
Abstract
Purpose
This review evaluates the current and future role of cardiopulmonary exercise testing (CPET) in the context of Enhanced Recovery After Surgery (ERAS) programs.
Principal findings
There is substantial literature confirming the relationship between physical fitness and perioperative outcome in general. The few small studies in patients undergoing surgery within an ERAS program describe less fit individuals having a greater incidence of morbidity and mortality. There is evidence of increasing adoption of perioperative CPET, particularly in the UK. Although CPET-derived variables have been used to guide clinical decisions about choice of surgical procedure and level of perioperative care as well as to screen for uncommon comorbidities, the ability of CPET-derived variables to guide therapy and thereby improve outcome remains uncertain. Recent studies have reported a reduction in CPET-defined physical fitness following neoadjuvant therapies (chemo- and radio-therapy) prior to surgery. Preliminary data suggest that this effect may be associated with an adverse effect on clinical outcomes in less fit patients. Early reports suggest that CPET-derived variables can be used to guide the prescription of exercise training interventions and thereby improve physical fitness in patients prior to surgery (i.e., prehabilitation). The impact of such interventions on clinical outcomes remains uncertain.
Conclusions
Perioperative CPET is finding an increasing spectrum of roles, including risk evaluation, collaborative decision-making, personalized care, monitoring interventions, and guiding prescription of prehabilitation. These indications are potentially of importance to patients having surgery within an ERAS program, but there are currently few publications specific to CPET in the context of ERAS programs.
Résumé
Objectif
Cette étude évalue le rôle actuel et dans le futur des tests d’efforts cardiopulmonaires (CPET) dans le contexte des programmes de récupération rapide après la chirurgie (RRAC).
Constatations principales
Il existe une abondante littérature confirmant les rapports entre la forme physique et l’évolution générale du patient en période périopératoire. Les quelques petites études menées avec des patients subissant une chirurgie dans un programme de RRAC indiquent que les individus les moins en forme ont une plus grande incidence de morbidité et mortalité. Il existe des données probantes sur l’adoption croissante du CPET périopératoire, en particulier au Royaume-Uni. Bien que des variables tirées du CPET aient été utilisées pour guider les décisions cliniques sur le choix de la procédure chirurgicale et le niveau de soins périopératoires, ainsi que pour dépister des comorbidités rares, la capacité des variables tirées du CPET pour guider le traitement et, par conséquent, améliorer ses résultats reste incertaine. Des études récentes ont décrit une baisse de la forme physique (définie par le CPET) après des traitements néoadjuvants (chimio et radiothérapie) précédant une intervention chirurgicale. Les données préliminaires suggèrent que cela peut être associé à un effet secondaire sur les résultats cliniques des patients ayant la moins bonne condition physique. De premiers rapports suggèrent que les variables tirées du CPET peuvent être utilisées pour guider la prescription d’interventions d’entraînement à l’effort et, par conséquent, améliorer leur condition physique avant la chirurgie (c’est-à-dire, préadaptation). L’impact de telles interventions sur les résultats cliniques reste incertain.
Conclusions
Le CPET périopératoire connaît une plage croissante d’utilisations, notamment pour l’évaluation du risque, la prise de décision collaborative, les soins personnalisés, l’évaluation du bénéfice des interventions et le guidage de la prescription de préadaptation. Ces indications sont potentiellement importantes pour les patients devant subir une chirurgie dans le cadre d’un programme de RRAC, mais il n’y a actuellement que peu de publications portant spécifiquement sur le CPET dans le contexte de programmes de RRAC.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Cardiopulmonary exercise testing (CPET) has an established role in the evaluation of perioperative risk in a range of types of surgery. Early work focused on heart transplant and lung resection surgery.1-3 Recently, the majority of studies have focused on major intra-abdominal surgery.4-7 The way in which data derived from CPET have been used has evolved over time. Initially, the focus was on guiding clinician decisions about whether to undertake surgery and where to care for patients following surgery (intensive care unit [ICU] or general ward) as well as identifying previously unsuspected comorbidity. Over time, the focus has broadened to encompass contributing to collaborative decision-making between patients and clinicians,8 evaluating the consequences of neoadjuvant therapies (including chemo- and radio-therapy), and guiding prehabilitation (prehab) programs.
Enhanced Recovery after Surgery (ERAS) programs have evolved over the past two decades from an enthusiast-led clinical innovation9 to national implementation.10 A typical ERAS care pathway incorporates pre- intra- and postoperative elements, and implementation of such pathways has been shown to reduce duration of hospital stay with no increase in readmission rate.11 The relative contribution of each element to the observed benefit is, in general, uncertain. Early mobilization and feeding are the elements most consistently associated with reduced hospital stay.11 Overall, increased adherence to ERAS elements seems to be associated with reduced length of stay.11 Key preoperative elements include careful evaluation of risk and management of patient expectations. Cardiopulmonary exercise testing has the potential to contribute to these elements as well as to evaluate the consequences of novel perioperative interventions of relevance to patients within ERAS programs, including anti-cancer treatments (e.g., neoadjuvant chemotherapy) and exercise training (prehab).
The aim of this article is to explore the role of CPET and prehab in patients undergoing surgery within an ERAS program. To achieve this aim, we conducted two systematic searches of Ovid MEDLINE® (1946-present, including in-process and daily update). To identify studies addressing ERAS, we used the search terms “enhanced recovery” or “ERAS” or “fast track” and “surgery”.11 To identify studies using CPET in the context of ERAS, this ERAS search was combined with the search terms “CPET” or “CPX” or “cardiopulmonary exercise testing” or “exercise testing” or “CPEX” or “\(\dot V{O_2}max\)” and “surgery”.12 To identify studies using prehab in the context of ERAS, this ERAS search was combined with the search terms “prehabilitation” or “prehab” or “exercise training” or “training” or “exercise therapy” or “exercise program” or “exercise intervention” or “physical training”.13
The search of CPET in ERAS identified one consensus statement in the British Medical Journal discussing the potential benefit of CPET in preoperative assessment for ERAS but no primary reports of studies.14 The search of prehabilitation in ERAS programs identified two narrative reviews15,16 but no specific studies. Some recent studies from the UK (including from our own group)17,18 evaluate CPET within the context of an ERAS program but do not explicitly report that patient care was ERAS-based. This has occurred, in part, as a consequence of the national implementation of the Enhanced Recovery Partnership Program10,14 within the National Health Service (NHS) in the UK from 2009 to 2011, which resulted in widespread adoption of ERAS programs across most NHS trusts for a range of common elective surgeries (colorectal, urology, gynecology, lower limb joint replacements).
