
Abstract
Purpose
The purpose of this study was to investigate myometrial contractility induced by oxytocin in women with advanced maternal age (AMA) and morbid obesity (MO). We hypothesized that both oxytocin-pretreated and oxytocin-naïve myometrial tissues from women of AMA and women who are MO would exhibit poor myometrial contractility compared with women that are younger and of normal body mass index (BMI).
Methods
This prospective in vitro study was conducted using myometrial samples obtained from women undergoing elective Cesarean deliveries. Three groups of patient were studied: control (≤ 35 yr; BMI, 20–24.9 kg·m−2), AMA (≥ 40 yr; BMI, 20–24.9 kg·m−2), and MO (≤ 35 yr BMI, ≥ 40 kg·m−2). Each myometrial strip was either pretreated with oxytocin 10−5 M or left in physiologic salt solution for two hours. This was followed by a dose-response testing to oxytocin (10−10 M to 10−5 M), during which contractile parameters were measured. The primary outcome was motility index (MI, amplitude × frequency) of contractions.
Results
The MI of contractions was reduced in oxytocin-pretreated samples when compared with their oxytocin naïve counterparts in control (estimated difference −69%; 95% confidence interval [CI], −82 to −48; P < 0.001) and AMA groups (estimated difference, −44%; 95% CI, −68 to −2; P = 0.07). The MI of contractions was not different between oxytocin naïve and oxytocin-pretreated samples from MO women (estimated difference, −26%; 95% CI, −63 to 49; P = 0.46); however, it was significantly lower in these groups compared with oxytocin-naïve samples from the control group.
Conclusions
Oxytocin pre-treatment reduced myometrial contractility in AMA and control group women compared with their oxytocin-naïve counterparts, as a function of the desensitization phenomenon. Attenuated oxytocin-induced myometrial contractility in MO women in both oxytocin-pretreated and oxytocin-naïve samples suggests that these women have intrinsically reduced uterine contractile ability.
Trial registration
www.clinicaltrials.gov (NCT01865669; registered 28 May, 2013).
Résumé
Objectif
L’objectif de cette recherche était d’étudier la contractilité myométriale induite par l’oxytocine chez des femmes d’âge maternel avancé (AMA) et ayant une obésité morbide (OM). Nous avons formulé l’hypothèse que les tissus de myomètre prétraités avec de l’oxytocine ainsi que les tissus naïfs d’oxytocine provenant de femmes d’AMA ou ayant une OM présenteraient une mauvaise contractilité comparativement à des femmes plus jeunes et à l’indice de masse corporelle (IMC) normal.
Méthodes
Cette étude prospective in vitro a été menée en utilisant des échantillons de myomètre prélevés sur des femmes accouchant par césarienne planifiée. Trois groupes de patientes ont été étudiés : contrôles (≤ 35 ans; IMC, 20 à 24,9 kg·m−2), AMA (≥ 40 ans; IMC, 20 à 24,9 kg·m−2) et OM (≤ 35 ans IMC, ≥ 40 kg·m−2). Chaque bandelette de myomètre a été prétraitée avec de l’oxytocine 10−5 M ou laissée dans une solution salée physiologique pendant deux heures. Cela a été suivi de tests de réponse à des doses croissantes d’oxytocine (10−10 M à 10−5 M) au cours desquels les paramètres contractiles ont été mesurés. Le critère d’évaluation principal était l’indice de motilité (IM, amplitude × fréquence) des contractions.
Résultats
Cet IM des contractions était diminué dans les échantillons prétraités avec l’oxytocine, comparativement à leurs équivalents naïfs d’oxytocine dans les groupes contrôles (différence estimée -69 %; intervalle de confiance [IC] à 95 % : -82 à -48; P < 0,001) et AMA (différence estimée, -44 %; IC à 95 %, -68 à -2; P = 0,07). L’IM des contractions n’était pas différent entre les échantillons naïfs d’oxytocine et les échantillons prétraités provenant de femmes ayant une OM (différence estimée, -26 %; IC à 95 %, -63 à 49; P = 0,46). Il était cependant significativement plus faible dans ces groupes comparativement aux échantillons naïfs pour l’oxytocine provenant du groupe contrôle.
Conclusions
Le prétraitement à l’oxytocine a réduit la contractilité myométriale des femmes des groupes AMA et contrôle comparativement à celle des prélèvements naïfs d’oxytocine en fonction d’un phénomène de désensibilisation. L’atténuation de la contractilité myométriale induite par l’oxytocine dans les échantillons prétraités et naïfs d’oxytocine chez les femmes présentant une OM suggère que ces dernières présentent une capacité contractile intrinsèquement réduite de l’utérus.
Enregistrement de l’essai clinique
www.clinicaltrials.gov (NCT01865669; enregistré le 28 mai 2013).
