
Abstract
Catheter ablation (CA) of atrial fibrillation (AF) is currently one of the most commonly performed electrophysiology procedures. Ablation of paroxysmal AF is based on the elimination of triggers by pulmonary vein isolation (PVI), while different strategies for additional AF substrate modification on top of PVI have been proposed for ablation of persistent AF. Nowadays, various technologies for AF ablation are available. The radiofrequency point-by-point ablation navigated by electro-anatomical mapping system and cryo-balloon technology are comparable in terms of the efficacy and safety of the PVI procedure. Long-term success of AF ablation including multiple procedures varies from 50 to 80%. Arrhythmia recurrences commonly occur, mostly due to PV reconnection. The recurrences are particularly common in patients with non-paroxysmal AF, dilated left atrium and the "early recurrence" of AF within the first 2–3 post-procedural months. In addition, this complex procedure can be accompanied by serious complications, such as cardiac tamponade, stroke, atrio-esophageal fistula and PV stenosis. Therefore, CA represents a second-line treatment option after a trial of antiarrhythmic drug(s). Good candidates for the procedure are relatively younger patients with symptomatic and frequent episodes of AF, with no significant structural heart disease and no significant left atrial enlargement. Randomized trials demonstrated the superiority of ablation compared to antiarrhythmic drugs in terms of improving the quality of life and symptoms in AF patients. However, nonrandomized studies reported additional clinical benefits from ablation over drug therapy in selected AF patients, such as the reduction of the mortality and stroke rates and the recovery of tachyarrhythmia-induced cardiomyopathy. Future research should enable the creation of more durable ablative lesions and the selection of the optimal lesion set in each patient according to the degree of atrial remodeling. This could provide better long-term CA success and expand indications for the procedure, especially among the patients with non-paroxysmal AF.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The incidence and prevalence of atrial fibrillation (AF) are progressively increasing because of aging of the population, the higher prevalence of known AF risk factors in older people and better strategies for arrhythmia detection [1]. The presence of AF is associated with a 1.5–2-fold increase in death and heart failure (HF) and 5-fold increase in the rates of stroke and systemic thromboembolism [2, 3]. In addition, AF can significantly reduce quality of life (QoL) and exercise tolerance because of limiting symptoms [1,2,3]. Catheter ablation (CA) is superior to antiarrhythmic drug (AAD) therapy in patients with paroxysmal (PAF) and persistent AF (PeAF) [4]. The number of AF ablation procedures in the last decade grew exponentially, and indications for the procedure are increasingly expanding; hence, AF-CA has become the most commonly performed ablation procedure [5].
However, the success of AF ablation is limited and depends largely on the patient’s clinical characteristics [2, 3, 6]. Optimal selection of patients for AF-CA is important to avoid exposing the patients with low chances for long-term sinus rhythm maintenance to an invasive procedure and to refer those who would benefit from AF ablation for AF-CA [1,2,3, 6]. In this article, we present an overview of the basic technical aspects of the AF-CA procedure and long-term results of the procedure and discuss the optimal selection of AF patients for CA as well as an adequate follow-up strategy and drug therapy after this complex procedure.
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Catheter Ablation Procedure
Set of Ablation Lesions
The initiation and maintenance of an AF episode are caused by a complex interaction of the arrhythmia triggers, atrial substrate and the autonomic nervous system activity [2, 3]. The triggers are primarily responsible for the PAF, but with progression from paroxysmal to persistent arrhythmia, an atrial substrate assumes a dominant role in sustaining AF [2, 3, 7].
Although the optimal set of ablation lesions has not been identified yet, it depends primarily on the clinical type of AF [2, 3]. In patients with PAF, the procedure is directed toward the elimination (isolation) of AF triggers, while in non-PAF patients many operators proceed with a supplementary modification of the AF substrate, on top of trigger elimination, to improve the procedure outcome [3, 8,9,10,11,12,13]. For patients with long-standing PeAF, the success of multiple ablation procedures based solely on the pulmonary vein isolation (PVI) strategy was less than 50% during a 5-year follow-up [14]. However, the STAR AF II study recently failed to demonstrate superiority of adjuvant ablation strategies compared to PVI alone in patients with PeAF [15]. This multicenter study randomized patients to three ablation strategies: PVI alone, PVI + complex fractionated atrial electrogram ablation (CFAE) and PVI + left atrial (LA) lines, and after 18 months of follow-up, the rate of freedom from AF (with or without AADs) was 59, 49 and 46%, respectively, and after redo ablation in patients with clinical recurrence there was still no significant difference in final arrhythmia outcome [15]. Obviously, using any set of lesions as a routine ablation strategy will lead to over- or under-treatment in a significant proportion of AF patients. Therefore, the optimal ablation strategy should be individually adjusted in each AF patient and determined by the degree of structural and electrical changes in the atrial myocardium and not only by the AF clinical type [16,17,18].
Targeting the AF Triggers
The arrhythmia triggers originate within the PVs in majority (80–94%) of AF patients [19, 20]. Compared to LA myocytes, cardiomyocytes in the PVs have a shorter refractoriness and increased triggered activity, and myocardial strands at the LA-PV junction form an anisotropic mesh with a propensity for micro-reentry [21]. Figure 1a illustrates a typical electrocardiographic (ECG) presentation of a highly active PV trigger with repetitive short bursts of atrial ectopic beats in the patient with PAF.

a–c Electrocardiograms of a patient with paroxysmal AF. a Repetitive short-lasting runs of atrial tachycardias, i.e., salvos of atrial ectopic beats, commonly originating from the pulmonary veins. These runs of atrial arrhythmia are a trigger for paroxysmal AF (b). After introduction of a class I antiarrhythmic drug (propafenone), an AF episode organized to typical atrial flutter (c), implying the presence of a complex atrial arrhythmia substrate. AF atrial fibrillation
Electrical isolation of the PVs is a cornerstone of AF ablation [2,3,4,5,6, 8,9,10,11,12,13,14,15,16,17]. During the evolution of the procedure, the ablation level was displaced from the PV ostia to the LA antra to increase the clinical success and reduce the risk of PV stenosis [22,23,24]. The ultimate endpoint of AF-CA is electrical isolation of all PVs [2,3,4,5,6, 22,23,24]. Evaluation of PV electrical activity and identification of residual gaps in the LA-PV conduction during and/or after ablation are performed by a circular multipolar catheter placed at the PV ostium, as presented in Fig. 2 [23, 24].