Given the paucity of primary clinical studies in the context of ERAS, we subsequently conducted a secondary search to explore the roles of CPET and prehabilitation in patients undergoing surgery irrespective of whether this was in the context of an ERAS program. Where examples from ERAS are available, we have highlighted this; however, much of the content of this review is based on extrapolating from the surgical literature in general. To give context to this literature, we have added an introductory section summarizing the substantial general literature exploring the relationship between physical fitness, physical exercise, and health outcomes as well as describing the physiology and conduct of CPET.
Physical activity, exercise, and health outcomes
There is a large body of evidence supporting the notion that physical fitness has benefits in almost every context of health and disease19,20 and, furthermore, that physical inactivity is one of the leading public health issues facing our generation.21,22 For example, better outcomes for fitter or more active patients have been documented in coronary artery disease,23,24 heart failure,25-27 hypertension,28 diabetes,29,30 chronic obstructive pulmonary disease (COPD),31 depression,32 dementia,33 chronic kidney disease,34 cancer,35 and stroke.36,37 It has also been shown that physical activity reduces the risk of chronic diseases, including type 2 diabetes,38 osteoporosis,39 obesity,40 depression,41 and cancer of the breast,42 kidney,43 and colon.24 Although the instantaneous risk of death may be increased during physical activity or training,23,44 the cumulative benefit of regular physical activity and/or exercise outweighs this relatively short-lived period of elevated risk.24
Such data raise the obvious hypothesis: can health outcomes be improved by intervening to improve physical fitness? Where data are available, it is generally true that public health promotion of physical activity is effective.45 Moreover, exercise interventions in the form of supervised and unsupervised training programs have been shown to be beneficial in a variety of conditions, including COPD, stroke, heart failure, and intermittent claudication,46-50 although the long-term benefits of such interventions are less well evaluated.
Perioperative cardiopulmonary exercise testing
Cardiopulmonary exercise testing provides an objective method of evaluating exercise capacity (functional reserve or physical fitness). Furthermore, it allows interrogation of the causes of exercise intolerance when exercise capacity is reduced. Cardiopulmonary exercise testing integrates expired gas analysis (oxygen and carbon dioxide concentrations) with the measurement of ventilatory flow, thereby enabling calculation of oxygen uptake (\(\dot V{O_2}\)) and carbon dioxide production (\(\dot VC{O_2}\)) under conditions of varying physiological stress imposed by a range of defined external workloads. Heart rate, oxygen saturations, blood pressure, and electrocardiogram can also be monitored simultaneously with expired gas analysis. Thus, CPET provides a global assessment of the integrated responses of the pulmonary, cardiovascular, hematological, and metabolic systems that are not adequately reflected through measuring how individual organ systems function at rest.51
The modes of exercise commonly employed in CPET include cycle ergometry and treadmill, while arm crank ergometry is used occasionally. In the perioperative setting, most groups have utilized cycle ergometry, and this has several advantages over the treadmill. Most importantly, cycle ergometry allows accurate determination of the external work rate and thus evaluation of the \(\dot V{O_2}\)-work rate relationship, which is difficult with a treadmill. In addition, cycle ergometry also requires less skill than a treadmill (i.e., performance is consequently less affected by practice); it is cheaper and takes up less space.52
A variety of exercise protocols can be used during CPET (e.g., incremental tests, constant work rate tests) in order to interrogate different elements of the exercise response. In the perioperative context, the continuous incremental exercise test (incremental ramp test) to the limit of tolerance (symptom limited) has been used most widely.53 The advantages of this exercise protocol are as follows:
-
1.
It evaluates the exercise response across the entire range of functional capacity.
-
2.
It allows assessment of the normalcy or otherwise of the exercise response.
-
3.
It permits identification of the site of functional exercise limitation.
-
4.
It gives an appropriate frame of reference for training or rehabilitation targets.
-
5.
The initial work rate is low and there is a short duration of high intensity exercise.
-
6.
The entire protocol is of short duration – eight to twelve minutes of exercise.
A typical test profile includes three minutes of resting measurement, followed by three minutes of unloaded cycling (cycling against no resistance), and then a continuously increasing ramp until exhaustion. The gradient of the ramp is selected to achieve a test duration of eight to twelve minutes. In addition, gas exchange data may be collected in recovery, typically for five minutes.
In the early days of perioperative CPET, some groups initially stopped tests above the anaerobic threshold (AT) but before symptom limitation because of safety concerns in this previously unevaluated population.4,6 Nevertheless, subsequent review of the safety studies of CPET has revealed a mortality rate of approximately two to five per 100,000 in patient populations that include patients undergoing lung and heart transplant.51,54 Consequently, symptom limited tests are now most commonly employed.
The measurements made during an incremental exercise test are summarized in Table 1. The output from incremental CPET is by convention represented graphically in a nine-panel plot.51,52 Exercise capacity can be evaluated and causes of exercise limitation can be identified as patterns of abnormality in these plots.
