
Abstract
Purpose
Sociodemographic risks contributing to health inequities are often inadequately captured and reported in critical care studies. To address the lack of standardized terms and definitions, we sought to develop a practical and convenient resource of questions and response options for collecting sociodemographic variables for critical care research.
Source
To identify domains and variables that impact health equity, we searched: 1) PubMed for critical care randomized trials (2010 to 2021); 2) high-impact critical care and general medicine journals for special issues relating to equity; and 3) governmental and nongovernmental resources.
Principal findings
We identified 23 domains associated with health equity, including pronouns, age, sex, gender identity, sexual orientation, race and ethnicity, visible minorities, language, household income, marital/relationship status, education, disabilities, immigrant and refugee status, employment, primary care access, expanded health insurance, internet access, housing security, food security, dependents, religion, and postal code. For each domain we provided standardized questions and response options; for 13/23 domains, we included more than one version of the question and response categories.
Conclusion
We developed a standardized, practical, and convenient demographic data collection tool for critical care research studies. Questions and response options can be adapted by researchers for inclusion in individual study questionnaires or case report forms.
Résumé
Objectif
Les risques sociodémographiques qui contribuent aux inégalités en matière de santé sont souvent mal saisis et rapportés dans les études de soins intensifs. Pour remédier au manque de termes et de définitions normalisés, nous avons cherché à élaborer une ressource à la fois pratique et utile de questions et d’options de réponse pour le recueil des variables sociodémographiques pour la recherche en soins intensifs.
Sources
Pour identifier les domaines et les variables qui ont une incidence sur l’équité en santé, nous avons effectué des recherches dans : 1) PubMed, pour en extraire les études randomisées en soins intensifs (2010 à 2021); 2) des revues de soins intensifs et de médecine générale à impact élevé pour identifier les numéros spéciaux liés à l’équité; et 3) les ressources gouvernementales et non gouvernementales.
Constatations principales
Nous avons identifié 23 domaines associés à l’équité en santé, y compris les pronoms, l’âge, le sexe, l’identité de genre, l’orientation sexuelle, la race et l’origine ethnique, les minorités visibles, la langue, le revenu du ménage, l’état matrimonial / relationnel, l’éducation, les handicaps, le statut d'immigrant·e et de réfugié·e, l’emploi, l’accès aux soins primaires, l’assurance maladie élargie, l’accès à l’internet, la sécurité du logement, la sécurité alimentaire, les personnes à charge, la religion et le code postal. Pour chaque domaine, nous avons fourni des questions et des options de réponse normalisées; pour 13/23 domaines, nous avons inclus plus d’une version des catégories de questions et réponses.
Conclusion
Nous avons mis au point un outil de collecte de données démographiques normalisé, pratique et utile pour la recherche en soins intensifs. Les options de questions et de réponses peuvent être adaptées par les chercheuses et chercheurs pour être incluses dans des questionnaires d’étude individuels ou des formulaires de présentation de cas.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Sociodemographic factors are highly related to health and health care inequities. Age, sex, gender identity, race, ethnicity, housing, neighbourhood, education, literacy, and income all affect an individual’s social capital and access to care and are associated with health outcomes.1,2,3,4,5 Understanding individuals and communities’ barriers to health care can help identify disparities, inform initiatives, and improve the quality of health care delivery.1,2 Nevertheless, sociodemographic risks contributing to health inequities are often inadequately captured and reported in health research.3,4,5
Within critical care medicine, marginalized groups have worse health outcomes,6,7 and are often under-represented in clinical trials.8,9 Identifying and addressing health inequities depends on robust data collection; however, barriers include the lack of standardized definitions, inconsistent reporting of sociodemographic variables,10 and insufficient granularity regarding sociodemographic variables (e.g., racial and ethnic categories). These issues limit the use of published data, prevent comparisons across studies and pooling of data, and impede efforts to ensure that study patients are representative of diverse communities. Funding bodies are increasingly mandating that research participants reflect the wider population, and journals are increasingly mandating reporting of study diversity variables to better reflect the representativeness of study findings.11 Nevertheless, an important first step to facilitate consistent collection and reporting of sociodemographic variables is to develop a tool for standardized data collection; no such tool currently exists.