Similar content being viewed by others


The past decade has seen a significant shift in the demographics of childbearing women in the United States, Canada, and several other countries. In Canada, the average age at childbirth has been increasing over time, with almost one in five women being over 35 yr of age. From 1998 to 2007, the rate of live births for women over 40 yr of age increased by 48% (from 2.9 to 4.3 per 1,000 women).1 Advanced maternal age (AMA) women have higher rates of dysfunctional labour, labour augmentation with oxytocin, intrapartum Cesarean delivery (CD), postpartum hemorrhage (PPH), and blood transfusion.2,3,4
There has also been a worldwide exponential increase in the rate of obesity. The proportion of overweight and obese women in Canada increased from 34% in 1978 to 57% in 2018.5 Concordantly, rates of obesity in pregnancy have also increased, with 34% of women being reported as overweight and obese, according to 2016 data from the Public Health Agency of Canada.6 Perinatal complications associated with maternal obesity include reduced spontaneous term labour, increased induction and augmentation of labour, and an increased risk of intrapartum CD for dysfunctional labour.6,7 Furthermore, the incidence of PPH increases with maternal obesity, and this complication is independent of delivery mode and oxytocin use.8
Postpartum hemorrhage is the most common cause of maternal mortality worldwide, with 70–80% of cases resulting directly from uterine atony.9,10 Oxytocin is the first-line agent for the prevention and treatment of PPH; however, it is also used to induce and augment labour to facilitate vaginal delivery.10 Prolonged exposure to large doses of oxytocin, such as during labour, can result in an attenuated contractile response to subsequent oxytocin administration, and consequently severe PPH secondary to uterine atony.11 These clinical findings are explained in part by the phenomenon of oxytocin receptor (OTR) desensitization.12,13,14,15 Under normal circumstances, uterine contractions are initiated when oxytocin binds to myometrial OTRs. Like other G-protein-coupled receptors, OTRs undergo rapid homologous desensitization due to prolonged stimulation. Continuous and prolonged exposure of cultured human myometrial cells to oxytocin downregulates OTRs and decreases OTR messenger ribonucleic acid expression and oxytocin-binding sites.12,13,14 Once the process of desensitization has begun, there is a decrease in the response of myocytes to any additional exogenous oxytocin, suggesting functional alterations of OTR localization and/or expression.16,17
Current studies on obese women, based on in vitro contractility analyses, provide conflicting evidence, with some suggesting increased and some suggesting decreased myometrial contractility compared with normal weight women.18,19 In much the same way, there is no clear consensus on the effect of aging on human myometrial contractility.20,21 Furthermore, no previous studies have investigated if the oxytocin desensitization phenomenon specifically affects myometrial contractility in these at-risk populations.
The objective of this study was to investigate the pharmacological dose-response profiles of oxytocin by in vitro isometric tension measurements of contractions in oxytocin-pretreated and oxytocin-naïve myometrial samples from women with AMA and morbid obesity (MO), and to compare them with those from younger and normal weight women. We used our previously validated in vitro desensitization model to study the phenomenon.15 We hypothesized that women with AMA and MO would exhibit poor myometrial contractility compared with women that are younger and of normal BMI, in both oxytocin-pretreated and oxytocin-naïve myometrium.
Methods
After approval by the Research Ethics Board, Mount Sinai Hospital, Toronto, ON, Canada (MSH REB # 13-0024-E, dated April 30, 2013), this prospective laboratory study was conducted at Mount Sinai Hospital and the Lunenfeld-Tanenbaum Research Institute in Toronto, ON, Canada from May 29, 2013 to June 13, 2017. The study included non-labouring singleton pregnant women at 37–40 weeks gestational age undergoing elective primary or first repeat CD under spinal anesthesia. Written informed consent was obtained from all women enrolled in the study. Exclusion criteria were labouring women, those with more than two previous CDs or other myometrial surgeries, CD under general anesthesia, use of medications affecting uterine contractility, and any condition predisposing to uterine atony or PPH (such as multiple gestation, abnormal placentation, preeclampsia, polyhydramnios, macrosomia, uterine fibroids, chorioamnionitis, coagulopathy, or a history of PPH). Three patient populations were studied: control group with age ≤ 35 yr and normal pre-pregnancy BMI of 20–24.9 kg·m−2, AMA group with age ≥ 40 yr and normal pre-pregnancy BMI of 20–24.9 kg·m−2, and MO group with age ≤ 35 yr and pre-pregnancy BMI ≥ 40 kg·m−2.
Anesthethic technique, tissue collection, and tissue preparation
The attending anesthesiologist administered spinal anesthesia using 0.75% hyperbaric bupivacaine 1.8 mL with fentanyl 10 μg and morphine 100 μg, as per routine in our hospital with standard monitoring. The patients underwent CD via Pfannenstiel incision. After the delivery of the fetus and placenta, but before the administration of oxytocin, a small sliver of myometrium was excised from the upper border of the lower segment transverse uterine incision. The myometrial sample was immediately placed in 3-N-morpholino propanesulfonic acid buffer solution (145 mM sodium chloride [NaCl], 4.7 mM potassium chloride [KCl], 1.5 mM calcium chloride [CaCl2], 1.17 mM magnesium sulfate heptahydrate [MgSO4·H2O], 1.2 mM sodium phosphate monobasic [NaH2PO4·H2O], 3.0 mM 3-N-morpholino propanesulfonic acid solution, 5.0 mM glucose, and 2.0 mM pyruvate) with a pH of 7.4. If present, the endometrium and serosa were dissected away from the sample, after which the myometrial sample from each patient was divided longitudinally into four to eight strips (each with an approximate size of 10 mm × 2 mm × 1 mm), parallel to the direction of the muscle fibres.