Exercise capacity (functional capacity or physical fitness) can be described by the AT and \(\dot V{O_2}peak.\)These variables are metabolic rates that are expressed in millilitres of \(\dot V{O_2}\) per minute absolute, or indexed to bodyweight, or as percentages of predicted values. The term \(\dot V{O_2}peak\) is defined as the highest oxygen uptake recorded during an incremental exercise test at the point of symptom limitation. The anaerobic threshold (also known as the lactate threshold, ventilatory threshold, gas exchange threshold, or lactic acidosis threshold) is considered to be a descriptor of exercise capacity that characterizes the upper limits of exercise intensities that can be accomplished almost wholly aerobically.51 Below the AT, exercise can be sustained almost indefinitely, whereas above the AT, progressive increases in work rate result in progressive reductions in exercise tolerance.55 The AT is defined as the \(\dot V{O_2}\) at which there is a transition from a phase of no increase, or only a small increase in arterial [lactate], to a phase of rapidly accelerating increase in arterial [lactate] associated with a progressive metabolic acidosis.56 This point can be estimated noninvasively by breath-by-breath expired gas analysis during CPET.57 The onset of metabolic acidosis at the AT is accompanied by a rise in the pulmonary CO2 output (\(\dot VC{O_2}\)) resulting from the intramuscular and blood buffering by bicarbonate of lactate-associated protons.58,59 This can be identified during incremental exercise testing as a change in the gradient of the \(\dot VC{O_2}\)-\(\dot V{O_2}\) relationship (V-slope method57 or modified V-slope method),60 typically accompanied by a systematic rise in the ventilatory equivalent for oxygen (\(\dot V\) E/\(\dot V{O_2}\)) and in end-tidal PO2 (PETO2) without a concomitant decrease in end-tidal PCO2 (PETCO2) or increase in the ventilatory equivalent for CO2 (\(\dot V\) E/\(\dot VC{O_2}\)) (ventilatory equivalents method).61 Several investigators have shown that these indirect approaches provide a valid estimate of the lactic acid threshold (LaT) both in healthy volunteers and in patients with cardiac disease and COPD.62-65
The ratio of ventilation \(\dot V\) E to \(\dot V{O_2}\) is the ventilatory equivalent for oxygen (\(\dot V\) E/\(\dot V{O_2}\)), and the ratio of \(\dot V\) E to \(\dot VC{O_2}\) is the ventilatory equivalent for carbon dioxide (\(\dot V\) E/\(\dot VC{O_2}\)). The ventilatory equivalents for both \({{\text{O}}_2}\) and \({\text{C}}{{\text{O}}_2}\) are related to the ratio of pulmonary dead space to tidal volume (Vd/Vt) and increase as dead space increases (although they also increase with hyperventilation). Abnormally high ventilatory equivalents are thus evident in any pathological condition with increased dead space, e.g., COPD, pulmonary fibrosis, heart failure, and pulmonary embolic disease.
In summary, the incremental exercise test to the limit of tolerance using cycle ergometry (incremental ramp test) has been used extensively in both clinical practice and clinical trials. It permits the accurate determination of exercise capacity and also allows the identification of the site of exercise limitation when this is abnormal. The AT and \(\dot V{O_2}peak,\)which are determined from this test, are validated measures of exercise capacity and are the appropriate variables to use to describe physical fitness in clinical practice and research trials. The efficacy of exercise training programs (prehab or otherwise) can be evaluated using the incremental exercise test. Effective training would be expected to cause an increase in the AT and/or \(\dot V{O_2}peak.\)These variables can be measured reliably and can thus be used to compare patient groups from different clinical centres and compare outcomes in clinical trials.
Cardiopulmonary exercise testing-derived variables and perioperative outcomes
The hypothesis that unfit patients are more susceptible to adverse outcomes following major surgery is intuitively appealing and implicit in many aspects of preoperative assessment. For example, the ability to climb stairs or walk to the local shops is often used as a clinical indicator of functional capacity during preoperative assessment. During the late 1980s and early 1990s, Paul Older et al. in Melbourne, Australia published novel research using CPET in preoperative assessment. In 1993, they reported preoperative CPET data on 184 patients undergoing elective major surgery and reported that a lower AT was associated with elevated mortality following surgery.66 To date, 24 cohort studies (including over 4,000 patients) have reported the relationship between preoperative CPET-derived variables and postoperative outcome (see Table 2 for details). These data have been brought together in several systematic reviews12,67,68 that, in summary, show a remarkably consistent relationship between physical fitness – defined using CPET-derived variables – and postoperative outcome. The few studies that do not find a statistically significant relationship are small and underpowered. Indeed, all studies evaluating more than 100 patients report a statistically significant relationship with outcome. A limitation of this literature is the fact that, in most studies, clinicians were not blinded to the CPET results and so used them to make clinical decisions such as the elective utilization of critical care facilities. This confounding by indication introduces uncertainty as to the true strength of the relationship between fitness and surgical outcome.69 The effect of such confounding would be to reduce the strength of association reported in the literature, since clinicians would be likely to respond to high-risk tests by instituting management to reduce risk, thereby diluting the strength of the association between risk and outcome. The limited available blinded data5,18 reports a stronger association between risk and outcome than the potentially confounded data6 supporting the notion of confounding by indication. An additional value of CPET that is less amenable to evaluation in clinical trials is the opportunity to identify unsuspected comorbidities such as ischemic heart disease (e.g., a flat oxygen pulse, electrocardiogram changes or arrhythmias,66,70 and pulmonary hypertension, which we have correctly identified in a handful of cases in our own practice).71-73
The use of CPET in the perioperative setting has increased rapidly in the UK over the last decade. Survey data from the UK suggest that the number of hospitals using CPET for evaluation of perioperative risk has risen from 17% in 200874 to 32% in 2011,75 and anecdotally, it is probably 40-50% in 2014. In general, perioperative CPET tests were requested by surgeons or anesthetists and conducted by anesthetists, but clinical arrangements varied across institutions. Adoption in other countries is not documented, but anecdotally, it is at a much lower level then in the UK.
Complex risk stratification
Recent data have extended previous work in a number of ways, including the use of multiple CPET-derived variables to construct predictive models, exploration of the prediction of longer-term outcomes, as well as the comparison and combination of CPET with other candidate risk predictors.
Colson et al. reported data on 1,725 patients undergoing elective major surgery in a single institution in Australia with 36% mortality in this cohort at five years. While no single variable was significantly predictive of long-term outcome, a model incorporating four physiological variables measured at the AT predicted five-year mortality.76 These data are intriguing because of both the prediction of a longer-term mortality and the use of a multivariable approach. It is unclear whether this model will be generalizable to other settings.
