
Abstract
Purpose
Deceased donation data requires standardization to enable accurate interprovincial and international comparisons of deceased donation performance. In Canada, most provincial organ donation organizations (ODOs) have developed different processes and infrastructures for referring potential donors and subsequent data collection. This has led to differing definitions of the performance measures used for each step in the donation process, from potential donor identification to consent to transplantation. The Deceased Donation Data Working Group (DDDWG), comprised of representatives from ODOs across Canada, was therefore convened by Canadian Blood Services to develop a national, comprehensive, standardized deceased donation minimum data set.
Methods
The DDDWG’s scope encompassed considering all potential deceased organ donation data elements, including operational and performance data collected along the deceased donor pathway from donation potential to donation and disposition of organs. An environmental scan was conducted of other existing deceased donation registries from the Canadian and the international community. The DDDWG then engaged in regular face-to-face meetings and teleconferences to develop recommendations for the minimum data set that would satisfy key considerations, including the impact on existing ODO data collection processes, financial impact on stakeholders, the clinical and operational needs of multiple healthcare professionals involved in the deceased donation pathway, and availability of other existing national data sets that could be leveraged to reduce data collection burden.
Results
The key deceased donation data elements identified by the DDDWG are contained in an inverted pyramid framework that was derived from similar work conducted in other countries.
Conclusion
The DDDWG developed recommendations for proposed definitions and data sources that should be adopted nationally to guide the collection of deceased donation data. The ultimate purpose of the final minimum data set is to harmonize and standardize donation data definitions in Canada and align with international standards; inform the development of operational and clinical practice standards at the provincial and national levels; develop a framework for deceased donation performance measures; and advance the science of deceased donation.
Résumé
Objectif
Les données concernant les dons d’organes de personnes décédées doivent être normalisées pour permettre des comparaisons précises de l’efficacité de ces dons entre provinces et entre pays. Au Canada, la majorité des organismes provinciaux de dons d’organes (ODO) ont élaboré divers processus et infrastructures pour l’orientation des donneurs potentiels et la collecte subséquente des données. Cela a abouti à des définitions différentes des mesures de performances utilisées pour chaque étape du processus de don, de l’identification du donneur potentiel au consentement à la transplantation. Le Groupe de travail sur les données de donneurs décédés (DDDWG), constitué de représentants des ODO de tout le Canada a donc été réuni par la Société canadienne du sang (SCS) pour élaborer un ensemble national et complet de données minimums standardisées de dons d’organes de personnes décédées.
Méthodes
Le DDDWG avait pour mission d’envisager tous les éléments de données de dons d’organes potentiels de personnes décédées, y compris les données opérationnelles et de performance collectées le long du parcours du donneur décédé, depuis le don potentiel jusqu’à l’utilisation des organes. Une analyse environnementale des autres registres existants (canadiens et internationaux) de dons d’organes de personnes décédées a été effectuée. Le DDDWG a alors entrepris des entretiens en face à face et des téléconférences pour élaborer ses recommandations pour un ensemble minimum de données qui répondraient aux problèmes clés, y compris : leur impact sur les processus de collecte de données des ODO existants, l’impact financier pour les différents acteurs, les besoins cliniques et opérationnels des multiples professionnels de santé impliqués tout au long du parcours de don de la personne décédée, et la disponibilité d’autres ensembles de données qui pourraient être utilisés pour réduire le fardeau de la collecte des données.
Résultats
Les principales données de don d’organes de donneur décédé, identifiées par le DDDWG, tiennent dans un cadre en pyramide inversée tiré d’un travail semblable mené dans d’autres pays.