The Canadian Critical Care Trials Group (CCCTG) is a highly productive research consortium dedicated to improving health care for critically ill patients.12 The CCCTG is committed to Equity, Diversity, Indigeneity, and Inclusion (EDII) within its policy development13 and scholarship, and prioritized the operationalization of granular demographic data collection and data disaggregation.14 To address the lack of standardized terms and definitions, we sought to develop a practical and convenient resource of questions and response options for collecting sociodemographic variables that could be adapted by researchers for inclusion in individual study questionnaires or case report forms.
Methods
We used a comprehensive search strategy to identify variables that are known or proposed economic and social risks for health inequity.
Instrument development
Item generation
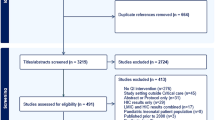
We searched PubMed from January 2010 to December 2021 for all critical care randomized trials; for each trial, we identified any sociodemographic variables significantly associated with patient outcomes. Concurrently, we searched for special issues relating to equity in high-impact critical care (Intensive Care Medicine, American Journal of Critical Care Medicine, Critical Care Medicine, Critical Care, and CHEST) and general medicine (New England Journal of Medicine, the Lancet, JAMA journals) journal websites. From these resources, we identified sociodemographic variables that have been associated with patient outcomes.
We searched selected Canadian and International governmental and nongovernmental organization (e.g., Health Canada, Ontario Human Rights Commission, Canadian Institutes of Health Research, Canadian Institute for Health Information, and Statistics Canada) websites for sociodemographic terms, categories, and response options relating to adults only. We did not consider terms relating exclusively to neonates or pediatric individuals. Three members of our team (Y. L., K. F., S. M.) reviewed the search results to identify all potential sociodemographic variables. We sampled to redundancy; that is, we terminated the search when we failed to identify new or additional domains or items.
Item reduction
The goal of item reduction was to retain 20–25 variables that are most likely to reflect risk factors for health inequities in critically ill patients, and are feasible to collect within critical care trials. Three members of our team (Y. L., K. F., S. M.) iteratively reached consensus on variables, prioritizing broad inclusion of known risk factors, and acknowledging that collection of some variables may not be feasible for retrospective studies or when critically ill patients are unable to provide their personal information because of impaired consciousness.
Instrument formatting and testing
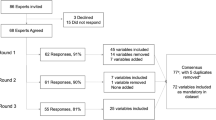
To meet the needs of researchers engaged in studies using diverse methodologies (e.g., questionnaires, surveys, observational studies, randomized trials) and scope (e.g., qualitative, population-based studies), we developed both concise and detailed versions of questions. Providing more than one question/response option will permit researchers to select the most appropriate version for their study requirements and population. When possible, questions and categorical response options were identified from official governmental and nongovernmental resources, and incorporated verbatim into the tool. If no response categories were identified from the resources, the authors drafted response options. The tool was iteratively revised based on review and input received from members of the CCCTG Equity, Diversity and Inclusion Working Group (nine members reflecting gender, ethnic, and professional diversity), and the CCCTG Executive Committee (six members reflecting gender, ethnic, and professional diversity).
Results
The comprehensive search generated 23 key domains related to sociodemographic variables associated with health risk and health care accessibility. Based on the variables identified in the search, we developed a toolkit for standardized data collection. The final tool includes questions and standardized response options relating to the following domains: pronouns, age, sex, gender identity, sexual orientation, race and ethnicity, visible minorities, language, household income, marital/relationship status, education, disabilities, immigrant and refugee status, employment, primary care access, expanded health insurance, internet access, housing security, food security, dependents, religion, and postal code/geography (Electronic Supplementary Material eAppendix). When categorical response options were identified from official governmental and nongovernmental resources, a citation is provided. If response categories were not identified from the resources, the authors drafted response options based on their review of published literature (i.e., domains 1, 14, 16, 18, and 19).