Carlisle et al. showed improved prediction of mortality following abdominal aortic aneurysm surgery when CPET-derived variables were used in combination with a clinical risk score, i.e., the revised cardiac risk index (“Lee score”), in comparison with CPET variables alone.77 James et al. showed better prediction of major adverse cardiac events and all complications using CPET-derived variables when compared with plasma biomarkers.78 They did not evaluate the performance of the different variables used in combination.
Using risk information
The majority of the perioperative CPET literature has focused on the use of CPET-derived information to guide clinicians’ decision-making. This has included choice of procedure and perioperative care environment. Patients defined as high-risk for adverse outcomes following surgery may be scheduled for less physiologically challenging procedures. For example, a defunctioning colostomy and palliative resection may be chosen instead of a more definitive tumour resection. The rationale for this approach is that the balance between risk and benefit for the procedure is specific to an individual, and the risks of major procedures for patients with the highest level of risk may outweigh any possible benefits. More commonly, CPET data have been used to guide the choice of postoperative care.4 In the context of enhanced recovery where the focus is on early mobilization and rapid normalization of physiological function, this may be viewed from the converse perspective of identifying low-risk patients who are safe to triage to enhanced recovery care on a normal ward.
Cardiopulmonary exercise testing-guided postoperative care
Following their original study,66 Older et al. suggested that CPET data might be useful to guide decisions about the choice of postoperative care environment, with less fit patients being allocated to an intensive care environment following surgery.4 In a subsequent prospective study, the same group used CPET-derived variables (AT, ventilatory equivalents for oxygen, myocardial ischemia) along with the magnitude of surgery to allocate patients to intensive care, high dependency care, and ward care.4 None of the patients allocated to ward care died from “cardiovascular” causes, and mortality in the high dependency unit and in the ICU was lower than historical control data from the same institution. This study is limited by the non-randomized design and historical control data and by the risk of bias in attributing the criteria for “cardiovascular” death (all-cause mortality was not reported).
While Older’s 1999 interventional study had several limitations and therefore falls short of meeting modern criteria for showing a causal link between the intervention (postoperative care allocated by CPET-derived variables) and outcome (postoperative morbidity and mortality), the results are provocative and merit further investigation. A pilot double-blind randomized controlled trial (RCT) evaluating this has recently been completed in the UK. The study enrolled 228 patients undergoing elective colorectal cancer surgery within an ERAS program, and results are expected early in 2015.79 Further studies exploring the impact of CPET-guided intervention on outcome are needed, but the complexity of evaluating such a multifaceted intervention have so far limited the number of investigators who have taken on this challenge. While the literature is replete with manuscripts describing the association between various preoperative markers of risk and outcome, there is a lack of studies evaluating their implementation using an experimental design.
Neoadjuvant therapy, physical fitness, and outcome following surgery
Neoadjuvant therapy using chemotherapy (NAC) or chemoradiotherapy (NACRT) is increasingly common before major cancer surgery. The aim of this therapy is to reduce tumour bulk prior to surgery and thereby increase the likelihood of complete (or optimal) tumour clearance and improve long-term outcome. Neoadjuvant therapy using chemotherapy/NACRT is widely used in surgery for gastric and esophageal cancer80 and for rectal cancer81 as well as for breast,82 urology,83 lung84 and other tumour types.
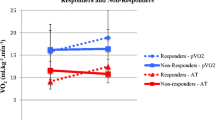
Two recently published studies explored the impact of neoadjuvant therapy on physical fitness prior to major surgery. The first study evaluated the effect of NAC on 89 patients with oesophageal or gastric cancer. Following NAC, CPET-measured oxygen consumption was reduced at the AT and peak exercise, and lower baseline values for these variables were associated with increased one-year mortality in patients who completed a full course of NAC and underwent surgery.85 A subsequent study in 25 patients undergoing NACRT prior to rectal cancer surgery within an ERAS program reported similar results, with a fall in oxygen consumption variables following NACRT but no effect on mortality.86
It is currently unknown if the effects of neoadjuvant immune therapies87 on physical fitness are similar to those of NAC and NACRT.
Prehabilitation: exercise training before a physiological challenge
Prehabilitation is defined as “the process of enhancing the functional capacity of the individual to enable him or her to withstand a stressful event”.88,89 Physical exercise training prior to elective surgery meets this criterion. It is well documented that exercise training is feasible and safe in patients with a spectrum of severe cardiac and pulmonary disease. For example, physical exercise programmes have been demonstrated to improve physical fitness and clinical outcomes in patients with cardiac failure,47 ischemic heart disease,90,91 and COPD50. Furthermore, patients on a screening program for abdominal aortic aneurysm have been shown to improve their physical fitness following a moderate intensity exercise intervention scheduled three times per week.92
In 2013, a systematic review of RCTs of aerobic exercise training in elective intracavity surgery identified ten studies with a total of 524 participants.13 Most of the eligible publications reported small single-centre studies describing feasibility and training efficacy. One eligible study reported a significant difference in outcome. Arthur et al. conducted an RCT of 246 patients undergoing cardiac surgery and reported a one-day reduction in ICU and hospital length of stay in the intervention group despite finding no difference in exercise capacity between the groups after eight weeks of aerobic interval training.93
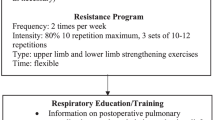
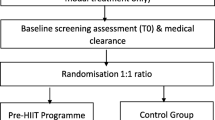
Preliminary non-randomized data from patients undergoing elective colorectal cancer surgery within an ERAS program have shown the feasibility of providing a CPET-guided structured responsive interval training program that is delivered three times a week for six weeks in a hospital setting after neoadjuvant chemoradiotherapy and before surgery.17 The control population was made up of patients unable to engage with the exercise program for logistical reasons (e.g., distance of residence from the hospital). A follow-on randomized study is currently evaluating the efficacy of a CPET-guided structured responsive training program in maintaining physical fitness after neoadjuvant chemoradiotherapy. The study population are patients scheduled to undergo elective rectal cancer surgery within an ERAS program.94 Importantly, the neoadjuvant therapies, which are typically administered as a course of therapy some weeks prior to surgery and followed by a recovery period of six to 12 weeks or more, have opened up a time window to train patients prior to major cancer operations where previously the pressure of reducing the time between diagnosis and surgery precluded such an intervention.