Intracardiac electrogram during a PVI procedure, paper speed 200 mm/s. A circular multipolar mapping catheter was positioned in the left superior PV. After completion of PVI, a spontaneous paroxysm of AF was recorded on the circular catheter (yellow) within the isolated PV, while stable sinus rhythm was maintained in the LA (see standard ECG leads, blue, as well as coronary sinus electrograms, green), confirming the exit PV-LA block after successful ablation. PVI pulmonary vein isolation, AF atrial fibrillation, LA left atrium, ECG electrocardiogram
Less commonly, identification and elimination of non-PV triggers are required for AF suppression [3, 20]. The majority of these non-PV triggers were found in the superior caval vein (especially in women and patients with chronic pulmonary disease or sleep apnea or those undergoing redo PAF ablation procedure), coronary sinus, and crista terminalis or at the posterior LA wall (in elderly and non-PAF patients), as well as in the left atrial appendage (LAA) (at redo ablation procedures for non-PAF) [25]. It was recently reported that non-PV triggers were identified in up to 44% of the patients with long-standing PeAF, and their presence was a strong predictor of AF recurrence after a CA procedure [26].
AF Substrate Modification
The process of LA remodeling is associated with chronic inflammation, fibrous degenerative changes and alteration in atrial electrophysiology (EP), leading to the development of the substrate for non-PAF maintenance [27, 28]. In patients with non-PAF and/or a long history of AF, magnetic resonance imaging (MRI) and intracardiac voltage maps reveal a widespread scarring most commonly in the thin posterior and anterior LA walls as well as in the LA septum [16,17,18, 27, 28]. Different adjuvant strategies for AF substrate modification on top of PVI have been proposed; however, data on their effectiveness are conflicting, and presently there is no consensus whether their application in the first-ever AF-CA procedure is justified [2].
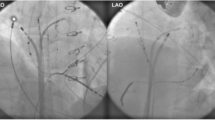
The linear LA ablation mimics the surgical mini-MAZE procedure and consists of two standard lines: the roof line connecting cranial aspects of upper PVs and the mitral isthmus line connecting the lateral mitral annulus and left inferior PV (Fig. 3a) [10, 11]. Clinical efficacy of this approach is based on LA compartmentalization and prevention of post-PVI macro-reentrant LA tachycardia [29]. The achievement of a complete and persistent conduction block across the lines is challenging but critical to eliminating arrhythmia [30, 31]. LA linear ablation significantly prolongs the procedure and fluoroscopy times and increases the risk of cardiac perforation [10, 15].

a Standard set of LA lesions commonly deployed in patients with non-paroxysmal AF, consisting of two circular ablation lines for isolation of ipsilateral PVs combined with two standard LA lines, i.e., the roof line connecting both upper PVs and mitral line connecting the lateral aspect of the mitral annulus with left PVs. b “Organization” of persistent AF into AT culminating in termination of the arrhythmia during the extensive ablation of complex fragmented atrial electrograms (CFAEs), i.e., LA defragmentation, due to considerable debulking of the LA substrate. LA left atrium, AF atrial fibrillation, PV pulmonary vein, AT atrial tachycardia
Defragmentation of the LA is based on the elimination of all multicomponent electrograms of short cycle length (i.e., CFAE), which possibly represent the dominant rotors of functional AF multiple-wavelet circuits [32]. Their ablation usually leads to prolongation of AF cycle length, culminating in conversion into atrial tachycardia (AT) or sinus rhythm (Fig. 3b) [11, 32]. However, the endpoints of such ablation are not clearly defined, resulting in low intra-procedural reproducibility of CFAE identification and elimination, a limited clinical success rate and frequent occurrence of iatrogenic ATs [15]. The presence of small rotor-like reentry with fibrillatory conduction in the rest of the atrium was identified by conventional mapping and signal analysis in 15% of patients with non-PAF, particularly in those with a shorter AF episode and less remodeled atrial substrate [33]. These rotors were responsible for maintenance of AF, and their ablation on top of PVI terminated AF in 75% of the cases [33]. Recent studies reported the FIRM (Focal Impulse and Rotor Modulation) ablation strategy, providing more specific identification of AF drivers amenable to ablation [7]. Using panoramic contact mapping with a basket multipolar catheter within the atria, stable electrical AF rotors and focal sources of AF were reproducibly identified [34]. Rotors and focal sources of AF perpetuated within atrial areas of ≈2 cm2 and their selective ablation led to the termination or organization of AF in 86% of patients with PeAF or PAF, offering a promising clinical outcome. However, the majority of CFAE sites were identified remote from AF sources and were not appropriate targets for ablation [34].
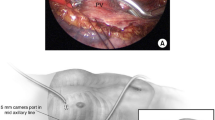
The concept of the LA denervation includes an intentional damage of the LA ganglionated plexi (GPs) to suppress their influence on the AF triggers and substrate [3]. Four GPs are located approximately 1–2 cm outside the PV ostia and can be identified by local endocardial high-frequency current stimulation or empirically ablated at specific anatomical areas, as illustrated in Fig. 4 [35]. However, the endpoint of “sufficient” denervation is not precisely defined, and sometimes it leads to post-procedural sinus tachycardia or postural hypotension [36]. Moreover, long-term consequences of parasympathetic denervation after AF ablation are not known. It is well recognized that cardiac denervation is a marker of higher cardiovascular death risk in patients with diabetes and heart failure and after myocardial infarction [37].

The GP ablation strategy for substrate modification (a). During left superior GP ablation a transitory slowing of the sinus rate was provoked. After several ablation attempts in this area, the vagally mediated response was blunted. b The pre-ablation voltage maps in two patients with paroxysmal AF were compared according to the voltage-color scale (red and violet represent low and high voltage, respectively). On the left part, a normal-to-high voltage map was obtained (violet color dominates), suggesting absence of significant LA fibrosis. In this particular patient the PVI procedure should be sufficient for AF suppression. However, on the right an example of a low voltage map is presented, suggesting the presence of profound LA fibrosis (red is dead) and the progression of the AF substrate, probably necessiting the adjuvant substrate modification on top of PVI. GP ganglionated plexi, AF atrial fibrillation, PVI pulmonary vein isolation
Approximately 20–25% of AF patients also have episodes of typical or atypical atrial flutter (AFL) due to the presence of a complex atrial substrate and/or a pro-arrhythmic effect of class IC or III AADs prescribed for the prevention of AF (Fig. 1) [38]. Commonly, the adjuvant ablation of these “organized” arrhythmias is a part of the substrate modification procedure to improve the outcome [3, 38]. Several studies have demonstrated no clinical benefit of additional ablation for typical or peri-mitral AFL beyond PVI in these patients, emphasizing the critical importance of the PV triggers for prevention of various atrial tachyarrhythmias [39, 40]. However, in patients with clinically documented or inducible typical AFL, cavotricuspid isthmus ablation during the same session is recommended [2].
Diseased atrial regions exhibiting low-voltage activity are responsible for slow conduction, contributing to the AF substrate [16]. Several reports confirmed the feasibility of a tailored atrial substrate modification based on low-voltage area ablation or the box isolation of “fibrotic” areas (BIFA) (Fig. 4b) [16, 41]. This individualized approach offers identification of patient-specific targets for ablation, irrespective of AF type [16]. The low-voltage areas were identified in 35% and 10% of patients with PeAF and PAF, respectively. The 1-year AF-free survival was significantly better among patients with low-voltage areas who underwent further substrate modification than in those who received only PVI (70% vs. 27%) [16]. In another study, ablation of these areas (in conjunction with PVI) led to termination of PeAF in 73% of patients and significantly improved the rate of 1-year single-procedure arrhythmia freedom compared to controls who underwent PVI alone [42].