Conclusion
Le DDDWG a élaboré des recommandations pour les définitions proposées et les sources de données qui devraient être adoptées à l’échelon national pour guider la collecte des données de dons d’organes de personnes décédées. Le but ultime de l’ensemble minimum final de données est d’harmoniser et standardiser les définitions des données concernant les dons au Canada et de s’aligner sur les normes internationales; d’informer le développement de normes opérationnelles et de pratique clinique au niveau des provinces et au niveau national; de développer un cadre pour la mesure des performances concernant les dons de donneurs décédés; et de faire progresser les connaissances sur ce type de dons.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Deceased donation data requires standardization as well as harmonization with international specifications.1 In Canada, most provincial organ donation organizations (ODOs) have developed different processes and infrastructure for referring potential donors and subsequent data collection. This has led to differing definitions of the performance measures used for each step in the donation process from potential donor identification to consent to transplantation.
The absence of standardized definitions in Canada precludes accurate interprovincial and international comparisons of deceased donation performance. Comparing deceased donation performance data is also limited by the most widely used performance index: deceased donors per million population (DPMP). Donors per million population uses population estimates as the “potential pool” from which solid organ donors (subsequently referred to as organ donors) become available. The advantages of using DPMP are that data are readily available and relatively easy to obtain at little or no cost. Nevertheless, DPMP may be an imperfect reflection of program performance because the denominator is composed of a pool of living people, whereas only a small percentage of deaths will be eligible for organ donation (primarily deaths due to devastating brain injury).2 In addition, the rates of these causes of death may vary between jurisdictions and across age categories. Therefore, the “true potential donor pool” can fluctuate substantially depending upon patterns of specific causes of death and/or the age distribution of a population. A higher DPMP may simply reflect a larger pool of potential donors rather than better program performance.
Other measures of program performance have been proposed,3,4,5 but their accuracy is also predicated on the use of numerators and denominators that are well defined and collected using similar approaches across jurisdictions. In Canada, most provincial organ donation organizations (ODOs) have developed different processes and infrastructures for referring potential donors and subsequent data collection. This has led to differing definitions of the performance measures used for each step in the donation process, from potential donor identification to consent to transplantation. Even when a common definition is used across the country it may not be in alignment with international measures. For example, in Canada, a deceased donor is defined as someone from whom at least one organ was transplanted into a recipient. However, Spain, the United States of America, and the United Kingdom all define a deceased donor as someone from whom at least one organ was recovered for the purpose of transplantation (but not necessarily transplanted into a recipient). Canada’s definition of deceased donation therefore leads to underestimation of its comparative donor rate relative to these other countries, unless its donor rate can be recalculated using similar definitions. The development of a national deceased donation minimum data set with standardized definitions is therefore essential for accurate ODO performance measurement, reporting, and benchmarking across regions and between countries.
Objectives
A mandate of Canadian Blood Services (CBS) is to “lead national practices, professional education, public awareness, and system performance activities for organ and tissue donation and transplantation”. As part of this mandate, CBS convened a Deceased Donation Data Working Group (DDDWG) in June 2014 to develop a national, comprehensive, standardized deceased donation minimum data set. The DDDWG comprised representatives from ODOs across Canada and experts familiar with existing national health databases. The DDDWG’s scope encompassed reviewing deceased organ donation data, including operational and performance data collected along the deceased donor pathway, from donation potential to donation and disposition of organs. The purposes of the final minimum data set were to: harmonize and standardize donation data definitions in Canada and align with international standards; inform the development of operational and clinical practice standards at the provincial and national levels; develop a framework for deceased donation performance measures; and advance the science of deceased donation.