Future directions
A number of opportunities are developing in perioperative CPET, including increasingly sophisticated risk prediction, collaborative decision-making, personalized medicine, and targeted exercise interventions.
Risk prediction
Increasingly sophisticated risk prediction may be achieved by using variables from CPET in combination with other sources of data, such as clinical risk scores and plasma biomarkers. In general, added predictive value would be expected from unrelated but effective tests, and the very limited available data are supportive of this notion.5,77 Furthermore, it seems likely that there will be an evolution towards developing a hierarchy of tests to describe risk. For example, simple clinical risk scores and screening biomarkers may be used to screen out low-risk patients at low cost. The remaining patients would, by definition, be of uncertain or high risk and could be evaluated by a more complex battery of tests so as to define their risk more precisely and to identify specific limiting factors. Cardiopulmonary exercise testing is likely to be of great value in the second stage of this process.
Collaborative decision-making
Increasing recognition of the issue of “provider bias”, whereby patients tend to be offered surgery more often when surgical capacity is generous in their local area, along with a cultural swing towards patient empowerment have driven the shared or collaborative decision-making agenda. Rather than being used simply to guide a clinician’s choice of care, risk data are now used to contribute to a discussion between patient and clinician about the best course of action for that patient. The aim of collaborative decision-making is to provide patients with sufficient information to allow them to decide on the most appropriate course of treatment for their circumstances. Cardiopulmonary exercise testing is of value in this process because it provides risk information in a way that is intuitively easy to comprehend – the idea of “fitness for surgery” is a good basis for a discussion about the specific risks and benefits of a particular procedure for a particular patient.
Evaluating perioperative therapies
The effect of neoadjuvant chemotherapy and chemoradiotherapy on physical fitness and the consequent adverse impact of these interventions on clinical outcomes in less fit patients are likely to become of increasing importance. Surgery for cancer, in particular, is now commonly part of a complex set of interventions (e.g., NAC, NACRT, immunotherapy) directed against the underlying pathology. The complex interactions between these interventions are likely to alter the risk-benefit equation for each treatment element for each patient. In addition to the areas already highlighted in this review, the impact of immunotherapies on physical fitness is unknown. Furthermore, the effect of surgery on physical fitness and the pattern of recovery postoperatively may be of importance in the choice and timing of adjuvant therapies. Cardiopulmonary exercise testing is a candidate technology for evaluating the effects of adjuvant therapies in isolation or in combination on physical fitness, specifically identifying exercise limitation caused by organ-specific harm.
Personalized medicine
Many of these themes are drawn together under the heading of personalized or individualized medicine, i.e., the concept of giving the right treatment to the right patient at the right time. The contribution of CPET to the evaluation of perioperative risk is one example of this – tailoring the choice of procedure and the perioperative care to the individual patient’s risk. More sophisticated uses for CPET may arise around neoadjuvant cancer therapies. Variability in tumour response to treatment is potentially amenable to prediction using information such as tumour genome sequencing. Weighing such information against CPET-derived data assessing the risk that neoadjuvant therapy will adversely impact physical fitness, it might be possible to assess the likelihood of benefit and harm from a specific neoadjuvant treatment for individual patients. This information could be used to guide therapy, including the selection of chemotherapy, the timing of chemotherapy in relation to surgery, and the choice of an appropriate prehabilitation program.
Exercise interventions
The use of CPET to define exercise training programs has already been shown in a number of fields. It is likely that such interventions will become increasingly sophisticated. Prehabilitation approaches include endurance and strength training, so-called high-intensity training schedules, and the use of nutritional and pharmaceutical adjunctive therapies to improve the efficacy of training stimuli. Improved understanding of the optimal duration, pattern, intensity, and qualities of such interventions will be needed to maximize efficacy. In order to maximize the effectiveness of training, we need a better understanding of the complex interplay between adherence, efficacy, and cost for in-hospital supervised training interventions vs self-directed outpatient approaches.
Future clinical trials
While there is extensive evidence that exercise capacity predicts adverse postoperative outcome, the case for intervening to improve outcome on the basis of exercise capacity is currently less clear. Further clinical trials are required to evaluate the two most commonly promoted clinical approaches based on exercise capacity data:
-
1.
Altering the location and type of perioperative care to reduce the risk of complications.
-
2.
Exercise training programs to improve exercise capacity prior to surgery – prehabilitation.
Trials are required: first, to establish that training programs are effective in the surgical population and, second, to ascertain that improved fitness translates to improved outcome. Interrogation of the clinical trials database identified 29 trials evaluating exercise testing in surgical patients.95 The result of one RCT evaluating the utility of CPET to direct perioperative care is expected imminently.79 Twenty ongoing clinical trials are currently evaluating the effect of prehabilitation training interventions in a variety of surgical specialties, including colorectal (seven trials), upper gastrointestinal (three trials), and bariatric patients (one trial), abdominal aortic aneurysm (one trial) urology (three trials), orthopedic (one trial), and liver patients (two trials), general abdominal (one trial), and coronary artery bypass grafting patients (one trial). Thus, substantial new data should be forthcoming in the near future.
Conclusions
While there is limited literature specific to CPET and ERAS, the available data are consistent with the wider literature on CPET and major surgery. Reduced physical fitness (as defined by CPET variables) is associated with an increased incidence of postoperative morbidity and mortality. Information derived from CPET has been used to guide both the choice of surgical procedure and the postoperative care environment. Cardiopulmonary exercise testing may also identify unsuspected comorbidities.
Recent developments include the increasing importance of collaborative/shared decision-making, recognition of the adverse impact of neoadjuvant therapies on physical fitness (and possibly clinical outcome), and CPET-guided prehabilitation.
Looking forward, CPET may have a role in increasing the sophistication of the evaluation of preoperative risk (hierarchical multivariable approach), in evaluating the impact of a spectrum of neoadjuvant therapies, and in guiding multimodal prehabilitation interventions.
References
Benzo R, Kelley GA, Recchi L, Hofman A, Sciurba F. Complications of lung resection and exercise capacity: a meta-analysis. Respir Med 2007; 101: 1790-7.
