
Abstract
Background
Exercise testing should be symptom-limited. Nevertheless, 40% of clinical laboratories applying for ICANL accreditation use 85% of maximal age-predicted heart rate (MPHR) as the primary exercise endpoint. We hypothesized that this approach importantly may underestimate exercise capacity and inducible ischemia.
Methods
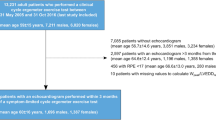
Two patient cohorts were studied. 1. A prospective registry of patients referred for exercise testing. 2. A retrospective cohort of patients with positive exercise ECG.
Results
Of 306 registry patients, 211 (69%) continued exercising after reaching 85% MPHR to maximal HR of 101% ± 7% of MPHR. Forty-two patients (14%) stopped <1 minute after achieving 85% MPHR; 53 (17%) did not achieve 85% MPHR. More women (75%) than men (64%) achieved >85% MPHR (P = .02). Of 300 patients with positive ECG, 232 patients (77%) exercised to >85% MPHR. At 85% MPHR 144 patients (62%) had positive ECG (1.2 ± .7 mm ST depression) compared to 232 patients (100%) at peak exercise (2.3 ± .9 mm ST depression, P < .001). Mean workload at 85% MPHR was 7.3 ± 2.4 METs compared to 10.6 ± 2.8 METs at peak exercise (P < .001).
Conclusion
Achievement of 85% MPHR is not a valid diagnostic or functional exercise endpoint because it significantly underestimates exercise capacity and inducible ischemia.


Similar content being viewed by others


References
Mark DB, Shaw L, Harrell FE, Hlatky MA, Lee KL, Bengtson JR, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med 1991;325:849-53.
Tanaka H, Monahan KD, Seals DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol 2001;37:153-6.
Holly TA, Abbott BG, Al-Mallah M, Calnon DA, Cohen MC, DiFilippo FP, et al. ASNC imaging guidelines for nuclear cardiology procedures. Single photon-emission computed tomography. 2010. http://www.asnc.org/section_73.cfm (Accessed September, 2011).
Froelicher VF, Lehman KG, Thomas R, Goldman S, Morrison D, Edson R, et al. The electrocardiographic exercise test in a population with reduced workup bias: Diagnostic performance, computerized interpretation, and multivariable prediction. Ann Int Med 1998;128:965-74.
Morris CK, Ueshima K, Kawaguchi T, Hideg A, Froelicher VF. Prognostic value of exercise capacity: A review of the literature. Am Heart J 1991;122:1423-31.
Bruce RA, Blackmon JR, Jones JW, Strait G. Exercise testing in adult normal subjects and cardiac patients. Pediatrics 1963;32:742-56.
Iskandrian AS, Heo J, Kong B, Lyons E. Effect of exercise level on the ability of Thallium-201 tomographic imaging in detecting coronary artery disease: Analysis of 461 patients. J Am Coll Cardiol 1989;14:1477-86.
Garber CE, Carlton RA, Camaione DN, Heller GV. The threshold for myocardial ischemia varies in patients with coronary artery disease depending on the exercise protocol. J Am Coll Cardiol 1991;17:1256-62.
Heller GV, Ahmed I, Tilkemeier PL, Barbour MM, Garber CE. Comparison of chest pain, electrocardiographic changes and thallium-201 scintigraphy during varying exercise intensities in men with stable angina pectoris. Am J Cardiol 1991;68:569-74.
Heller GV, Ahmed I, Tilkemeier PL, Barbour MM, Garber CE. Influence of exercise intensity on the presence, distribution, and size of thallium-201 defects. Am Heart J 1992;123:908-16.
Lauer MS, Francis GS, Okin PM, Pashkow FJ, Snader CE, Marwick TH. Impaired chronotropic response to exercise stress testing as a predictor of mortality. JAMA 1999;281:524-9.
Gibbons RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, Froelicher VF, et al. ACC/AHA 2002 guideline update for exercise testing: Summary article: A report of the ACC/AHA Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). J Am Coll Cardiol 2002;40:1531-40.
Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2010;56:e50-103.
Azarbal B, Hayes SW, Lewin HC, Hachamovitch R, Cohen I, Berman DS. The incremental prognostic value of percentage of heart rate reserve achieved over myocardial perfusion single-photon emission computed tomography in the prediction of cardiac death and all cause mortality. Superiority over 85% of maximal age-predicted heart rate. J Am Coll Cardiol 2004;44:423-30.
Navare SM, Thompson PD. Acute cardiovascular response to exercise and its implications for exercise testing. J Nucl Cardiol 2003;10:521-8.
Henzlova MJ, Cerqueira MD, Hansen CL, Taillefer R, Yao S. ASNC Imaging guidelines for nuclear cardiology procedures. Stress Protocols and tracers. 2009. http://www.asnc.org/section_73.cfm (Accessed June, 2011).
Fox SM, Naughton JP, Haskell WL. Physical activity and the prevention of coronary artery disease. Ann Clin Res 1971;3:404-32.
Pinkstaff S, Peberdy MA, Kontos MC, Finucane S, Arena R. Quantifying exertion level during exercise stress testing using percentage of age-predicted maximal heart rate, rate pressure product, and perceived exertion. Mayo Clin Proc 2010;85:1095-100.
Bourque JM, Charlton GT, Holland BH, Belyea CM, Watson DD, Beller GA. Prognosis in patients achieving ≥10 METs on exercise stress testing: Was SPECT imaging useful? J Nucl Cardiol 2011;18:230-7.
Myers J, Manish P, Froelicher V, Partington S, Atwood E. Exercise capacity and mortality among men referred for exercise testing. New Eng J Med 2002;346:793-801.
Gulati M, Pandey DK, Arnsdorf MF, Lauderdale DS, Thisted RA, Wicklund RH, Al-Hani AJ, Black HR. Exercise capacity and the risk of death in women: The St James Women Take Heart Project. Circulation 2003;108:1554-9.
Mora S, Redberg RF, Cui Y, Whiteman MK, Flaws JA, Sharrett AR, Blumenthal RS. Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women. JAMA 2003;290:1600-7.
Acknowledgments
We would like to thank Mary Beth Farrell, MS, CNMT of the Intersocietal Commission for Accreditation of Nuclear Laboratories (www.icanl.org), Ellicott City, MD for performing a survey of the exercise protocols at our request. We greatly appreciate the constructive comments by Drs Barry L. Zaret and Raymond Russell.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jain, M., Nkonde, C., Lin, B.A. et al. 85% of maximal age-predicted heart rate is not a valid endpoint for exercise treadmill testing. J. Nucl. Cardiol. 18, 1026–1035 (2011). https://doi.org/10.1007/s12350-011-9454-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-011-9454-0