Methods
Group formation
The Chair of the DDDWG was appointed by CBS. Working group members were selected from across Canada to represent ODOs and based on relevant professional knowledge and experience in deceased donation and in data management. The final group contained representatives from the following organizations: BC Transplant, BC; Southern Alberta Organ and Tissue Donation Program and Human Organ Procurement and Exchange, AB; Transplant Manitoba - Gift of Life, MB; Trillium Gift of Life Network, ON; Transplant Québec, QC; Nova Scotia Organ and Tissue Donation Program, NS; Canadian Institute for Health Information; Canadian National Transplant Research Program; and CBS. Members had different medical professional backgrounds, including representation from ODO leadership and coordination roles, physicians and nurses, and adult and pediatric clinical practice. An initial teleconference call was convened to review the terms of reference (TOR) and agree on the approach the DDDWG would take to achieve its mandate. A face-to-face meeting was convened on September 15, 2014 to: approve the TOR; review current data capabilities; discuss principles and key considerations to guide the development of a minimum data set; review the data collation process; and walk through the collated data set (data scan) to identify and analyze data for the development of a minimum data set. Following this meeting, regular teleconference meetings occurred to discuss emerging issues, develop recommendations, and gain expertise from other knowledge areas. The diagram below outlines the basic process methodolgy adopted by the group used by CBS to build consensus, and is similar to the Consensus Development Conference introduced by the National Institue of Health.6 The DDDWG TOR required that a majority of the voting members of the DDDWG constitute a quorum (Fig. 1).

Reproduced with permission from the Canadian Blood Services
Process overview.
Principles
During the development of the data set and recommendations, the DDDWG started with the guiding principles for national organ donation and transplant data management as recommended in a Canadian National Workshop.7 These guiding principles focus on governance, data scope, data compliance, data standardization, data quality, data stewardship, data accessibility, and system efficiency. To encompass elements specific to its mandate of developing a national minimum data set for deceased donation, the DDDWG expanded this list to include the following principles:
-
1.
Data collection will be instrumental in advancing scientific evidence-based healthcare.
-
2.
The final minimum data set will be meaningful, comparable, measurable, and unambiguous, making data collection easy for data collectors.
-
3.
The minimum data set will support data sharing and satisfy international data contributions.
-
4.
The minimum data set will be defined as containing the elements that the system should aspire to collect.
-
5.
The national minimum data set will provide guidance on data definitions and interpretations where national data standardization is required. It will serve as a national minimum data platform, while provincial data sets can include additional data.
-
6.
The DDDWG will ensure that the national minimum data set lends itself to national and international benchmarking by ODO.
-
7.
The minimum data set will not be static. It will need to evolve and be re-evaluated on a scheduled timeline.
-
8.
The minimum data set should be used for the benefit of donors, families, patients, recipients, provincial and federal governments, and Canadians.
Key considerations
During the development of the national minimum data set, DDDWG identified the following key considerations:
-
1.
The changes required as a result of the recommended national data set will impact existing ODO data collection and reporting processes.
-
2.
There is an anticipated financial impact to stakeholders due to the need for increased resources, infrastructure, and development of requirements necessary to support the recommended data collection and data linkages between electronic systems.
-
3.
There is an opportunity to satisfy international data commitments through a consolidated approach to the minimum data set.
-
4.
The minimum data set considers national practices and the data needs of all health care professionals involved on the deceased donation critical pathway.
-
5.
The transplant and donation community is working towards a national data, analytics, and reporting system that will benefit donation and transplantation in Canada.
-
6.
Existing data sets were used as a basis from which to start developing the minimum data set.
Synthesis of available information
At the first meeting, the DDDWG was provided with results of a comparative evaluation conducted by one of the DDDWG members (K. Hornby, unpublished MSc thesis), which compared different organ donation definitions and performance metrics from the following countries and organizations: the World Health Organization, Australia, Austria, Canada, Finland, France, Germany, the Netherlands, Spain, the United Kingdom, and the United States of America. The DDDWG then conducted an environmental scan of existing deceased donation registries and data collections from all Canadian ODOs and Canadian administrative databases. The environmental scan described what deceased donation data elements are being collected and helped inform what elements to include in the minimum data set (Table 1). The findings of this environmental scan were summarized in a large spreadsheet file and circulated to the group, and used as the basis for subsequent discussions about definitions and data elements (summary available upon request). The DDDWG also considered and included data that would be required by transplant programs to assess the candidacy of the deceased donor for transplant, and recommended the inclusion of these data elements as identified by the various organ-specific data working groups convened by CBS.