Osada N, Chaitman BR, Miller LW, et al. Cardiopulmonary exercise testing identifies low risk patients with heart failure and severely impaired exercise capacity considered for heart transplantation. J Am Coll Cardiol 1998; 31: 577-82.
Ong KC, Benedicto JP, Chan AH, Tan YS, Ong YY. Cardiopulmonary exercise testing in heart transplant candidates. Ann Acad Med Singapore 2000; 29: 442-6.
Older P, Hall A, Hader R. Cardiopulmonary exercise testing as a screening test for perioperative management of major surgery in the elderly. Chest 1999; 116: 355-62.
Snowden CP, Prentis JM, Anderson HL, et al. Submaximal cardiopulmonary exercise testing predicts complications and hospital length of stay in patients undergoing major elective surgery. Ann Surg 2010; 251: 535-41.
Wilson RJ, Davies S, Yates D, Redman J, Stone M. Impaired functional capacity is associated with all-cause mortality after major elective intra-abdominal surgery. Br J Anaesth 2010; 105: 297-303.
Hennis PJ, Meale PM, Hurst RA, et al. Cardiopulmonary exercise testing predicts postoperative outcome in patients undergoing gastric bypass surgery. Br J Anaesth 2012; 109: 566-71.
Glance LG, Osler TM, Neuman MD. Redesigning surgical decision making for high-risk patients. N Engl J Med 2014; 370: 1379-81.
Bardram L, Funch-Jensen P, Jensen P, Crawford ME, Kehlet H. Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobilisation. Lancet 1995; 345: 763-4.
DH, NHS Improvement, NCAT, NHS Institute. Enhanced Recovery Partnership Programme – Report March 2011. Available from URL: https://www.gov.uk/government/publications/enhanced-recovery-partnership-programme (accessed September 2014).
Grocott MP, Martin DS, Mythen MG. Enhanced recovery pathways as a way to reduce surgical morbidity. Curr Opin Crit Care 2012; 18: 385-92.
Hennis PJ, Meale PM, Grocott MP. Cardiopulmonary exercise testing for the evaluation of perioperative risk in non-cardiopulmonary surgery. Postgrad Med J 2011; 87: 550-7.
O’Doherty AF, West M, Jack S, Grocott MP. Preoperative aerobic exercise training in elective intra-cavity surgery: a systematic review. Br J Anaesth 2013; 110: 679-89.
Knott A, Pathak S, McGrath JS, et al. Consensus views on implementation and measurement of enhanced recovery after surgery in England: Delphi study. BMJ Open 2012; DOI:10.1136/bmjopen-2012-001878.
Baldini G, Carli F. Anesthetic and adjunctive drugs for fast-track surgery. Current Drug Targets 2009; 10: 667-86.
Hoogeboom TJ, Dronkers JJ, Hulzebos EH, van Meeteren NL. Merits of exercise therapy before and after major surgery. Curr Opin Anaesthesiol 2014; 27: 161-6.
West MA, Lythgoe D, Barben CP, et al. Cardiopulmonary exercise variables are associated with postoperative morbidity after major colonic surgery: a prospective blinded observational study. Br J Anaesth 2014; 112: 665-71.
West MA, Parry MG, Lythgoe D, et al. Cardiopulmonary exercise testing for the prediction of morbidity risk after rectal cancer surgery. Br J Surg 2014; 9: 1166-72.
Fiuza-Luces C, Garatachea N, Berger NA, Lucia A. Exercise is the real polypill. Physiology (Bethesda) 2013; 28: 330-58.
Sallis RE. Exercise is medicine and physicians need to prescribe it! Br J Sports Med 2009; 43: 3-4.
Kohl HW 3rd, Craig CL, Lambert EV, et al. The pandemic of physical inactivity: global action for public health. Lancet 2012; 380: 294-305.
Lee IM, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012; 380: 219-29.
Thompson PD, Franklin BA, Balady GJ, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation 2007; 115: 2358-68.
Thompson PD, Buchner D, Pina IL, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation 2003; 107: 3109-16.
Belardinelli R, Georgiou D, Cianci G, Purcaro A. Randomized, controlled trial of long-term moderate exercise training in chronic heart failure: effects on functional capacity, quality of life, and clinical outcome. Circulation 1999; 99: 1173-82.
O’Connor CM, Whellan DJ, Lee KL, et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009; 301: 1439-50.
Mandic S, Myers J, Selig SE, Levinger I. Resistance versus aerobic exercise training in chronic heart failure. Curr Heart Fail Rep 2012; 9: 57-64.
Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc 2013; 2: e004473.
Thomas DE, Elliott EJ, Naughton GA. Exercise for type 2 diabetes mellitus. Cochrane Database Syst Rev 2006; 3: CD002968.
Hayashino Y, Jackson JL, Fukumori N, Nakamura F, Fukuhara S. Effects of supervised exercise on lipid profiles and blood pressure control in people with type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Diabetes Res Clin Pract 2012; 98: 349-60.
Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest 2011; 140: 331-42.
Cooney GM, Dwan K, Greig CA, et al. Exercise for depression. Cochrane Database Syst Rev 2013; 9: CD004366.
Forbes D, Thiessen EJ, Blake CM, Forbes SC, Forbes S. Exercise programs for people with dementia. Cochrane Database Syst Rev 2013; 12: CD006489.
Heiwe S, Jacobson SH. Exercise training for adults with chronic kidney disease. Cochrane Database Syst Rev 2013; 10: CD003236.
Des Guetz G, Uzzan B, Bouillet T, et al. Impact of physical activity on cancer-specific and overall survival of patients with colorectal cancer. Gastroenterol Res Pract 2013; 2013: 340851.
Saunders DH, Sanderson M, Brazzelli M, Greig CA, Mead GE. Physical fitness training for stroke patients. Cochrane Database Syst Rev 2013; 10: CD003316.
Austin MW, Ploughman M, Glynn L, Corbett D. Aerobic exercise effects on neuroprotection and brain repair following stroke: a systematic review and perspective. Neurosci Res 2014; DOI:10.1016/j.neures.2014.06.007.