A randomized study reported that empirical addition of LAA isolation on top of “standard” AF ablation significantly increases the rate of freedom from atrial arrhythmias during the 2-year follow-up [43]. Routine LAA isolation in this study was reported to be safe with no cases of stroke or embolism after the procedure, although an impaired contractile function of the LAA was identified post procedure in more than 50% of these patients using transesophageal echocardiography (TEE) [43]. However, the results of other investigators have recently aroused concerns regarding LAA thrombogenicity after its inadvertent isolation during a complex ablation of LA substrate for the treatment of AF [44]. During the 6-month follow-up after the procedure, stroke or transitory ischemic attack occurred in 6% of the patients with isolated LAA, and LAA thrombus was found in 21% of the remaining patients despite oral anticoagulation (OAC) therapy [44].
Ablation Technologies
The PVI can be performed by radiofrequency (RF) current or cryoenergy and by successive application of point-by-point necrotic lesions or a single shot of energy in a circular fashion at the level of the LA-PV junction [2, 3]. At present, the choice of technology is a matter of operator preference [2, 3].
Point-by-point PVI is performed using RF energy and a 3.5–4 mm irrigated-tip ablation catheter [22,23,24,25]. An electro-anatomical system is commonly used, providing a fluoroscopy reduction, better catheter navigation and additional information throughout the procedure such as the LA activation and voltage maps [12,13,14,15,16, 22,23,24,25, 41, 42]. This technology requires extensive training of the operator, but enables him/her to continue with ablation of the substrate, non-PV triggers or AFL once the PVI has been completed [9, 10, 12,13,14,15,16, 29,30,31,32, 35, 38,39,40,41,42,43,44]. Recent development of the catheters with contact-force sensing enabled a more efficient tissue heating and the formation of more a durable lesion with better clinical outcome [45, 46]. In addition, to date the RF energy source has been the most widely used technology for AF ablation; it was introduced early for the procedure, and this technology has the longest post-ablation follow-up data [2, 3, 6, 22].
A randomized study recently demonstrated non-inferiority of the cryo-balloon PVI procedure compared to standard RF point-by-point PVI with respect to clinical success and procedural safety during the mean follow-up of 1.5 years [47]. Although a cryo-balloon enables faster and easier PVI compared to RF technology, it was associated with significantly higher radiation doses because PV angiography to confirm complete PV occlusion by the balloon is necessary for optimal tissue freezing [47,48,49,50]. Cryo-balloon technology has a shorter learning curve and is less operator-dependent than RF ablation, ensuring a better reproducibility of the procedural endpoint especially among less experienced electrophysiologists [47,48,49,50]. Therefore, it could be an attractive option for low-to-medium volume centers with limited previous experience in AF ablation. The presence of unfavorable PV anatomy (i.e., a common trunk of ipsilateral PVs) limits the application of this technology and preoperative screening by computed tomography (CT) or MRI may help in appropriate patient selection [3, 45,46,47]. In addition, this technology is designed only for PVI procedures; if necessary, further ablation of targets other than PVs is not possible without exchanging the catheters and ablation set-up, increasing the cost of the procedure [47,48,49,50].
Visually guided laser balloon ablation requires a short learning curve for the operator and has several features that facilitate the PVI procedure [51]. Thus, by changing its diameter the balloon can accommodate various PV sizes and anatomies. In addition, a thin endoscope allows direct visualization of targeted atrial structures during ablation, and titration of energy provides creation of optimal lesions at different anatomical sites [51]. A multicenter randomized study reported comparable 12-month clinical success after visually guided laser-balloon ablation and standard irrigated RF ablation of AF (63.5% vs. 63.9%), similar procedural complication rates (11.8% vs. 14.5%) and similar rates of durable PVI lesions at redo procedures (52.7% vs. 46.4%) [51]. Balloon catheters that use RF energy for PVI have recently become available (hot balloon) or are on the way (multi-electrode RF balloon) [52].
Complications
Major complications occur in 4.5–6% of the AF ablation procedures, more commonly in older and female patients, patients with a very low or very high body mass index, those with structural heart disease and those undergoing a redo procedure, especially if the procedure is performed in a low-volume center [22, 53,54,55,56,57]. Peri-procedural mortality is 0.01% and most often is a related to cardiac tamponade, stroke or atrio-esophageal fistula [2, 22, 25]. The incidence of cardiac perforation and tamponade is between 0.5% and 3% and decreases with the learning curve of the operator [3, 53, 54, 57]. In the majority of these patients, emergency pericardiocentesis and reversal of anticoagulation are sufficient for complete recovery, but urgent surgical repair may be lifesaving in 15–20% of the cases, raising the question of the safety of the procedure performed without in-house surgical back-up [58]. Importantly, a delayed occurrence of tamponade, days to weeks after discharge, was reported because of a rupture of the thinned LA wall following ablation or inflammation in the setting of Dressler's syndrome [3, 25, 58]. The reported stroke rate ranges between 0.5% and 2% and is the highest during the procedure and in the first 7–30 post-procedural days [3, 22, 25, 53,54,55,56,57]. A strategy of uninterrupted OAC throughout the ablation procedure significantly reduced the intra-procedural stroke rate compared to "bridging" with low-molecular-weight heparin [2]. However, approximately 40% of low- or medium-volume centers have not implemented this strategy yet because it differs from local surgical practice in the case of a hemorrhagic procedural complication [59]. Systemic thromboembolism due to AF ablation should be treated by emergency percutaneous intervention or by thrombolytic therapy [3, 25]. Atrio-esophageal fistula is a rare complication (0.05%) associated with high mortality (75%) [2, 3, 25, 53,54,55,56,57]. Several strategies have been proposed for protecting the esophagus during an AF-CA procedure, such as pre-procedural or intra-procedural visualization of the esophagus (by barium swallow, 3D mapping system, CT or MRI), active displacement of the esophagus before RF delivery at the LA posterior wall (by TEE probe or intra-pericardial balloon insertion), monitoring of esophageal temperature during ablation, limiting the energy output or duration of RF application in the projection of the esophagus and esophageal cooling during the CA procedure (by irrigation of esophagus with cool water) [60]. The triad of symptoms such as sepsis, stroke and dysphagia appearing 7–30 days after the AF ablation procedure is suspicious for this complication [24, 61]. The diagnosis is confirmed by CT, while gastroscopy can be fatal because of insufflation of air into the esophagus and LA with massive cerebral embolism, and the treatment relies mainly on immediate surgery [3, 61]. Evolution of the PVI procedure with more proximal ablation outside the PV ostia led to considerable reduction of the PV stenosis rate to less than 1% [21,22,23,24, 53,54,55,56,57]. It should however be kept in mind that PV stenosis develops gradually and insidiously [3, 25]. The occurrence of pneumonia, hemoptysis, dyspnea and effort intolerance several months after the ablation procedure indicate secondary pulmonary hypertension due to PV stenosis [25]. Diagnosis is made by CT or MRI. Percutaneous angioplasty with stenting showed unsatisfactory long-term results with a high restenosis rate of up to 50% [62].