Data collection considering time points
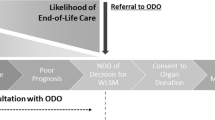
The transplant data working groups convened by CBS typically considered clinical trajectories of transplant recipients to ensure all major events and data were captured at the appropriate time point. Nevertheless, given the frequent non-linearity of the deceased donation process, the DDDWG utilized an inverted pyramid framework, adapted from the one used by the Australian Organ and Tissue Donation and Transplantation Authority,8 to guide the identification of data elements. This is described in greater detail in the results section.
Data analysis and review
The DDDWG was responsible for highlighting existing data gaps and determining what new elements were required to reconcile these disparities. To accommodate the identification of data gaps, the environmental scan was organized along two axes: 1) data category (identification of opportunity, referral, declaration of death, family engagement, consent, donor management, assessment, allocation, offer, international organ sharing, logistics [pre, intra, post-transplant], recovery, package and label, organ disposition, post donation, and reporting and measurement) and 2) existing data sources (Table 1). This provided the DDDWG with a detailed understanding of what deceased donation data elements are currently collected by existing programs. The DDDWG then employed an iterative review approach to refine the minimum data set and ensure all aspects of the deceased donation process were captured with the appropriate level of detail. As part of the analysis process, specific sub areas of interest were identified and additional information was captured. This information was presented back to the group for further exploration, discussion, modification, approval, and inclusion into the final minimum data set.
Results
The data pyramid
The key deceased donation data elements identified by the DDDWG are contained in the inverted pyramid framework (Fig. 2). The DDDWG recommends that these concepts, their definitions, and data sources (Tables 2 and 3) be adopted nationally to guide the collection of deceased donation data.

Adapted with permission from Figure 8: Australia’s potential organ donor population (7). Reproduced with permission from the Canadian Blood Services
Deceased donation information pyramid.
Each level in the pyramid represents data collection that is required from a specific group or denominator of patients. The pyramid moves from data collection occurring at the level of the entire population, and becomes more focused with each subsequent level until reaching the apex of utilized donors. More granular data collection is required at each successive (smaller) level of the pyramid. The pyramid is separated into two distinct sections by a bold horizontal line; data collection for groups identified above the line will be measured in aggregate using existing Canadian data sets: 1) Statistics Canada for population and deaths, and (2) the Canadian Institute for Health Information (CIHI) Discharge Abstract Database (DAD)-Hospital Morbidity Database (HMDB) and National Ambulatory Care Reporting System (NACRS). Information below the line will be sourced directly from the provincial ODOs (Table 2). This framework was developed to maximize efficiency and to take advantage of existing national data collection systems already in place (i.e., national health administrative databases), which utilize common data collection infrastructure and harmonized variable definitions. Using this approach, common performance metrics can be calculated that are derived from similar denominators across regions (Table 3).
Minimum data set—considerations and interpretations
All data elements in the minimum data set should be considered mandatory. The DDDWG recommended that the aggregated national minimum data set be maintained by CBS. Data from existing national data sets will be collected from each agency (e.g., CIHI) by CBS, and information from referred potential donors will be provided to CBS by the provincial ODOs. The DDDWG did not make recommendations regarding “optional” data elements, since these would not be part of the minimum data set. Notably, optional data would be incomplete as not all programs would be collecting the data and conclusions drawn from the data could be invalid.
The DDDWG considered how donors are reported as either those determined dead using circulatory criteria (DCD) or neurological criteria (NDD) and decided that it was not necessary to categorize each individual data element as being associated with either NDD or DCD. Nevertheless, sufficient detail about the deceased donor should be captured by ODOs to ensure the ability to distinguish between NDD and DCD (e.g., for calculation of metrics such as organs per donor, where rates between NDD and DCD are expected to vary, or conversion rates of eligible donors).
Emerging issues
The DDDWG identified several emerging issues that will require further discussion and development within the deceased donation community to improve the transparency and reporting of deceased donation performance metrics. These are summarized in the discussion section.