Hopper I, Billah B, Skiba M, Krum H. Prevention of diabetes and reduction in major cardiovascular events in studies of subjects with prediabetes: meta-analysis of randomised controlled clinical trials. Eur J Cardiovasc Prev Rehabil 2011; 18: 813-23.
Howe TE, Shea B, Dawson LJ, et al. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst Rev 2011; 7: CD000333.
Tate DF, Jeffery RW, Sherwood NE, Wing RR. Long-term weight losses associated with prescription of higher physical activity goals. Are higher levels of physical activity protective against weight regain? Am J Clin Nutr 2007; 85: 954-9.
Mammen G, Faulkner G. Physical activity and the prevention of depression: a systematic review of prospective studies. Am J Prevent Med 2013; 45: 649-57.
Friedenreich CM. Physical activity and breast cancer: review of the epidemiologic evidence and biologic mechanisms. Recent Results Cancer Res 2011; 188: 125-39.
Behrens G, Leitzmann MF. The association between physical activity and renal cancer: systematic review and meta-analysis. Br J Cancer 2013; 108: 798-811.
De Backer G, Ambrosioni E, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of eight societies and by invited experts). Eur J Cardiovasc Prev Rehabil 2003; 10: S1-10.
Heath GW, Parra DC, Sarmiento OL, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet 2012; 380: 272-81.
Lane R, Ellis B, Watson L, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev 2014; 7: CD000990.
Taylor RS, Sagar VA, Davies EJ, et al. Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev 2014; 4: CD003331.
Mehrholz J, Pohl M, Elsner B. Treadmill training and body weight support for walking after stroke. Cochrane Database Syst Rev 2014; 1: CD002840.
Carson KV, Chandratilleke MG, Picot J, Brinn MP, Esterman AJ, Smith BJ. Physical training for asthma. Cochrane Database Syst Rev 2014; 9: CD001116.
Puhan MA, Gimeno-Santos E, Scharplatz M, Troosters T, Walters EH, Steurer J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2011; 10: CD005305.
American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 2003; 167: 211-77.
Porszasz J, Stringer W, Casaburi R. Equipment, measurements and quality control. In: Ward SA , Palange P (Eds). Clinical Exercise Testing: European Respiratory Monograph. European Respiratory Society Journals; 2007: 108-28.
Whipp BJ, Davis JA, Torres F, Wasserman K. A test to determine parameters of aerobic function during exercise. J Appl Physiol Respir Environ Exerc Physiol 1981; 50: 217-21.
Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000; 20: 251-8.
Sullivan CS, Casaburi R, Storer TW, Wasserman K. Non-invasive prediction of blood lactate response to constant power outputs from incremental exercise tests. Eur J Appl Physiol Occup Physiol 1995; 71: 349-54.
Beaver WL, Wasserman K, Whipp BJ. Improved detection of lactate threshold during exercise using a log-log transformation. J Appl Physiol (1985) 1985; 59: 1936-40.
Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol (1985) 1986; 60: 2020-7.
Wasserman K, Beaver WL, Whipp BJ. Gas exchange theory and the lactic acidosis (anaerobic) threshold. Circulation 1990; 81: II14-30.
Wasserman K. The anaerobic threshold: definition, physiological significance and identification. Adv Cardiol 1986; 35: 1-23.
Sue DY, Wasserman K, Moricca RB, Casaburi R. Metabolic acidosis during exercise in patients with chronic obstructive pulmonary disease. Use of the V-slope method for anaerobic threshold determination. Chest 1988; 94: 931-8.
Whipp BJ, Ward SA, Wasserman K. Respiratory markers of the anaerobic threshold. Adv Cardiol 1986; 35: 47-64.
Matsumura N, Nishijima H, Kojima S, Hashimoto F, Minami M, Yasuda H. Determination of anaerobic threshold for assessment of functional state in patients with chronic heart failure. Circulation 1983; 68: 360-7.
Simonton CA, Higginbotham MB, Cobb FR. The ventilatory threshold: quantitative analysis of reproducibility and relation to arterial lactate concentration in normal subjects and in patients with chronic congestive heart failure. Am J Cardiol 1988; 62: 100-7.
Dickstein K, Barvik S, Aarsland T, Snapinn S, Karlsson J. A comparison of methodologies in detection of the anaerobic threshold. Circulation 1990; 81: II38-46.
Patessio A, Casaburi R, Carone M, Appendini L, Donner C, Wasserman K. Comparison of gas exchange, lactate, and lactic acidosis thresholds in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis 1993; 148: 622-6.
Older P, Smith R, Courtney P, Hone R. Preoperative evaluation of cardiac failure and ischemia in elderly patients by cardiopulmonary exercise testing. Chest 1993; 104: 701-4.
Smith TB, Stonell C, Purkayastha S, Paraskevas P. Cardiopulmonary exercise testing as a risk assessment method in non cardio-pulmonary surgery: a systematic review. Anaesthesia 2009; 64: 883-93.
West M, Jack S, Grocott MP. Perioperative cardiopulmonary exercise testing in the elderly. Best Pract Res Clin Anaesthesiol 2011; 25: 427-37.
Grocott MP, Pearse RM. Prognostic studies of perioperative risk: robust methodology is needed. Br J Anaesth 2010; 105: 243-5.
Belardinelli R, Lacalaprice F, Carle F, et al. Exercise-induced myocardial ischaemia detected by cardiopulmonary exercise testing. Eur Heart J 2003; 24: 1304-13.
Glaser S, Obst A, Koch B, et al. Pulmonary hypertension in patients with idiopathic pulmonary fibrosis – the predictive value of exercise capacity and gas exchange efficiency. PLoS One 2013; 8: e65643.
Guazzi M, Cahalin LP, Arena R. Cardiopulmonary exercise testing as a diagnostic tool for the detection of left-sided pulmonary hypertension in heart failure. J Card Fail 2013; 19: 461-7.
McCabe C, Deboeck G, Harvey I, et al. Inefficient exercise gas exchange identifies pulmonary hypertension in chronic thromboembolic obstruction following pulmonary embolism. Thromb Res 2013; 132: 659-65.
Simpson JC, Sutton H, Grocott MP. Cardiopulmonary exercise testing – a survey of current use in England. JICS 2009; 10: 275-8.