Success of AF Ablation
Long-term success of percutaneous AF-CA varies considerably from 50 to 80% [3, 6]. Estimation of the real AF ablation success is difficult because of inconsistency in the definitions of procedural success and post-procedural recurrences, the difference in the intensity of post-procedural rhythm monitoring as well as the analysis of outcomes after single or multiple CA procedures [2, 3]. The academic community has defined AF recurrence as the occurrence of any symptomatic or asymptomatic atrial tachyarrhythmia after the procedure lasting more than 30 s [2, 3]. It is obvious that this definition is arbitrary, and although it allows precise scientific communication, it should be understood in the broader clinical context. For example, if uncontrolled PeAF in a patient with tachycardiomyopathy and congestive HF symptoms transformed into oligosymptomatic, sporadic attacks of PAF accompanied with complete recovery of left ventricular (LV) function after AF ablation, we must underline the considerable clinical benefit of the procedure although formally it failed since the arrhythmia recurrence was clearly documented.
Therefore, the clinical success of AF ablation should be considered in relation to different outcomes, such as (1) the rhythm outcome after a single CA and after multiple ablation procedures, (2) the rhythm outcome without AADs and with AADs following ablation, (3) the rhythm outcome with respect to the intensity of rhythm monitoring (intermittent vs. continuous) and post-procedural follow-up strategy and (4) the outcome in terms of significant clinical issues other than rhythm control, such as improvement of LV function and/or QoL, AF-related symptom relief, reduction of mortality, etc.
Outcome After Single and Multiple Procedures
Long-term AF ablation success was significantly improved after repeated procedures in comparison to single AF ablation [6, 13, 63]. In a meta-analysis that included 19 studies and 6167 AF patients with mean age ranging from 51 to 65 years who were followed between 28 and 71 months after multiple AF ablation procedures, the AF-freedom rate after a single CA procedure was 65% at 1 year, 56% at 3 years and 51% at 5 years. However, after multiple ablation procedures AF was successfully suppressed in 86% of patients at 12 months, 79% of patients at 3 years and 78% at 5 years [6].
The rate of freedom from AF after a single CA procedure was significantly higher in patients with PAF than in those with PeAF [2, 3, 6, 13, 63]. The single-procedure annual success rate was 67% for PAF and 52% for PeAF [6]. At the end of long-term follow-up of between 3 and 5 years, only 54% of patients with PAF and 42% with PeAF were arrhythmia free. However, after multiple procedures long-term success was similar in patients with PAF or PeAF (79% and 78%, respectively), while the number of procedures per patient was significantly higher in patients with persistent compared to those with paroxysmal arrhythmia (1.7 vs. 1.4) [6].
AAD Therapy After Ablation
Even after repeated AF-CA procedures, one-third to one half of patients are still taking AADs [64]. In patients with recurrent arrhythmias after ablation, a decision on a re-do procedure is commonly postponed after an AAD trial, although an aggressive approach with early invasive re-intervention may be justified [65]. In addition, in patients with low expected procedural success (i.e., older patients with very dilated LA and non-PAF) and a history of a technically challenging previous procedure (e.g., difficult vascular or transseptal access or unusual PV anatomy), the clinician may indefinitely continue AAD therapy following the ablation regardless of outcome, hoping to prevent arrhythmia recurrence and avoid the re-do procedure [2, 3, 25, 63, 64].
Effectiveness of AADs seems to be increased after CA because of significant damage of the arrhythmogenic tissue responsible for the initiation and maintenance of AF as well as changes in the autonomic nervous tone after (un)intentional ablation of parasympathetic GPs [35, 66,67,68]. Therefore, the selection of AAD that was ineffective before the procedure could have a theoretical justification [67]. Data from a repeated invasive EP study showed that 3 months after failed ablation, the LA-PV conduction delay was significantly more pronounced in patients who maintained sinus rhythm on AADs than in “AAD non-responders” after the procedure [67]. It has been suggested that AADs after AF ablation promote further LA-PV conduction slowing until a block through the damaged tissue and occurrence of a more organized recurrent atrial arrhythmia with slower ventricular rate compared to pre-ablation AF [66, 68].
Reintroduction of AADs for AF recurrence after ablation resulted in successful 5-year arrhythmia suppression in up to 70% of 125 patients with multiple CA procedure failure [69]. During the follow-up of 161 PAF patients for almost 5 years after multiple CAs, 68% were free of AF without AADs, increasing to 80% after the re-introduction of AADs in those with recurrent AF [63]. In another study 100 patients with PAF were followed for more than 3 years after multiple ablation procedures [64]. The success rate was 57% off-AADs and 82% after re-introduction of AADs [64].
However, another study on 107 patients with PAF and PeAF who were randomly assigned to ablation alone or ablation combined with AADs (preferably amiodarone) showed different results from the previous reports [66, 70]. During a 12-month follow-up, the continuation of AAD therapy in patients undergoing AF ablation did not significantly reduce the rate of AF recurrence (34% after CA alone vs. 30% after CA combined with AADs) but significantly increased the proportion of asymptomatic AF episodes among patients with post-ablation arrhythmia recurrence (68% in patients with AADs and 28% in those without AAD after ablation) [70].
Clinical Benefits of AF Ablation
Data accumulated in the last 15 years suggest that CA, at least in some subsets of AF patients, could have important clinical benefits such as the reduction of systemic thromboembolism and mortality rate as well as improvement in HF management and QoL [2, 3, 25, 71,72,73,74,75,76].
Mortality and Thromboembolism
Randomized trials have not demonstrated superiority of ablation compared to medical therapy in reducing mortality and thromboembolic events, most probably because of the limited duration of post-procedural follow-up and selection of relatively younger patients with a low prevalence of structural heart disease and low thromboembolic risk [77]. However, several non-randomized studies showed advantages of CA over medical therapy with respect to survival and stroke prevention in the subgroups of “sicker” and older AF patients with significant heart disease, HF and a high CHA2DS2VASc score [71,72,73,74,75,76]. These studies included patients with mean age between 57 and 69 years and more than one risk factor for thromboembolism; more than half of the patients had significant structural heart or lung disease [71,72,73,74,75,76]. During the mean follow-up of 2.5–4.4 years, significantly lower mortality (3–6% vs. 7–14%) and thromboembolism rates (2–3% vs. 4–9%) were observed after ablation compared to AAD therapy. Moreover, a stable sinus rhythm after the procedure was strongly associated with a reduction in mortality [HR 0.14 (95% CI: 0.06 to 12.36)], while an AF recurrence was an independent predictor of vascular thromboembolic events [HR 2.52 (95% CI: 1.05 to 6.06)] [72, 74]. The stroke rate reduction was most prominent among patients with a high CHA2DS2VASc score of ≥2 [HR 0.39 (95% CI: 0.19 to 0.78)] [75].