Discussion
National deceased donation data strategy
The DDDWG determined that the most important priority was to ensure the national deceased donor minimum data set is comprehensive, valid, and relevant to stakeholders across Canada. Comparative performance measures can therefore be derived from the minimum data. Accuracy of these performance measures is predicated on numerators and denominators that are well defined and collected using similar approaches across provinces. Nevertheless, most provincial ODOs in Canada have developed different processes and infrastructure for defining and referring potential donors and subsequent data collection. The DDDWG therefore recognized the importance of using existing population-level data that are collected using similar approaches across regions to describe the pool of potential donors. The CIHI-DAD-HMDB and the Canadian Transplant Registry both have a national scope, and provided a feasible methodology for creating performance measures for deceased donation using common data collection procedures and definitions. The DDDWG recognized that some stakeholders may choose to report deceased organ donation performance measures using different denominators than those that appear in the pyramid (e.g., per million persons vs per 1,000 hospitalized deaths vs per 1,000 ventilated deaths, etc.). The DDDWG considered these issues when creating a framework for data collection and reporting using the newly proposed minimum dataset. This approach ensures that Canadian deceased organ donation performance as measured by the minimum dataset can still be compared with other regions or countries using different denominators to describe the potential donor pool.
The DDDWG acknowledges that there may be discrepancies between the potential donor numbers identified using administrative data (smallest level above the line) and the referred potential donor numbers (largest level below the line) due to the different approaches used in collecting these data. Nevertheless, comparison of the number of patients in these levels across regions may provide insights to explain differences in estimates calculated at the national level (e.g., potential donors) and those obtained at the provincial level (e.g., referred potential donors).
Clinical triggers for referrals to organ donation organizations
Notably, there currently exists variability across provinces in the referral process for potential donors (due to differing clinical triggers that define when hospitals need to refer a potential donor) and also for the identification of eligible donors (due to variations in eligibility criteria). This variability reflects differences in local processes and standards, therefore it is not expected that numbers of potential donors estimated at the national level and numbers of referred potential donors will be the same. Nevertheless, the DDDWG recommends a clinical trigger initiative be undertaken to standardize definitions at a national level, and to ensure that referred potential donors are consistently defined. This work is currently underway. It is also recommended that an exclusion criteria initiative be undertaken to standardize exclusion criteria and to ensure that eligible donors are consistently defined.
Potential donor definition limitations
The DDDWG focused on identifying potential donors that had sustained a brain injury, since this is the most common condition leading to organ donation. Nevertheless, the DDDWG acknowledges that there may be cases of organ donation arising from other lethal conditions not associated with brain injury (e.g., end stage neuromuscular disorders such as amyotrophic lateral sclerosis, organ donation after medical assistance in dying) that will not be identified using the proposed framework for identifying potential donors based on national databases (e.g., CIHI-DAD-HDMB/NACRS). It is estimated that up to 10-15% of potential DCD donors (i.e., 2-3 % of all deceased donors) will not be captured using the proposed approach using the national databases. As well, depending upon the circumstances of the case, physician-assisted deaths may not be captured as potential donors. Patients with devastating brain injury who are never ventilated as part of their course of treatment, because it is deemed not to be in the best interest of the patient, will not be captured as potential donors. The impact of these limitations should be monitored (these cases will still be identified by provincial ODOs) and the definition of a potential donor using the national databases should be revisited if there is a substantial increase in these types of cases. In particular, the approach to measuring potential donors using the CIHI database may need to be modified to reflect changes in the epidemiology of organ donation.
CIHI-DAD/NACRS measurement of potential donor limitations
The CIHI-DAD (the national source for potential donor data, except Quebec) only identifies those patients that “ever received mechanical ventilation”, and therefore will not actually be able to capture potential donors who require “mechanical ventilation at or near the time of death”. Until more detailed data on the timing of mechanical ventilation is captured in the CIHI-DAD, only patients who died as a result of a brain injury who ever (yes or no) received mechanical ventilation will be captured as a potential donor. This may overestimate the number of potential donors. The DDDWG has submitted a request to CIHI to create a new CIHI-DAD variable representing “mechanical ventilation in the 24 hr prior to death”, and will work with CIHI to support this change.