Isometric tension recordings of contractility
For the contractility analysis, each myometrial strip was mounted into a single 10 mL organ-bath chamber (Radnoti 4-unit tissue-organ bath system [two systems], model 159920; Harvard Apparatus Canada, Montreal, QC, Canada) filled with physiologic salt solution (PSS) (112 mM NaCl, 25 mM NaHCO3, 1 mM potassium phosphate monobasic [KH2PO4], 5 mM KCl, 1.2 mM MgSO4·H2O, 11.5 mM glucose, and 2.5 mM CaCl2), at 37°C and pH 7.4, to mimic physiologic conditions. The organ-bath solution was aerated continuously with a mixture of 95% oxygen (O2) and 5% carbon dioxide (CO2). The myometrial strips were allowed to equilibrate in PSS at 1 g tension for up to two hours, until ten minutes of continuous, spontaneous rhythmic contractions developed. Myometrial strips not developing immediate spontaneous contractions were flushed with PSS every 15 min until regular contractions were obtained. After equilibration, the myometrial strips were stimulated with 120 mM KCl to provide both viability verification of the strips and a reference maximal contraction. The KCl solution was drained from the organ baths, and each chamber was washed three times with PSS to ensure full removal of any residual KCl.
Individual strips were either pretreated with oxytocin 10−5 M for two hours or left in PSS without oxytocin as a proxy for the labouring (and hence desensitized) and non-labouring uterus, respectively. This method is based on our previously established desensitization model, which showed a significant attenuation of oxytocin-induced myometrial contractions after pre-treatment with 10−5 M oxytocin for two hours.15 A pre-set list of these two treatment conditions was created before each experiment and allocated to each organ-bath chamber in a sequential manner. The study groups were sequentially rotated between the organ baths to ensure similar allocation of each study group to each organ bath, as well as to control.
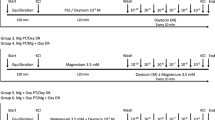
Following the two-hour pre-treatment period, the chambers were flushed three times with PSS, and allowed to re-equilibrate in the PSS solution for ten minutes. After the re-equilibration period, all strips were subjected to dose-response testing with 10−10 to 10−5 M oxytocin, increased cumulatively in a pattern of one-log molar concentration every ten minutes. At the end of the experiment, a final stimulation with 120 mM KCl confirmed the viability of the myometrial strips (Fig. 1). Myometrial strips failing to contract were removed and excluded from the analyses.

Experimental design. Myometrial strips were exposed to one of two 2-hr pre-treatment conditions: PSS (oxytocin-naïve) or oxytocin 10−5 M (oxytocin-pretreated/desensitized) for each study group (control, advanced maternal age, and morbid obese). The strips were then subjected to a dose-response testing with increasing concentrations of oxytocin in a pattern of 1 log molar increase every ten minutes from 10−10 to 10−5M. KCl = potassium chloride; PSS = physiologic salt solution
Myometrial contractions were continuously recorded using an isometric force transducer connected to a data acquisition system with AcqKnowledge® 3.9.0 software, MP 100 (Biopac System Inc, Gelota, CA, USA). The amplitude (g) and frequency of contractions (number of contractions [c] per ten minutes) were recorded for 600 sec during the equilibration period and during each step of the oxytocin dose-response period. The motility index (MI) (amplitude × frequency [g·c/10 min]) and area under the curve (AUC; integral force; g·sec−1) were calculated to determine the uterine activity and contractility, respectively. The contractile parameters were compared among the various groups. The primary outcome was MI, and secondary outcomes included frequency, amplitude, and AUC.
Statistical analysis
Statistical analysis was performed using SAS statistical software version 9.4 (The SAS Institute, Cary, NC, USA). All observations were normalized by dividing the outcome values by baselines measured during the equilibration period. Since the variables were non-normally distributed, outcomes in all of the analyses were log-transformed to satisfy the assumptions for regression models to be fitted. The values were expressed as either study group-specific predicted geometric means with 95% confidence intervals (CI) or estimated differences (with 95% CI) of the summation of measurements obtained over the range of oxytocin concentrations from 10−10 to 10−5 M during the dose-response period. An estimated difference is expressed as a ratio of two geometric means. Generalized linear regression models were fitted using SAS PROC GENMOD with identity link function. Generalized estimating equation was implemented in all models to account for repeated measures from the same patients. A compound symmetry structure was chosen for the covariance structure based on quasi-likelihood under the independence model (QIC) criterion model fit evaluation. The interpretations of the pairwise group comparisons are based on multiplicity-adjusted p-values obtained by applying the false discovery rate method; however, multiplicity-unadjusted p-values of all the specific pre-planned comparisons are also provided. A two-tailed P value of < 0.05 was considered statistically significant.