Heart Failure
AF and HF share common risk factors for their development and progression (hypertension, diabetes, coronary and valvular disease, aging, etc.) [78]. Although the prevalence of AF increases proportionately to worsening of HF, in patients presenting with both AF and HF it is often difficult to determine a causal link between the two [79]. PeAF or frequent PAF episodes associated with a rapid ventricular rate may lead to secondary LV systolic dysfunction and congestive HF, a condition known as “tachycardiomyopathy” or tachyarrhythmia-induced HF [80]. The recovery of LV systolic function after restoration of sinus rhythm can last for months after the procedure, depending on the patient age, duration of pre-ablation AF episode and associated underlying heart disease. Approximately 10% of patients with AF and HF develop pure tachycardiomyopathy, and another 25–50% show a certain component of tachycardiomyopathy exacerbating preexisting HF [81].
The use of AADs and rate-controlling agents in HF is limited because of hypotension, worsening of congestive symptoms and possible ventricular pro-arrhythmia [79,80,81]. Therefore, a non-pharmacological treatment of AF such as CA is a desirable therapeutic option for HF patients [2, 78,79,80,81]. A randomized study demonstrated significantly better 2-year AF-free survival in patients with PeAF, congestive HF and EF <40% who underwent AF ablation (mean 1.4 procedures per patient) than in those who were treated with amiodarone (70% vs. 34%) [82].
In approximately 70% of AF patients with reduced LV systolic function (ejection fraction, EF <50%), a significant average increase of EF for 12–23% or normalization of EF to ≥55% can be expected after several months post ablation [80, 83]. Maintenance of sinus rhythm after the procedure was a clinical factor independently associated with an increase in LV EF for more than 10% [OR 4.26 (95% CI: 1.69 to 10.74)] [84]. In addition, several studies have demonstrated a significant increase in exercise tolerance and reduction of mitral regurgitation and number of hospitalizations for HF after successful AF-CA in HF patients [84, 85]. A rate of maintaining stable sinus rhythm in patients with HF was 48% after the first AF ablation increasing to 75% after the re-do procedure, while 32% of patients underwent multiple CA procedures [85].
Quality of Life Improvement
Symptomatic and functional improvement of patients is among the main goals of AF treatment [2, 3, 25, 27]. AF significantly reduces the physical and mental health components of QoL measured by generic and arrhythmia-specific questionnaires, such as the Short Form-36 (SF-36) score and Symptom Check List Frequency and Severity (SCL-F and SCL-S) scores [86, 87]. It has been shown that the QoL score returned to the pre-procedural level after only several weeks post ablation, staying at the initial level during a long-term follow-up [86]. The QoL improvement was strikingly higher in patients who were AF-free than in those with recurrent arrhythmia after the procedure [86,87,88]. However, even in patients with AF recurrence, a significant QoL improvement was observed following ablation compared to pre-ablation values, possibly because of the higher proportion of asymptomatic arrhythmia episodes, reduction in AF burden, LA denervation, increased AAD effectiveness or placebo effect post procedure [88].
Rhythm-Monitoring Strategy After AF Ablation
There is no consensus on the optimal rhythm-monitoring strategy after AF ablation procedures [2, 3]. In most cases, the procedural outcome is assessed using only clinical follow-up and findings of non-invasive rhythm-monitoring systems [2, 3, 89]. These non-invasive monitoring tools, including a standard 12-lead ECG, Holter, event-recorder, trans-telephonic transmission systems, etc., strongly depend on patient adherence [89]. Moreover, these systems are only capable of intermittent rhythm monitoring and are commonly activated by the patient, providing moderate sensitivity for post-procedural AF detection in the range from 31 to 71% [89]. Although these systems enable clinicians to evaluate the symptoms suggestive of AF relapse, such monitoring strategies can easily overlook subclinical short-lasting and sporadic AF recurrences after procedures [90]. The clinical decision on the long-term use of OAC therapy is often only based on the outcome of ablation procedures estimated by non-invasive rhythm-monitoring strategies [91]. However, the finding of short-term episodes of atrial tachyarrhythmia has been shown to be strongly associated with an increased risk of cryptogenic stroke, thus emphasizing the need for more reliable strategies for routine monitoring after AF ablation [92].
Implantable cardiac rhythm monitors (ICM) allow continuous rhythm monitoring for several months to years after the procedure [89, 90, 93]. ICM is armed with specific algorithms for automatic AF detection, demonstrating very high accuracy for AF detection of 98% [2, 89]. Recently, ICMs were implanted in 50 patients 3 months prior to AF ablation, and these patients were followed for 18 months after AF-CA [90]. The proportion of asymptomatic AF episodes increased significantly from 52% before ablation to 79% after ablation, changing the ratio of asymptomatic to symptomatic AF episodes from 1.1 before to 3.7 after the procedure. In addition, the median duration of AF episodes was significantly shortened from 22 min before to 6 min after ablation [90]. Importantly, the ultimate AF recurrence rate after multiple CA procedures, as estimated on the basis of post-procedure symptoms, periodic 48-h Holter and findings of ICM interrogation, was 58, 56 and 46%, because up to 12% of patients experienced exclusively asymptomatic AF recurrences after ablation [90]. Other studies reported similar findings [93]. These systems are still not routinely used in this clinical setting, likely because of their invasiveness and costs; however, they can be an option for selected patients [2].
Recurrence of AF After Ablation
AF recurrences after CA were arbitrarily defined as “early,” “late” and “very late”, because the time course of AF recurrence could implicate the mechanism as well as clinical significance of post-procedure atrial arrhythmia relapse [3].
Early Recurrence of AF
“Early” recurrences of AF (ERAF) usually occur during the first 1–3 months after the AF ablation procedure [3]. This vulnerable period after the procedure is called the “blanking period”, referring to the period of maturation and healing of RF lesions after LA ablation [94]. A high incidence of ERAF during the first weeks post ablation was reported, ranging between 30% and 70%, and the ERAF occurrence does not imply immediate re-do ablation [23, 94,95,96]. It was believed that transient LA tissue inflammation after RF ablation could be responsible for a significant proportion of the ERAF cases because in 40–60% of these patients arrhythmia recurrences gradually disappear in the weeks and months post CA [94,95,96,97]. In addition, it has been shown that antiinflammatory therapy (i.e., corticosteroids or colchicine) or AAD therapy during the first days and weeks after AF ablation can significantly reduce the ERAF occurrence, but with no impact on the long-term rhythm outcome [94,95,96]. It is therefore recommended to continue with AAD therapy during the 3-month blanking period after the procedure in all patients, hoping to reduce the risk of overt ERAF episodes requiring in-hospital cardioversion [2, 3, 96].
