A., & Pfeifer, K. (Eds.). (2017). Nationale Empfehlungen für Bewegung und Bewegungsförderung. Köln: BZgA.
Saß, A. C., Lange, C., Finger, J. D., Allen, J., Born, S., Hoebel, J., Ziese, T., et al. (2017). „Gesundheit in Deutschland aktuell“ – Neue Daten für Deutschland und Europa. Hintergrund und Studienmethodik von GEDA 2014/2015-EHIS. Journal of Health Monitoring, 2(1), 83–90.
Steindorf, K., Depenbusch, J., Haussmann, A., Tsiouris, A., Schmidt, L., Hermann, S., Ungar, N., et al. (2020). Change patterns and determinants of physical activity differ between breast, prostate, and colorectal cancer patients. Supportive Care in Cancer, 28, 3207–3218.
Steppuhn, H., Kuhnert, R., & Scheidt-Nave, C. (2017). 12-Monats-Prävalenz der bekannten chronisch obstruktiven Lungenerkrankung (COPD) in Deutschland. Journal of Health Monitoring, 2(3), 46–54.
Stewart, R., Held, C., Brown, R., Vedin, O., Hagstrom, E., Lonn, M. E., White, H., et al. (2013). Physical activity in patients with stable coronary heart disease: an international perspective. European Heart Journal, 34(42), 3286–3293.
Sudeck, G., & Pfeifer, K. (2016). Physical activity-related health competence as an integrative objective in exercise therapy—conception and validation of a short questionnaire. German Journal of Exercise and Sport Research, 46, 74–87.
Thorpe, O., Johnston, K., & Kumar, S. (2012). Barriers and enablers to physical activity participation in patients with COPD: a systematic review. Journal of Cardiopulmonary Rehabilitation and Prevention, 32, 359–369.
World Health Organization (WHO) (2001). International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization.
World Health Organization (WHO) (2010). Global recommendations on physical activity for health. Geneva: WHO.
World Health Organization (WHO) (2014). Global status report on noncommunicable diseases 2014. Geneva: WHO.
World Health Organization (WHO) (2018). More active people for a healthier world. Global action plan on physical activity 2018–2030. Geneva: WHO.
Zhao, M., Veeranki, S. P., Magnussen, C. G., & Xi, B. (2020). Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study. BMJ, 370, m2031.
Funding
Open Access funding enabled and organized by Projekt DEAL
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G. Sudeck, W. Geidl, K. Abu-Omar, J. D. Finger, I. Krauß and K. Pfeifer declare that they have no competing interests.
All studies performed involving human participants were in accordance with ethical standards indicated in each case. Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sudeck, G., Geidl, W., Abu-Omar, K. et al. Do adults with non-communicable diseases meet the German physical activity recommendations?. Ger J Exerc Sport Res 51, 183–193 (2021). https://doi.org/10.1007/s12662-021-00711-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12662-021-00711-z