Our previous studies have shown that the effect size between two groups, where a significant difference existed for MI, could be expected to be between 0.7 and 1.4 √g·c/10 min with a standard error of 0.25–0.35 √g·c/10 min.15,22 Based on these assumptions, and powering for the beta of 80% and alpha of 0.05, a sample size of 28 strips per group was deemed adequate for analysis. This sample size was also deemed to have enough power to detect a geometric mean ratio as small as 1.7 (equivalent to relative difference of 70% or -41% depending on which group is used for reference) with 90% power, P < 0.01, and coefficient of variance within each group of 0.5.23
Results
Patients were recruited for this study from May 2013 to June 2017. Thirty-nine eligible women from the following three populations consented to participate in the study. A total of 236 experiments were conducted across the six study groups (oxytocin-pretreated and oxytocin naïve for three patient populations), of which 176 were successful (control, n = 64; AMA, n = 56; MO, n = 56) and used for analysis. The study flow chart with patient recruitment and sample distribution is shown in Fig. 2.

Flowchart showing patient recruitment and subsequent allocation of myometrial strips to each study group. Oxytocin-naïve = physiologic salt solution pre-treatment; oxytocin pretreated = 10−5 M oxytocin pre-treatment; N = number of patients; n = number of myometrial strips; Control: ≤ 35 yr and pre-pregnancy BMI (body mass index) = 20-24.9 kg·m−2; AMA (advanced maternal age): ≥ 40 yr and pre-pregnancy BMI = 20-24.9 kg·m−2; MO (morbid obese): ≤ 35 yr and pre-pregnancy BMI ≥ 40 kg·m−2
The clinical characteristics of the participants are shown in Table 1. The mean (standard deviation [SD]) age in the AMA group was 41.2 (2.1) yr. In the MO patient population, the mean (SD) pre-pregnancy BMI and BMI at delivery were 48.1 (7.5) kg·m−2 and 52.4 (5.9) kg·m−2, respectively. The median (range) gestational age for the entire patient population was 39.0 (37.0–40.4) weeks. None of the participants had any other co-morbidities such as hypertension or diabetes. Furthermore, none experienced any complications post-CD, including PPH, up to 24 hr postpartum or required any additional uterotonic agents.
Table 2 shows the summary of contractile parameters that were induced by increasing concentrations of oxytocin during the dose-response period in the control, AMA, and MO populations, in both oxytocin-pretreated and oxytocin-naïve settings, as estimated geometric mean with 95% CI. Estimated differences with 95% CIs between the contractile parameters in the six study groups are outlined in Table 3. The oxytocin dose-response curves for the MI, amplitude, frequency, and AUC for each of the six study groups are shown in Fig. 3.

The oxytocin dose-response curves for motility index, frequency, amplitude, and area under the curve of oxytocin-induced contractions during the dose response period for each study group. Oxytocin-naïve = physiologic salt solution pre-treatment; oxytocin pretreated = 10−5 M oxytocin pre-treatment; control = ≤ 35 yr and pre-pregnancy BMI (body mass index) = 20-24.9 kg·m−2; AMA (advanced maternal age): ≥ 40 yr and pre-pregnancy BMI = 20-24.9 kg·m−2; MO (morbid obese): ≤ 35 yr and pre-pregnancy BMI ≥ 40 kg·m−2
Oxytocin pre-treatment vs no pre-treatment in each study group
In the control group, myometrial strips that were pretreated with oxytocin generated a significantly lower geometric mean (95% CI) MI of contractions when compared with the oxytocin- naïve myometrial strips [0.386 (0.263 to 0.567) √g·c/10 min vs 1.253 (0.878 to 1.790) √g·c/10 min, respectively; estimated difference, −69%; 95% CI, −82% to −48%; P < 0.001]. Also the amplitude, frequency, and AUC were significantly reduced in the oxytocin-pretreated samples compared to untreated samples in the control group (Table 3).
There was a trend towards reduction in the geometric mean (95% CI) MI of contractions in oxytocin-pretreated myometrial strips in the AMA group compared with their oxytocin- naïve counterparts [0.764 (0.515 to 1.131) √g·c/10 min vs 1.354 (0.918 to 1.998) √g·c/10 min, respectively; estimated difference, −44%; 95% CI, −68 to −2; P = 0.07 (raw P = 0.04)]. The frequency of contractions was significantly reduced in pretreated samples compared with untreated samples from the AMA group, although there were no differences in amplitude and AUC (Table 3).