Current guidelines recommended a 3-month blanking period after AF ablation [3]. However, a recent study called into question the 90-day cutoff value, reporting a strong correlation between the timing of ERAF and late AF recurrence [97]. The 1-year freedom from AF was 62.6, 36.4 and only 7.8% in patients with ERAF occurrence within the first, second and third month post-PAF ablation, respectively (P < 0.0001), indicating the need for redefining the blanking period duration [97]. Other long-term follow-up studies after AF ablation confirmed these findings [98, 99]. During follow-up for up to 3 years after ablation, any ERAF occurrence was a strong and independent predictor of subsequent arrhythmia recurrence [98, 99]. In a recent prospective study, according to the study protocol all patients underwent a mandatory invasive EP procedure 2 months after the index PVI for PAF [100]. The presence of a late PV reconnection as well as the number of reconnected PVs at the repeated EP procedure significantly correlated with ERAF occurrence following the index CA [100].
Late and Very Late Recurrence of AF
AF recurrences occurring after the blanking period are considered as late recurrences of AF (LRAF) [3]. In repeated EP procedures, a reconnection of at least one PV was observed in 98% of patients with clinically manifested LRAF [3, 25, 69]. In addition, re-isolation of these PVs led to long-term AF suppression in the majority of these patients, suggesting a late PV reconnection post PVI as the main mechanism of LRAF [25]. So far, various clinical and biochemical (pre- and post-procedural) predictors of LRAF have been identified, such as a history of non-paroxysmal AF, LA enlargement, hypertension, obesity, diabetes mellitus, aging, HF, chronic renal insufficiency, preprocedural amiodarone failure, biochemical markers of inflammation (a higher preprocedural C-reactive protein level, natriuretic peptide level and neutrophil/lymphocyte ratio as well as a lower post procedural troponin serum level), MRI finding of significant atrial fibrosis, increased thromboembolic score (CHADS2 and CHA2DS2VASc), presence of non-PV triggers, ERAF occurrence post procedure and others [2, 3, 25, 69, 101,102,103,104,105,106,107,108,109]. In addition, several intraprocedural strategies were proposed for achieving an enduring PVI lesion, significantly reducing the LRAF rate (e.g., an optimal contact force between the catheter tip and tissue surface during RF ablation, the use of steerable long sheaths and the methods for unmasking and eliminating dormant LA-PV connections post PVI such as adenosine testing or ablation of PV encircling lesions until “loss of local pace capture”) [45, 110, 111].
Several studies have shown that the majority of the LRAFs occurred in the 1st and 2nd years after the procedure, and thereafter only a small number of new-onset AF relapses were documented [25]. Thus, among LRAF patients, arrhythmia recurrences were observed in approximately 75% of patients in the 1st year and in 90% of patients up to the end of 2 years post procedure [112]. However, other studies have shown conflicting findings and argue about the persistency of the long-term AF ablation results [99, 102]. In patients who were AF-free during the 1st year post procedure (and therefore were considered “cured”), a progressive increase in the rate of very late AF recurrence (VLRAF) was identified: 13% after 2 years, 35% after 4 years and 55% after 6 years [102]. The mechanisms of VLRAF have not been completely clarified. Although a PV reconnection was found at the re-do ablation procedure in the majority of patients with VLRAF (69-100%), several observations indicate that mechanisms other than a simple PV reconnection could be responsible for some VLRAF cases [101,102,103,104,105,106,107,108,109,110,111,112]. Compared to patients with LRAF, those with VLRAF had a significantly lower rate of AF foci within the LA and PVs (50% vs. 97% and 50% vs. 79%, respectively) and higher rate of AF foci within the right atrium (67% vs. 3%) [112]. In addition, in VLRAF patients, one-third of the AF foci identified at re-do procedures were the new AF foci, previously not ablated during the index procedure, and atrial tachycardia unrelated to the PVs was identified in more than a half of VLRAF patients [104]. Probably the various inherent risk factors (e.g., hypertension, aging, HF, etc.) promote the bi-atrial cardiomyopathy progression in spite of temporary “successful” AF ablation, leading to further arrhythmogenic substrate development and re-occurrence of atrial tachyarrhythmia after several years post CA [99].
Recently, several scoring systems, such as ALARMEc, APPLE, BASE-AF2 and MB-LATER, were specifically developed for the prediction of AF recurrence after ablation [98, 99, 105, 106]. All these scores included easily available clinical variables, providing better selection of patients for invasive procedures (or redo procedures) and optimal intensity and duration of rhythm monitoring after the procedure. Of note, the common constituents of all of these scores are three clinical features: pre-ablation history of non-paroxysmal AF and LA enlargement and ERAF occurrence post ablation [98, 99, 105, 106]. It would be of clinical value if the accurate prediction of the long-term procedural outcome could inform decisions on the duration of anticoagulant therapy post procedure.
Indication for AF Ablation
During management of AF patients in daily clinical practice, two questions commonly arise: (1) Who is a good candidate for CA of AF? (2) When in the clinical course of AF does the invasive procedure becomes medically justified for the patient? An overview of the indications for the AF ablation procedure is listed in Table 1.
The best candidates for CA are relatively younger patients with PAF and structurally normal heart or those with only minimal concomitant structural heart disease [2, 3, 25, 99,100,101,102,103,104,105,106,107,108,109, 113, 114]. An 85–90% single CA procedure success rate has been reported in younger patients with lone AF during the 3–5-year follow-up post procedure [113, 114].
The effectiveness of ablation compared to medical therapy was most pronounced in AF patients who had already failed AAD therapy [2, 115]. In patients with PAF refractory to at least one class IC or III drug, changing the AAD led to successful AF suppression in <20% of patients [115]. However, the long-term effectiveness of ablation in this setting approaches 70–75% [6]. Although invasive cardiac procedures involve life-threatening complications, long-term AAD therapy has been shown to be more commonly associated with considerable side effects compared to ablation (17% vs. 8%) [116]. In addition, a few studies have reported that CA can even be considered as the first therapeutic option for selected patients with PAF [114].
Anticoagulation Therapy After Ablation
There is no consensus about the duration of OAC therapy after ablation [2, 3]. In accordance with current recommendations, OAC drugs (vitamin K antagonists or non-vitamin K antagonist OAC) should be prescribed to all patients in the first 6 weeks to 3 months after the procedure. Thereafter, the indication for OAC should be based on the individual stroke risk (e.g., CHA2DS2-VASc score) irrespective of the post-procedural rhythm outcome [2, 3]. A retrospective study showed an overall stroke incidence of 1.5% during the median follow-up of 18 months after AF ablation, with half of all events occurring during the first month after the procedure [117]. Stroke risk scores such as the CHADS2, R2CHADS2 and CHA2DS2-VASc score were independent predictors of thromboembolic complications post procedure, while AF recurrence indicated only a non-significant trend for increased thromboembolic risk. Using the CHA2DS2-VASc score additionally stratified patients within the low-risk stratum as categorized by the CHADS2 and R2CHADS2 scores, especially in those with documented AF relapse after ablation [117]. However, controversy exists because it has recently been reported that all thromboembolic events after RF-CA of AF occurred in patients with an arrhythmia recurrence, with the rate of 4% during a mean follow-up of 5 years [91]. Moreover, routine continuation of warfarin following CA in patients with low-to-intermediate thromboembolic risk conferred greater hemorrhagic risk than the benefit from thromboembolic prevention [91]. Therefore, more accurate prediction and detection of late and very late AF recurrence after ablation could influence the decision about the continuation of long-term OAC therapy after the procedure [2, 89,90,91,92,93].