Huddart S, Young EL, Smith RL, Holt PJ, Prabhu PK. Preoperative cardiopulmonary exercise testing in England – a national survey. Periop Med (Lond) 2013; 2: 4.
Colson M, Baglin J, Bolsin S, Grocott MP. Cardiopulmonary exercise testing predicts 5 yr survival after major surgery. Br J Anaesth 2012; 109: 735-41.
Carlisle J, Swart M. Mid-term survival after abdominal aortic aneurysm surgery predicted by cardiopulmonary exercise testing. Br J Surg 2007; 94: 966-9.
James S, Jhanji S, Smith A, O’Brien G, Fitzgibbon M, Pearse RM. Comparison of the prognostic accuracy of scoring systems, cardiopulmonary exercise testing, and plasma biomarkers: a single-centre observational pilot study. Br J Anaesth 2014; 112: 491-7.
US National Institutes of Health. Cardiopulmonary Exercise Testing and Preoperative Risk Stratification. ClinicalTrials.Gov Identifier: NCT00737828. Available from URL: https://clinicaltrials.gov/ct2/show/NCT00737828?term=grocott&rank=3 (accessed September 2014).
Ronellenfitsch U, Schwarzbach M, Hofheinz R, et al. Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: systematic review with meta-analysis combining individual patient and aggregate data. Eur J Cancer 2013; 49: 3149-58.
Bosset JF, Collette L, Calais G, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med 2006; 355: 1114-23.
Petrelli F, Barni S. Response to neoadjuvant chemotherapy in ductal compared to lobular carcinoma of the breast: a meta-analysis of published trials including 1,764 lobular breast cancer. Breast Cancer Res Treat 2013; 142: 227-35.
Leow JJ, Martin-Doyle W, Fay AP, Choueiri TK, Chang SL, Bellmunt J. A systematic review and meta-analysis of adjuvant and neoadjuvant chemotherapy for upper tract urothelial carcinoma. Eur Urol 2014; DOI:10.1016/j.eururo.2014.03.003.
Horita N, Miyazawa N, Morita S, et al. Preoperative chemotherapy is effective for stage III resectable non-small-cell lung cancer: metaanalysis of 16 trials. Clin Lung Cancer 2013; 14: 488-94.
Jack S, West MA, Raw D, et al. The effect of neoadjuvant chemotherapy on physical fitness and survival in patients undergoing oesophagogastric cancer surgery. Eur J Surg Oncol 2014; 40: 1313-20.
West MA, Loughney L, Barben CP, et al. The effects of neoadjuvant chemoradiotherapy on physical fitness and morbidity in rectal cancer surgery patients. Eur J Surg Oncol 2014; DOI:10.1016/j.ejso.2014.03.021.
Davar D, Tarhini AA, Kirkwood JM. Adjuvant immunotherapy of melanoma and development of new approaches using the neoadjuvant approach. Clin Dermatol 2013; 31: 237-50.
Ditmyer MM, Topp R, Pifer M. Prehabilitation in preparation for orthopaedic surgery. Orthop Nurs 2002; 21: 43-51.
Topp R, Ditmyer M, King K, Doherty K, Hornyak J 3rd. The effect of bed rest and potential of prehabilitation on patients in the intensive care unit. AACN Clin Issues 2002; 13: 263-76.
Heran BS, Chen JM, Ebrahim S, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2011; 7: CD001800.
Oldridge N. Exercise-based cardiac rehabilitation in patients with coronary heart disease: meta-analysis outcomes revisited. Future Cardiol 2012; 8: 729-51.
Kothmann E, Batterham AM, Owen SJ, et al. Effect of short-term exercise training on aerobic fitness in patients with abdominal aortic aneurysms: a pilot study. Br J Anaesth 2009; 103: 505-10.
Arthur HM, Daniels C, McKelvie R, Hirsh J, Rush B. Effect of a preoperative intervention on preoperative and postoperative outcomes in low-risk patients awaiting elective coronary artery bypass graft surgery. A randomized, controlled trial. Ann Intern Med 2000; 133: 253-62.
US National Institutes of Health. The Effect of Chemotherapy and Surgery for Cancer on Exercise Capacity. ClinicalTrials.Gov. Identifier: NCT01325883. Available from URL: https://clinicaltrials.gov/ct2/show/NCT01325883?term=grocott&rank=5 (accessed September 2014).
US National Institutes of Health. Clinical Trials Registry. Available from URL: https://clinicaltrials.gov/ct2/home (accessed September 2014).
Grocott MP, Browne JP, Van der Meulen J, et al. The postoperative morbidity survey was validated and used to describe morbidity after major surgery. J Clin Epidemiol 2007; 60: 919-28.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240: 205-13.
Statement of competing interests (relating to this article)
Dr. Denny Z. H. Levett is course director for the UK Perioperative Cardiopulmonary Exercise Course and is an executive board member of the Xtreme-Everest Oxygen Research Consortium, who have received unrestricted research grant funding from (amongst others) BOC Medical (Linde Group) and Smiths Medical. Professor Michael P. W. Grocott is a co-chair of the annual UK National Perioperative Cardiopulmonary Exercise Testing Meeting and a board member of CPX International. He has received honoraria for speaking for and/or travel expenses from BOC Medical (Linde Group) and Cortex GmBH. He leads the Fit-4-Surgery research collaboration and also leads the Xtreme-Everest Oxygen Research Consortium. Professor Michael P. W. Grocott is also funded in part from the British Oxygen Company Chair of the Royal College of Anaesthetists awarded by the National Institute of Academic Anaesthesia. Some of this work was undertaken at University Southampton NHS Foundation Trust – University of Southampton NIHR Respiratory Biomedical Research Unit, which received a portion of funding from the UK Department of Health Research Biomedical Research Units funding scheme. All funding was unrestricted. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Levett, D.Z.H., Grocott, M.P.W. Cardiopulmonary exercise testing, prehabilitation, and Enhanced Recovery After Surgery (ERAS). Can J Anesth/J Can Anesth 62, 131–142 (2015). https://doi.org/10.1007/s12630-014-0307-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-014-0307-6