Although contractility was poor in oxytocin-pretreated strips from MO women compared with oxytocin-naïve strips, the difference (95% CI) was not statistically significant [0.519 (0.292 to 0.922) √g·c/10 min vs 0.696 (0.472 to 1.029) √g·c/10 min; estimated difference, −26%; 95% CI, −63 to 49; P = 0.46). No other significant differences were noted in any secondary outcomes between the pretreated and untreated study groups in MO women (Table 3).
Comparison of contractile parameters in oxytocin-naïve samples (no pre-treatment)
In oxytocin-naïve samples, no differences were observed in the MI, amplitude, frequency, and AUC of contractions between the AMA and control study groups (Table 3). Nevertheless, there was a significant reduction in the frequency (estimated difference, −38%; 95% CI, −58 to −7; P = 0.04) and trend towards reduction in the MI of contractions (estimated difference, −44%; 95% CI, −67 to −6; P = 0.06 [raw P = 0.03]) in the MO group compared with the control group, although there were no differences in the amplitude and AUC of contractions (Table 3).
Comparison of contractile parameters in oxytocin-pretreated samples
In oxytocin-pretreated samples, the MI was significantly higher in the AMA group compared with the control group (estimated difference, 98%; 95% CI, 14 to 242; P = 0.04) (Table 3). The amplitude frequency and AUC of contractions exhibited a similar pattern. Nevertheless, there were no differences in the contractile parameters between the oxytocin-pretreated samples of MO and control study groups. The MI in pretreated samples of the MO group was significantly lower compared with oxytocin-naïve samples from the control group (estimated difference, −59%; 95% CI, −79 to −19; P = 0.04).
Discussion
Our present in vitro study shows that oxytocin pre-treatment reduces oxytocin-induced myometrial contractility in samples obtained from young and normal weight women, as well as those with AMA, when compared with their oxytocin-naïve counterparts. This validates our previous findings of desensitization induced by oxytocin pre-exposure.15,22 There was a non-significant reduction in contractility in oxytocin-pretreated samples compared with oxytocin-naïve samples from MO women.
To date, only three studies have investigated the biological effects of aging on uterine contractility in vitro. Smith et al.24 found that spontaneous activity of human pregnant myometrium obtained from women in the age range of 22–45 yr is significantly reduced with increasing maternal age. Arrowsmith et al.20 made a similar observation, but only in non-pregnant myometrium. In pregnant myometrium, they found a small downward trend in spontaneous and oxytocin-induced contractility with increasing maternal age; however, it did not reach statistical significance. Through a more extensive series of experiments, Crankshaw et al. 21 concluded that there was no significant impairment in spontaneous and oxytocin-induced myometrial contractility with increasing maternal age in samples obtained from pregnant women aged 28–52 yr.
When we assessed oxytocin-induced myometrial contractility in oxytocin naïve myometrium, we observed that there were no differences in contractile ability between the control and AMA groups. Our findings are in agreement with previous studies,20,21,25 in which no significant impairment in myometrial contractility was observed with an increase in maternal age. These results, combined with a recent study that showed no significant variations in the smooth muscle content of human myometrium with increasing maternal age, suggest that other factors may increase PPH rates in AMA patients.25 For example, the incidence of risks factors associated with PPH may also increase with AMA, such as preeclampsia, placental abnormalities (placenta previa, low-lying placenta), macrosomia, and retained placenta.26 We excluded patients with such co-morbidities in our study to avoid any confounders and to assess the effect of only advanced age or morbid obesity on myometrial contractions.
In our current study, the findings concerning the effect of oxytocin desensitization on oxytocin-induced myometrial contractility in control population are consistent with our previous observations in other in vitro studies and are representative of what would normally occur in a clinical setting.15,22,27 Clinically, we have observed that women with oxytocin-augmented labour (desensitized myometrium) require nine-fold greater doses of oxytocin at CD to produce adequate uterine tone compared with non-labouring women (oxytocin-naïve myometrium). Furthermore, despite this higher oxytocin dose, blood loss is almost twice in labouring than that of non-labouring women.26,28 Myometrial samples from AMA patients behaved in much the same way, with oxytocin pre-treatment reducing oxytocin-induced myometrial contractility compared with their untreated counterparts.
To date, there has been no consensus regarding the intrinsic ability of human myometrium to contract in obese parturients. Zhang et al.18 have shown that myometrium from obese women spontaneously contracts with less force, frequency, and calcium flux than that from women with normal BMI, while Higgins et al.19 have shown that there is no correlation between maternal BMI and uterine contractility. In a most recent study by Crankshaw et al.,29 the investigators showed that not only does the time for the onset of spontaneous contractions but also the maximal amplitude and mean force of contractions increase with increasing BMI. Although this study investigated a wide range of maternal BMIs, from 19 to 50.1 kg·m−2, it is important to note that only 5% of the study population had a BMI greater than 35 kg·m−2.