For 13 of the 23 domains, the data collection tool includes two or more versions of the question–response dyad, which enables investigators to select the version that is most appropriate for their study type and population. While investigators may modify questions and response options, this may limit standardization of questions and comparisons across studies.
The data collection tool was designed to be used in conjunction with a comprehensive glossary of EDII terms developed simultaneously by the CCCTG, which will be published separately. While the data collection tool mirrors the categories and terms initially included in the glossary, it can also be used by researchers as a standalone resource.
Discussion
Using a comprehensive search strategy, we developed a data collection toolkit on behalf of the CCCTG. The toolkit includes questions and response options relating to recognized sociodemographic determinants of health that can be tailored and incorporated into research initiatives. This convenient toolkit complements the CCCTG EDII glossary, which will be published separately. Together, the toolkit and glossary are important first steps to address an unmet need and provide researchers who are designing and conducting studies with a unique and valuable resource.
Unless we identify and address these sociodemographic determinants of health, we cannot begin to remedy the inequities that currently exist within our health care systems. Quantifying a social determinant’s impact on morbidity and mortality can help understand its scope. Standardized and consistent measurement and reporting of sociodemographic variables over time is essential to permit robust intersectional analyses and understand the needs and barriers of certain groups.15, 16 Nevertheless, there are critical barriers to actualizing this ideal of comprehensive, transferable, and granular data, including the lack of standardized terms and definitions, and the lack of integration of research and health care databases.
This data collection tool includes a broad list of social factors related to health disparities. The tool is expected to reduce researcher workload and enhance research efficiency by eliminating the need for investigators to develop their own questions and response options. Collecting standardized and expansive sociodemographic data will enable evaluation of the intersectionality of race, ethnicity, socioeconomic status, and critical illness.16 Consistent and clear language in data collection will also serve to reduce ambiguity, enable sharing of study databases, provide a framework to enable comparisons with other studies and among research consortia, and enable pooling of data across studies. Further, transparent data will provide reassurance regarding the generalizability of study results to the diverse populations, identify groups that are under-represented in research, and prompt development of novel strategies to ensure adequate and appropriate representation.11
This toolkit has limitations. We focused on adults in Canadian settings, so terms and concepts that are pediatric-specific are not represented in this tool. Additionally, selected terms may not be generalizable or applicable in other jurisdictions. Some variables may not be appropriate for retrospective studies, as the data may not be available in patient records. We did not conduct a formal systematic review. Our search strategy may not have identified all relevant terms; and terminology relating to diversity can be regional or personal, and not all readers will agree with the terms or acronyms we have included. Sensitivity is required when asking participants about their personal information; it is beyond the scope of this document to provide guidance on the best strategies.
Given that social determinants of health may change over time, this data collection tool will require periodic updating to remain current, relevant, and reflective of societal changes; these updates will be informed by the perspectives of CCCTG members, patients and families, and community partners. The data collection tool will be posted on the CCCTG website and disseminated to CCCTG members for use in their research initiatives. The next steps will involve eliciting broad perspectives from all stakeholders regarding toolkit elements, response options, and language.
Equitable health care is a national priority. Opportunities to participate in clinical research are an essential component of providing equitable health care to diverse populations and diverse patient representation within clinical trials improves scientific generalizability. Structured data collection is an important element of the vision to generate inclusive science, and to identify and address health care inequities in Canadian critical care.
References
Ahnquist J, Wamala SP, Lindstrom M. Social determinants of health -- a question of social or economic capital? Interaction effects of socioeconomic factors on health outcomes. Soc Sci Med 2012; 74: 930–9. https://doi.org/10.1016/j.socscimed.2011.11.026
Braveman PA, Kumanyika S, Fielding J, et al. Health disparities and health equity: the issue is justice. Am J Public Health 2011; 101: 149–56. https://doi.org/10.2105/AJPH.2010.300062
Chauhan A, Walton M, Manias E, et al. The safety of health care for ethnic minority patients: a systematic review. Int J Equity in Health 2020; 19: 1–25. https://doi.org/10.1186/s12939-020-01223-2
Dunne C. Black women’s health matters. BCMJ 2020; 62: 203–4.