Comprehensive identification of patients who have a neurological determination of death
An International Classification of Diseases-10-CA code exists to identify patients who have a determination of neurological death (G93.81). Nevertheless, this is an optional code rather than a mandatory data element, and thus it is not comprehensively collected in the CIHI-DAD/NACRS. Consistent use of this code in appropriate cases would allow for discrimination between deaths that occur following a determination of neurological death vs circulatory death. The DDDWG made a submission to CIHI to request that all deaths determined using neurologic criteria be identified as a mandatory data element.
Conclusion
This effort represents a fundamental step towards building a national deceased donation data system that utilizes common definitions and data collection approaches to improve transparency, accuracy, and interpretability. The ultimate purpose of the final minimum data set is to harmonize and standardize donation data definitions in Canada and align with international standards; inform the development of operational and clinical practice standards at the provincial and national levels; develop a framework for deceased donation performance measures; and advance the science of deceased donation.
References
Domınguez-Gil BD, Delmonico FL, Shaheen FA, et al. The critical pathway for deceased donation: reportable uniformity in the approach to deceased donation. Transplant Int 2011; 24: 373-8.
Souter MJ, Blissitt PA, Blosser S, et al. Recommendations for the critical care management of devastating brain injury: prognostication, psychosocial, and ethical management: a position statement for healthcare professionals form the Neurocritical Care Society. Neurocrit Care 2015; 23: 4-13.
de la Rosa G, Domínguez-Gil B, Matesanz R, et al. Continuously evaluating performance in deceased donation: the Spanish Quality Assurance Program. Am J Transplant 2012; 12: 2507-13.
Sheehy E, O’Connor KJ, Luskin RS, et al. Investigating geographic variation in mortality in the context of organ donation. Am J Transplant 2012; 12: 1598-602.
Sheehy E, Conrad SL, Brigham LE, et al. Estimating the number of potential organ donors in the United States. N Engl J Med 2003; 349: 667-74.
Nair R, Aggarwal R, Khanna D. Methods of formal consensus in classification/diagnostic criteria and guideline development. Semin Arthritis Rheum 2011; 41: 95-105.
Canadian Blood Services. Data, Analytics and Reporting System Workshop. Canadian Blood Services, 2013. Available from URL: https://professionaleducation.blood.ca/sites/msi/files/CBS-Jun-2013-Data-Workshop-Report_Final.pdf (accessed October 2018).
Annual report. Australian Organ and Tissue Donation and Transplantation Authority, 2013-2014. Available from URL: https://www.health.gov.au/internet/budget/publishing.nsf/Content/2013-2014_Health_PBS_sup2/$File/2013-14_DoHA_PBS_4.05_AOTDTA.pdf (accessed October 2018).
Conflicts of interest
All members of the working groups declare that they have no conflicts of interest.
Editorial responsibility
This submission was handled by Dr. Gregory L. Bryson, Deputy Editor-in-Chief, Canadian Journal of Anesthesia.
Author contributions
All authors contributed substantially to all aspects of this manuscript, including conception and design; acquisition, analysis, and interpretation of data; and drafting the article.
Funding
The Deceased Donation Data Working Group was convened by Canadian Blood Services, which also provided funding for the meetings of the working group. Members of the Deceased Donation Working Group included representatives of the Canadian Blood Services, but the Canadian Blood Services had no role in the developing the final recommendations of this report.
Disclosure
Dr. D. Jim Kutsogiannis was paid by Alberta Health Services as the human organ procurement and exchange (HOPE) Northern Alberta Medical Director.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hornby, K., Shemie, S.D., Appleby, A. et al. Development of a national minimum data set to monitor deceased organ donation performance in Canada. Can J Anesth/J Can Anesth 66, 422–431 (2019). https://doi.org/10.1007/s12630-018-01290-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-018-01290-8