In oxytocin-naïve samples, oxytocin-induced contractility in the MO group was attenuated (as evidenced by reduced frequency and MI) compared with the control group. Nevertheless, there was no difference in oxytocin-induced contractility between the control and MO groups in desensitized myometrium. Furthermore, oxytocin pre-treatment in the MO group only minimally reduced oxytocin-induced myometrial contractility compared with the oxytocin-naïve MO group. Taken together, these results support the hypothesis that morbid obesity is associated with an intrinsic impairment in uterine contractility, for which a further desensitization effect is not evident. Although the reasons for this impairment remain to be elucidated, several factors could be involved.
In light of the finding that OXTR gene and protein expression are not altered in response to increasing maternal BMI, it is possible that impaired contractility in MO patients is due to altered OXTR signalling downstream of the receptor.30 Alternatively, although there may be no changes in the quantity of the OXTR with increasing BMI, the receptors could still be functionally altered in such a way that would impact the binding of oxytocin to the OXTR.31 Cholesterol, which is elevated in MO women, can alter the ligand-binding function of the OXTR and other integral membrane components involved in myometrial contractility, by altering membrane viscosity and fluidity.32,33 Moynihan et al.34 have also previously shown that in vitro treatment with cholesterol can lead to a dose-dependent decrease in spontaneous and oxytocin-induced uterine contractions. In addition, cholesterol is a fundamental component of specialized lipid rafts known as caveolae in myocytes, on which potassium channels cluster. In obese women, these hyperpolarizing, pro-relaxant channels are more active as a result of elevated cholesterol levels and may conceivably contribute to the reduced myometrial contractility observed in this patient population.35,36 Leptin, apelin, and visfatin, which are also found at higher levels in MO women, have been shown to exert a similar inhibitory effect on uterine contractions in vitro.34,37 In mice, leptin supresses the expression and function of ROCK-1 and 2, which are involved in calcium sensitization during uterine contractility.38 More recently, it was shown that there is a significant decrease in p160 ROCK-1 protein expression in the myometrium of pregnant obese women, suggesting that this may play a role in inhibiting contractility in this patient population.39 Gam et al.40 also recently showed that myometrium from obese women has reduced myocyte density and increased triglyceride content, which may contribute to the reduced intrinsic contractile ability of myometrium in MO patients.
There are some limitations to this study. It must be acknowledged that these are in vitro experiments, and that although the organ-bath environment mimics physiologic conditions, in vivo conditions cannot be fully recapitulated. Nevertheless, this system has long been recognized as an appropriate method of quantifying and analyzing myometrial contractility, so we believe that our results are objective and robust. It should also be noted that in vitro concentrations of oxytocin may not reflect the exact in vivo levels, perhaps representing an overestimation in the experimental setting. Nevertheless, they are in agreement with previously studied concentrations and those used in clinical settings.14,15,22 The plasma levels of oxytocin during pregnancy, labour, and postpartum have been reported to be variable and range from 10−12 to 10−8 M.41,42,43,44 These may, however, not accurately reflect local myometrial concentration. The range of oxytocin (10−10 to 10−5 M) used during the dose-response testing likely reflects the levels reached after its parenteral administration postpartum.
In summary, we have investigated the effect of oxytocin desensitization on oxytocin-induced myometrial contractility in women with AMA and MO. We found that in oxytocin-naïve myometrium, oxytocin-induced contractility was unchanged and reduced in AMA and MO groups, respectively, when compared with the control group. In the presence of oxytocin desensitization, myometrial samples from AMA patients, much like those from control patients, showed reduced oxytocin-induced myometrial contractility compared with their oxytocin-naïve counterparts. In MO women, myometrial contractility is attenuated in both oxytocin-naïve and oxytocin-pretreated samples, suggesting that these women have an intrinsically reduced uterine contractility ability—however, studies regarding the pathobiology behind this are scarce, and therefore warranted.
References
Canadian Institution for Health Information. In Due Time: Why Maternal Age Matters. Available from URL: https://secure.cihi.ca/free_products/AIB_InDueTime_WhyMaternalAgeMatters_E.pdf (accessed February 2020).
Korb D, Goffinet F, Seco A, Chevret S, Deneux-Tharaux C; EPIMONS Study Group. Risk of severe maternal morbidity associated with cesarean delivery and the role of maternal age: a population-based propensity score analysis. CMAJ 2019; 191: E352-60.
Yogev Y, Melamed N, Bardin R, Tenenbaum-Gavish K, Ben-Shitrit G, Ben-Haroush A. Pregnancy outcome at extremely advanced maternal age. Am J Obstet Gynecol 2010; 203(558): e1-7.
Main DM, Main EK, Moore DH 2nd. The relationship between maternal age and uterine dysfunction: a continuous effect throughout reproductive life. Am J Obstet Gynecol 2000; 182: 1312-20.
Statistics Canada. Overweight and obese adults, 2018. Available from URL: https://www150.statcan.gc.ca/n1/en/pub/82-625-x/2019001/article/00005-eng.pdf?st=OBRuwojR (accessed February 2020).
Government of Canada. Effect of maternal weight on pregnancy outcomes. Available from URL: https://www.canada.ca/en/public-health/services/publications/healthy-living/effect-maternal-weight-pregnancy-outcomes.html (accessed February 2020).