Hilton CL, Fitzgerald RT, Jackson KM, et al. Brief report: under-representation of African Americans in autism genetic research: a rationale for inclusion of subjects representing diverse family structures. J Autism Dev Disord 2010, 40: 633–9. https://doi.org/10.1007/s10803-009-0905-2
Fowler RA, Sabur N, Li P, et al. Sex- and age-based differences in the delivery and outcomes of critical care. CMAJ 2007; 177: 1513–9. https://doi.org/10.1503/cmaj.071112
McGowan SK, Sarigiannis KA, Fox SC, Gottlieb MA, Chen E. Racial disparities in ICU outcomes: a systematic review. Crit Care Med 2022; 50: 1–20. https://doi.org/10.1097/ccm.0000000000005269
Saleem D, Gusman E, Manson DK, et al. Ethnic diversity among participants in clinical trials of critical illness. Am J Respir Crit Care Med 2020; 201: A4809. https://doi.org/10.1164/ajrccm-conference.2020.201.1_MeetingAbstracts.A4809
Van Spall HG, Toren A, Kiss A, Fowler RA. Eligibility criteria of randomized controlled trials published in high-impact general medical journals: a systematic sampling review. JAMA 2007; 297: 1233–40. https://doi.org/10.1001/jama.297.11.1233
Orkin AM, Nicoll G, Persaud N, Pinto AD. Reporting of sociodemographic variables in randomized clinical trials, 2014-2020. JAMA Netw Open 2021; 4: 6–10. https://doi.org/10.1001/jamanetworkopen.2021.10700
Editors, Rubin E. Striving for diversity in research studies. N Engl J Med 2021; 385: 1429–30. https://doi.org/10.1056/NEJMe2114651
Canadian Critical Care Trials Group (CCCTG). Research coordinators group (CCCRCG), 2012. Available from URL: https://www.ccctg.ca/CCCTG/CCCRCG (accessed July 2022).
Canadian Critical Care Trials Group (CCCTG). Canadian Critical Care Trials Group diversity policy, 2018. Available from URL: https://www.ccctg.ca/ccctg/media/Banners/PDF%20Documents/CCCTG-Diversity-Policy-11-April-2018.pdf (accessed July 2022).
Seely AJ, Fowler R. Importance of nationally coordinated data collection and quality improvement networks. Can J Respir Crit Care Sleep Med 2021; 6: 6–8. https://doi.org/10.1080/24745332.2021.1946448
Baker KE, Streed CG Jr, Durso LE. Ensuring that LGBTQI+ people count-collecting data on sexual orientation, gender identity, and intersex status. New Engl J Med 2021; 384: 1184–6. https://doi.org/10.1056/nejmp2032447
Carbado DW, Crenshaw KW, Mays VM, Tomlinson B. Intersectionality: mapping the movements of a theory. Du Bois Rev 2013; 10: 303–12. https://doi.org/10.1017/s1742058x13000349
Author contributions
Yiyan Li, Kirsten Fiest, and Sangeeta Mehta contributed to all aspects of this manuscript, including study conception and design; acquisition, analysis, and interpretation of data; and drafting the article. Karen E. A. Burns, Katie O’Hearn, Christina Maratta, Kusum Menon, Bram Rochwerg, Srinivas Murthy, and Rob Fowler contributed to the conception and design of the study.
Acknowledgements
We are grateful to Julie Reid, PT, PhD, for reviewing the manuscript.
Disclosures
None.
Funding statement
This study received no funding.
Editorial responsibility
This submission was handled by Dr. Vishal Uppal, Associate Editor, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, Y., Fiest, K., Burns, K.E.A. et al. Addressing health care inequities in Canadian critical care through inclusive science: a pilot tool for standardized data collection. Can J Anesth/J Can Anesth 70, 963–967 (2023). https://doi.org/10.1007/s12630-023-02450-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-023-02450-1