Conclusion
Electrical isolation of PVs is the cornerstone of the AF-CA procedure. CA is superior to AAD therapy for clinical suppression of AF. Long-term elimination of AF after ablation is achieved in 50–80% of patients, but repeated procedure(s) are often necessary for a successful outcome. The strongest predictors of AF recurrence after CA are a pre-procedural history of non-paroxysmal AF, LA enlargement and early recurrence of arrhythmia during the 3-month post-procedural blanking period. In patients with high thromboembolic risk, maintenance of sinus rhythm after ablation was associated with a decrease in the rates of death and stroke. In addition, in patients with heart failure, a significant recovery of LV systolic function following successful AF-CA was recorded. The best candidates for CA are younger patients with symptomatic PAF with no structural heart disease and no significant LA remodeling. In these patients, the QoL improvement and symptomatic relief were more pronounced after ablation than with AADs. Because of the 1–5% risk of life-threatening complications, ablation represents a secondary treatment option for selected patients with AF. Additional technological improvement should enable the achievement of more durable ablative lesions and the identification of an optimal and individually adjusted lesion set for CA of PeAF. Such advances could significantly expand the indication for AF-CA. Also, more information is necessary for determining the optimal rhythm monitoring and anticoagulation strategy after AF ablation.
References
Chung SS, Blackshear JL, Shen WK, Hammill SC, Gersh BJ. Epidemiology and natural history of atrial fibrillation: clinical implications. J Am Coll Cardiol. 2001;37:371–8.
Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016;18:1609–78.
Calkins H, Kuck KH, Cappato R, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm. 2012;9:632–96.
Calkins H, Reynolds MR, Spector P, et al. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm Electrophysiol. 2009;2:349–61.
Kumar S, Walters TE, Halloran K, et al. Ten-year trends in the use of catheter ablation for treatment of atrial fibrillation vs the use of coronary intervention for the treatment of ischaemic heart disease in Australia. Europace. 2013;15:1702–9.
Ganesan AN, Shipp NJ, Brooks AG, et al. Long-term outcomes of catheter ablation of atrial fibrillation: a systematic review and meta-analysis. J Am Heart Assoc. 2013;2:e004549.
Krummen DE, Hebsur S, Salcedo J, Narayan SM, Lalani GG, Schricker AA. Mechanisms underlying AF: triggers, rotors, other? Curr Treat Options Cardiovasc Med. 2015;17:371–86.
Assasi N, Xie F, Blackhouse G, et al. Comparative effectiveness of catheter ablation strategies for rhythm control in patients with atrial fibrillation: a meta-analysis. J Interv Card Electrophysiol. 2012;35:259–75.
Kumagai K. Box isolation for atrial fibrillation. J Arrhythmia. 2011;27:255–67.
Mun H-S, Joung B, Shim J, et al. Does additional linear ablation after circumferential pulmonary vein isolation improve clinical outcome in patients with paroxysmal atrial fibrillation? Prospective randomized study. Heart. 2012;98:480–4.
Haïssaguerre M, Sanders P, Hocini M. Catheter ablation of long-lasting persistent atrial fibrillation: critical structures for termination. J Cardiovasc Electrophysiol. 2005;11:1125–37.
Eitel C, Hindricks G, Sommer P, et al. Circumferential pulmonary vein isolation and linear left atrial ablation as a single-catheter technique to achieve bidirectional conduction block: the pace-and-ablate approach. Heart Rhythm. 2010;7:157–64.
Gaita F, Caponi D, Scaglione M, et al. Long-term clinical results of 2 different ablation strategies in patients with paroxysmal and persistent atrial fibrillation. Circ Arrhythm Electrophysiol. 2008;1:269–75.
Tilz RR, Rillig A, Thum AM, et al. Catheter ablation of long-standing persistent atrial fibrillation: 5-year outcomes of the Hamburg Sequential Ablation Strategy. J Am Coll Cardiol. 2012;60:1921–9.
Verma A, Jiang CY, Betts TR, STAR AF II Investigators, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–22.
Rolf S, Kircher S, Arya A, et al. Tailored atrial substrate modification based on low-voltage areas in catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7:825–33.
Miller JM, Kalra V, Das MK, et al. Clinical benefit of ablating localized sources for human atrial fibrillation: the Indiana University FIRM Registry. J Am Coll Cardiol. 2017;69:1247–56.
Krummen DE, Swarup V, Narayan SM. The role of rotors in atrial fibrillation. J Thorac Dis. 2015;7:142–51.
Haïssaguerre M, Shah DC, Jaïs P, et al. Electrophysiological breakthroughs from the left atrium to the pulmonary veins. Circulation. 2000;102:2463–5.
Lin WS, Tai CT, Hsieh MH, et al. Catheter ablation of paroxysmal atrial fibrillation initiated by non-pulmonary vein ectopy. Circulation. 2003;107:3176–83.
Stiles MK, John B, Wong CX, et al. Paroxysmal lone atrial fibrillation is associated with an abnormal atrial substrate. Characterizing the “second factor”. J Am Coll Cardiol. 2009;14:1182–91.
Cappato R, Calkins H, Chen SA, et al. Updated Worldwide Survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3:32–8.
Ouyang F, Bänsch D, Ernst S, et al. Complete isolation of left atrium surrounding the pulmonary veins: new insights from the double-lasso technique in paroxysmal atrial fibrillation. Circulation. 2004;110:2090–6.
Arentz T, Weber R, Bürkle G, et al. Small or large isolation areas around the pulmonary veins for the treatment of atrial fibrillation? Results from a prospective randomized study. Circulation. 2007;115:3057–63.
Mujović N, Marinković M, Potpara TS, Geller L. Catheter ablation of lone atrial fibrillation. Curr Pharm Des. 2015;21:591–612.
Hung Y, Lo LW, Lin YJ, et al. Characteristics and long-term catheter ablation outcome in long-standing persistent atrial fibrillation patients with non-pulmonary vein triggers. Int J Cardiol. 2017;241:205–11.
Potpara TS, Lip GY. Lone atrial fibrillation: what is known and what is to come. Int J Clin Pract. 2011;65:446–57.
Gal P, Marrouche NF. Magnetic resonance imaging of atrial fibrosis: redefining atrial fibrillation to a syndrome. Eur Heart J. 2017;38:14–9.