Melchor I, Burgos J, Del Campo A, Aiartzaguena A, Gutierrez J, Melchor JC. Effect of maternal obesity on pregnancy outcomes in women delivering singleton babies: a historical cohort study. J Perinat Med 2019; 47: 625-30.
Butwick AJ, Abreo A, Bateman BT, et al. Effect of maternal body mass index on postpartum hemorrhage. Anesthesiology 2018; 128: 774-83.
Mehrabadi A, Liu S, Bartholomew S, et al.; Maternal Health Study Group of the Canadian Perinatal Surveillance System (Public Health Agency of Canada. Temporal trends in postpartum hemorrhage and severe postpartum hemorrhage in Canada from 2003 to 2010. J Obstet Gynaecol Can 2014; 36: 21-33.
Vogel JP, Williams M, Gallos I, Althabe F, Oladapo OT. WHO recommendations on uterotonics for postpartum haemorrhage prevention: what works, and which one? BMJ Glob Health 2019; DOI: https://doi.org/10.1136/bmjgh-2019-001466.
Grotegut CA, Paglia MJ, Johnson LN, Thames B, James AH. Oxytocin exposure during labor among women with postpartum hemorrhage secondary to uterine atony. Am J Obstet Gynecol 2011; 204(56): e1-6.
Phaneuf S, Asboth G, Carrasco MP, et al. Desensitization of oxytocin receptors in human myometrium. Hum Reprod Update 1998; 4: 625-33.
Phaneuf S, Rodriguez Linares B, TambyRaja RL, MacKenzie IZ, Lopez Bernal A. Loss of myometrial oxytocin receptors during oxytocin-induced and oxytocin-augmented labour. J Reprod Fertil 2000; 120: 91-7.
Robinson C, Schumann R, Zhang P, Young RC. Oxytocin-induced desensitization of the oxytocin receptor. Am J Obstet Gynecol 2003; 188: 497-502.
Balki M, Erik-Soussi M, Kingdom J, Carvalho JC. Oxytocin pretreatment attenuates oxytocin-induced contractions in human myometrium in vitro. Anesthesiology 2013; 119: 552-61.
Gimpl G, Reitz J, Brauer S, Trossen C. Oxytocin receptors: ligand binding, signalling and cholesterol dependence. Prog Brain Res 2008; 170: 193-204.
Smith MP, Ayad VJ, Mundell SJ, McArdle CA, Kelly E, Lopez Bernal A. Internalization and desensitization of the oxytocin receptor is inhibited by dynamin and clathrin mutants in human embryonic kidney 293 cells. Mol Endocrinol 2006; 20: 379-88.
Zhang J, Bricker L, Wray S, Quenby S. Poor uterine contractility in obese women. BJOG 2007; 114: 343-8.
Higgins CA, Martin W, Anderson L, et al. Maternal obesity and its relationship with spontaneous and oxytocin-induced contractility of human myometrium in vitro. Reprod Sci 2010; 17: 177-85.
Arrowsmith S, Robinson H, Noble K, Wray S. What do we know about what happens to myometrial function as women age? J Muscle Res Cell Motil 2012; 33: 209-17.
Crankshaw DJ, O’Brien YM, Crosby DA, Morrison JJ. Maternal age and contractility of human myometrium in pregnancy. Reprod Sci 2015; 22: 1229-35.
Balki M, Erik-Soussi M, Kingdom J, Carvalho JC. Comparative efficacy of uterotonic agents: in vitro contractions in isolated myometrial strips of labouring and non-labouring women. Can J Anesth 2014; 61: 808-18.
Newson R. Generalized power calculations for generalized linear models and more. Stata J 2004; 4: 379-401.
Smith GC, Cordeaux Y, White IR, et al. The effect of delaying childbirth on primary cesarean section rates. PLoS Med 2008; DOI: https://doi.org/10.1371/journal.pmed.0050144.
Sweeney EM, Crankshaw DJ, O’Brien Y, Dockery P, Morrison JJ. Stereology of human myometrium in pregnancy: influence of maternal body mass index and age. Am J Obstet Gynecol 2013; 208(324): e1-6.
Lao TT, Sahota DS, Cheng YK, Law LW, Leung TY. Advanced maternal age and postpartum hemorrhage - risk factor or red herring? J Matern Fetal Neonatal Med 2014; 27: 243-6.
Balki M, Ronayne M, Davies S, et al. Minimum oxytocin dose requirement after cesarean delivery for labor arrest. Obstet Gynecol 2006; 107: 45-50.
Carvalho JC, Balki M, Kingdom J, Windrim R. Oxytocin requirements at elective cesarean delivery: a dose-finding study. Obstet Gynecol 2004; 104: 1005-10.
Crankshaw DJ, O’Brien YM, Crosby DA, Morrison JJ. Maternal body mass index and spontaneous contractility of human myometrium in pregnancy. J Perinatol 2017; 37: 492-7.
