
Abstract
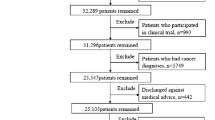
Due to high costs, resources and managemant associated with readmission into Intensive Care Units (ICU), it has been a center of clinical research. Previous research successfully identified several common risk factors and proposed a variety of frameworks to predict ICU readmissions, whereas, some studies reported that many risk factors were too specific and/or had limited focus. This study aims to investigate and analyze if the relevance of ICU readmission risk factors may have changed overtime. We used MIMIC-III database with 42,307 ICU stays of 31,749 patients from a US hospital, related to medical services provided from 2001 to 2012. The dataset was initially split into two chronological subsets (2001–2008 and 2008–2012), and then split again into train (70%) and test (30%) datasets. The training datasets were rebalanced through undersampling technique. To identify if the most relevant risk factors changes over time, 13 variables (12 features and one class) were selected and a three-step machine learning approach was executed: (i) Numerical Analysis, to identify overall quantitative changes; (ii) Feature Correlation Value Analysis, to rank the most important risk factors in each subset and compare them to identify any significant changes; and (iii) Classifier Performance Analysis, to identify changes in the risk factors prediction capability, based on the three machine learning algorithms - Multilayer Perceptron, Random Forest and Support Vector Machine. When considering readmission rates, some changes were observed for patients using private insurance (variability of +3.0%) and first admitted in ICU through Medical Intensive Care Unit (−3.1%). Regarding the feature analysis, the two most relevant variables were the same in both datasets, having similar correlation value. When applying the machine learning algorithms in test datasets, the model presented similar results for both periods, achieving the best accuracy of 86.4%, and Area Under ROC Curve (AUC) of 0.642. The difference in AUC values between the first and the second periods varied up to 0.05 (better in the first dataset) and in accuracy up to 4% (better in the second period). Overall results indicate that the most relevant risk factors were stable over the years, with some minor changes. Further research is required to incorporate other readmission risk factors, such as social determinants and mental health and well-being.


Similar content being viewed by others

Notes
LACE is the acronym for Length of Stay (L), Acute Admission (A), Comorbidity (C) and Visits to Emergency (E)
HOSPITAL is the acronym for Hemoglobin at discharge (H), discharge from an oncology service (O), sodium level at discharge (S), procedure during the index admission (P), index type of admission (IT), number of admissions during the last 12 months (A), and length of stay (L)
PARR-30 is the acronym for “Patients at Risk of Re-admission within 30 days” 10. Billings, J., et al., Development of a predictive model to identify inpatients at risk of re-admission within 30 days of discharge (PARR-30). BMJ open, 2012. 2(4): p. e001667.
PREADM is the acronym for “Preadmission Readmission Detection Model”
LOS, Number of Services, service MED and service SURG
References
Bosco JA, et al. Cost burden of 30-day readmissions following Medicare total hip and knee arthroplasty. J Arthroplast. 2014;29(5):903–5.
Paratz J, Thomas P, Adsett J. Re-admission to intensive care: identification of risk factors. Physiother Res Int. 2005;10(3):154–63.
Braet A, et al. Risk factors for unplanned hospital re-admissions: a secondary data analysis of hospital discharge summaries. J Eval Clin Pract. 2015;21(4):560–6.
Elliott M, Worrall-Carter L, Page K. Intensive care readmission: a contemporary review of the literature. Intensive and Critical Care Nursing. 2014;30(3):121–37.
Jiang S, et al. An integrated machine learning framework for hospital readmission prediction. Knowl-Based Syst. 2018;146:73–90.
Wong EG, et al. Association of severity of illness and intensive care unit readmission: A systematic review. Heart & Lung: The Journal of Acute and Critical Care. 2016;45(1):3–9 e2.
van Walraven C, et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. Can Med Assoc J. 2010;182(6):551–7.
Donzé J, et al. Potentially avoidable 30-day hospital readmissions in medical patients: derivation and validation of a prediction model. JAMA Intern Med. 2013;173(8):632–8.
Lee EW. Selecting the best prediction model for readmission. J Prev Med Public Health. 2012;45(4):259.
Billings J, et al. Development of a predictive model to identify inpatients at risk of re-admission within 30 days of discharge (PARR-30). BMJ Open. 2012;2(4):e001667.
Timmers T, et al. Patients’ characteristics associated with readmission to a surgical intensive care unit. Am J Crit Care. 2012;21(6):e120–8.
Charlson ME, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
van Walraven C, Wong J, Forster AJ. LACE+ index: extension of a validated index to predict early death or urgent readmission after hospital discharge using administrative data. Open Medicine. 2012;6(3):e80.
Shadmi E, et al. Predicting 30-day readmissions with preadmission electronic health record data. Med Care. 2015;53(3):283–9.
Rothman MJ, Rothman SI, Beals J IV. Development and validation of a continuous measure of patient condition using the electronic medical record. J Biomed Inform. 2013;46(5):837–48.
Robinson R, Hudali T. The HOSPITAL score and LACE index as predictors of 30 day readmission in a retrospective study at a university-affiliated community hospital. Peer J. 2017;5:e3137.
Maali Y, et al. Predicting 7-day, 30-day and 60-day all-cause unplanned readmission: a case study of a Sydney hospital. BMC Medical Informatics and Decision Making. 2018;18(1):1.
Johnson AE, et al. MIMIC-III, a freely accessible critical care database. Scientific Data. 2016;3:160035.
Fialho AS, et al. Data mining using clinical physiology at discharge to predict ICU readmissions. Expert Syst Appl. 2012;39(18):13158–65.
Hall M, et al. The WEKA data mining software: an update. ACM SIGKDD Explorations Newsletter. 2009;11(1):10–8.
Van Hulse J, Khoshgoftaar TM, Napolitano A. Experimental perspectives on learning from imbalanced data. In: Proceedings of the 24th international conference on Machine learning. ACM; 2007.
Al-Shahib A, Breitling R, Gilbert D. Feature selection and the class imbalance problem in predicting protein function from sequence. Appl Bioinforma. 2005;4(3):195–203.
Chawla NV, et al. SMOTE: Synthetic minority over-sampling technique. J Artif Intell Res. 2002;16:321–57.
Goswami S, Chakrabarti A. Feature selection: A practitioner view. International Journal of Information Technology and Computer Science (IJITCS). 2014;6(11):66.
Singh B, Kushwaha N, Vyas OP. A feature subset selection technique for high dimensional data using symmetric uncertainty. Journal of Data Analysis and Information Processing. 2014;2(04):95.
Yu L, Liu H. Feature selection for high-dimensional data: A fast correlation-based filter solution. In: Proceedings of the 20th international conference on machine learning (ICML-03). 2003.
Saito T, Rehmsmeier M. The precision-recall plot is more informative than the ROC plot when evaluating binary classifiers on imbalanced datasets. PLoS One. 2015;10(3):e0118432.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no conflict of interest.
Ethical approval
The ethical approval was obtained from the appropriate committees prior to conducting the research study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Junqueira, A.R.B., Mirza, F. & Baig, M.M. A machine learning model for predicting ICU readmissions and key risk factors: analysis from a longitudinal health records. Health Technol. 9, 297–309 (2019). https://doi.org/10.1007/s12553-019-00329-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12553-019-00329-0