Reversi A, Rimoldi V, Brambillasca S, Chini B. Effects of cholesterol manipulation on the signaling of the human oxytocin receptor. Am J Physiol Regul Integr Comp Physiol 2006; 291: R861-9.
Arthur P, Taggart MJ, Zielnik B, Wong S, Mitchell BF. Relationship between gene expression and function of uterotonic systems in the rat during gestation, uterine activation and both term and preterm labour. J Physiol 2008; 586: 6063-76.
Wiegand V, Gimpl G. Specification of the cholesterol interaction with the oxytocin receptor using a chimeric receptor approach. Eur J Pharmacol 2012; 676: 12-9.
Dreja K, Voldstedlund M, Vinten J, Tranum-Jensen J, Hellstrand P, Sward K. Cholesterol depletion disrupts caveolae and differentially impairs agonist-induced arterial contraction. Arterioscler Thromb Vasc Biol 2002; 22: 1267-72.
Moynihan AT, Hehir MP, Glavey SV, Smith TJ, Morrison JJ. Inhibitory effect of leptin on human uterine contractility in vitro. Am J Obstet Gynecol 2006; 195: 504-9.
Parkington HC, Stevenson J, Tonta MA, et al. Diminished hERG K+ channel activity facilitates strong human labour contractions but is dysregulated in obese women. Nat Commun 2014; DOI: https://doi.org/10.1038/ncomms5108.
Shmygol A, Noble K, Wray S. Depletion of membrane cholesterol eliminates the Ca2+-activated component of outward potassium current and decreases membrane capacitance in rat uterine myocytes. J Physiol 2007; 581: 445-56.
Hehir MP, Morrison JJ. The adipokine apelin and human uterine contractility. Am J Obstet Gynecol 2012; 206(359): e1-5.
Harrod JS, Rada CC, Pierce SL, England SK, Lamping KG. Altered contribution of RhoA/Rho kinase signaling in contractile activity of myometrium in leptin receptor-deficient mice. Am J Physiol Endocrinol Metab 2011; 301: E362-9.
O’Brien M, Carbin S, Morrison JJ, Smith TJ. Decreased myometrial p160 ROCK-1 expression in obese women at term pregnancy. Reprod Biol Endocrinol 2013; DOI: https://doi.org/10.1186/1477-7827-11-79.
Gam CM, Larsen LH, Mortensen OH, et al. Unchanged mitochondrial phenotype, but accumulation of lipids in the myometrium in obese pregnant women. J Physiol 2017; 595: 7109-22.
Seitchik J, Amico J, Robinson AG, Castillo M. Oxytocin augmentation of dysfunctional labor. IV. Oxytocin pharmacokinetics. Am J Obstet Gynecol 1984; 150: 225-8.
Kuwabara Y, Takeda S, Mizuno M, Sakamoto S. Oxytocin levels in maternal and fetal plasma, amniotic fluid, and neonatal plasma and urine. Arch Gynecol Obstet 1987; 241: 13-23.
Yamaguchi ET, Cardoso MM, Torres ML, et al. Serum oxytocin concentrations in elective caesarean delivery: a randomized comparison of three infusion regimens. Int J Obstet Anesth 2011; 20: 224-8.
Hawker RW, Walmsley CF, Roberts VS, Blackshaw JK, Downes JC. Oxytocic activity of human female blood. Endocrinology 1961; 69: 391-4.
Author contributions
Mrinalini Balki contributed to all aspects of this manuscript, including study conception and design; acquisition, analysis, and interpretation of data; and drafting the article. Alice Luca contributed to acquisition, analysis, and interpretation of data and drafting the article. Jose C.A. Carvalho contributed to the conception and design of the study, interpretation of data, and revision of the article. Nivetha Ramachandran contributed to the acquisition, analysis, and interpretation of data.
Acknowledgements
The authors acknowledge Eugene Woojin Yoon, MSc, statistician, Mount Sinai Hospital, for the statistical analysis of this study.
Conflicts of interest
None.
Funding statement
This research was supported by the Dr. R. A. Gordon Patient Safety Award, Canadian Anesthesia Research Foundation, Canadian Anesthesiologists’ Society. Dr. Mrinalini Balki was supported by funding from Canadian Anesthesiologists’ Society Career Scientist Award from the Canadian Anesthesia Research Foundation; and Merit Awards, Department of Anesthesia, University of Toronto. Dr. Jose Carvalho was supported by Merit Awards, Department of Anesthesia, University of Toronto.
Editorial responsibility
This submission was handled by Dr. Gregory L. Bryson, Deputy Editor-in-Chief, Canadian Journal of Anesthesia.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Luca, A.M., Carvalho, J.C.A., Ramachandran, N. et al. The effect of morbid obesity or advanced maternal age on oxytocin-induced myometrial contractions: an in vitro study. Can J Anesth/J Can Anesth 67, 836–846 (2020). https://doi.org/10.1007/s12630-020-01615-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-020-01615-6