Fassini G, Riva S, Chiodelli R, et al. Left mitral isthmus ablation associated with PV Isolation: long-term results of a prospective randomized study. J Cardiovasc Electrophysiol. 2005;16:1150–6.
Sawhney N, Anand K, Robertson CE, Wurdeman T, Anousheh R, Feld GK. Recovery of mitral isthmus conduction leads to the development of macro-reentrant tachycardia after left atrial linear ablation for atrial fibrillation. Circ Arrhythm Electrophysiol. 2011;4:832–7.
Anousheh R, Sawhney NS, Panutich M, Tate C, Chen WC, Feld GK. Effect of mitral isthmus block on development of atrial tachycardia following ablation for atrial fibrillation. Pacing Clin Electrophysiol. 2010;33:460–8.
Nademanee K, McKenzie J, Kosar E, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044–53.
Lin YJ, Lo MT, Lin C, et al. Prevalence, characteristics, mapping, and catheter ablation of potential rotors in nonparoxysmal atrial fibrillation. Circ Arrhythm Electrophysiol. 2013;6:851–8.
Narayan SM, Shivkumar K, Krummen DE, Miller JM, Rappel WJ. Panoramic electrophysiological mapping but not electrogram morphology identifies stable sources for human atrial fibrillation. Stable atrial fibrillation rotors and focal sources relate poorly to fractionated electrograms. Circ Arrhythm Electrophysiol. 2013;6:58–67.
Katritsis DG, Pokushalov E, Romanov A, et al. Autonomic denervation added to pulmonary vein isolation for paroxysmal atrial fibrillation: a randomized clinical trial. J Am Coll Cardiol. 2013;17(62):2318–25.
Sucu M, Aytemir K, Yorgun H. Innappropriate sinus tachycardia after superior vena cava isolation in addition to pulmonary veins isolatin of paroxysmal atrial fibrillation cryoballoon ablation. J Atr Fibrillation. 2015;8:1270.
Villareal RP, Liu BC, Massumi A. Heart rate variability and cardiovascular mortality. Curr Atheroscler Rep. 2002;4:120–7.
Scharf C, Veerareddy S, Ozaydin M, et al. Atrial flutter during pulmonary vein isolation in patients with atrial fibrillation. J Am Coll Cardiol. 2004;43:2057–62.
Mohanty S, Mohanty P, Di Biase L, et al. Results form a single-blind, randomized study comparing the imacts of different ablation approaches on long-term procedure outcome in coexistent atrial fibrillation and flutter (APPROVAL). Circulation. 2013;127:1853–60.
Bai R, Di Biase L, Mohanty P, et al. Ablation of perimitral flutter following catheter ablation of atrial fibrillation: impact on outcomes from a randomized study (PROPOSE). J Cardiovasc Electrophysiol. 2012;23:137–44.
Kottkamp H, Berg J, Bender R, Rieger A, Schreiber D. Box Isolation of Fibrotic Areas (BIFA): a patient-tailored substrate modification approach for ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2016;27:22–30.
Jadidi AS, Lehrmann H, Keyl C, et al. Ablation of persistent atrial fibrillation targeting low-voltage areas with selective activation characteristics. Circ Arrhythm Electrophysiol. 2016;9:e002962.
Di Biase L, Burkhardt JD, Mohanty P, et al. Left atrial appendage isolation in patients with longstanding persistent AF undergoing catheter ablation: BELIEF Trial. J Am Coll Cardiol. 2016;68:1929–40.
Rillig A, Tilz RR, Lin T, et al. Unexpectedly high incidence of stroke and left atrial appendage thrombus formation after electrical isolation of the left atrial appendage for the treatment of atrial tachyarrhythmias. Circ Arrhythm Electrophysiol. 2016;9(5):e003461.
Kautzner J, Neuzil P, Lambert H, et al. EFFICAS II: optimization of catheter contact force improves outcome of pulmonary vein isolation for paroxysmal atrial fibrillation. Europace. 2015;17:1229–35.
Shurrab M, Di Biase L, Briceno DF, et al. Impact of contact force technology on atrial fibrillation ablation: a meta-analysis. J Am Heart Assoc. 2015;4:e002476.
Kuck KH, Brugada J, Fürnkranz A, On behalf of the FIRE and ICE Investigators, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. 2016;374:2235–45.
Luik A, Radzewitz A, Kieser M, et al. Cryoballoon vs open irrigated radiofrequency ablation in patients with paroxysmal atrial fibrillation: the prospective, randomized, controlled, noninferiority FreezeAF study. Circulation. 2015;132:1311–9.
Vogt J, Heintze J, Gutleben KJ, Muntean B, Horstkotte D, Nölker G. Long-term outcomes after cryoballoon pulmonary vein isolation: results from a prospective study in 605 patients. J Am Coll Cardiol. 2013;61:1707–12.
Aryana A, Singh SM, Kowalski M, et al. Acute and long-term outcomes of catheter ablation of atrial fibrillation using the second-generation cryoballoon vs open-irrigated radiofrequency: a multicenter experience. J Cardiovasc Electrophysiol. 2015;26:832–9.
Dukkipati SR, Cuoco F, Kutinsky I, et al. Pulmonary vein isolation using the visually guided laser balloon: a prospective, multicenter, and randomized comparison to standard radiofrequency ablation. J Am Coll Cardiol. 2015;66:1350–60.
Sohara H, Ohe T, Okumura K, et al. HotBalloon ablation of the pulmonary veins for paroxysmal af: a multicenter randomized trial in Japan. J Am Coll Cardiol. 2016;68:2747–57.
Hoffmann BA, Kuck K-H, Andresen D, et al. Impact of structural heart disease on the acute complication rate in atrial fibrillation ablation: results from the German ablation registry. J Cardiovasc Electrophysiol. 2014;25:242–9.
Michowitz Y, Rahkovich M, Oral H, et al. Effects of sex on the incidence of cardiac tamponade after catheter ablation of atrial fibrillation: results from a worldwide survey in 34 943 atrial fibrillation ablation procedures. Circ Arrhythm Electrophysiol. 2014;7:274–80.
Shoemaker MB, Muhammad R, Farrell M, et al. Relation of morbid obesity and female gender to risk of procedural complications in patients undergoing atrial fibrillation ablation. Am J Cardiol. 2013;111:368–73.
Aldhoon B, Wichterle D, Peichl P, Čihak R, Kautzner J. Complications of catheter ablation for atrial fibrillation in a high-volume centre with the use of intracardiac echocardiography. Europace. 2013;15:24–32.
Baman TS, Jongnarangsin K, Chugh A, et al. Prevalence and predictors of complications of radiofrequency catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2011;22:626–31.
Mujović N, Marinković M, Marković N, et al. Management and outcome of periprocedural cardiac perforation and tamponade with radiofrequency catheter ablation of cardiac arrhythmias: a single medium-volume center experience. Adv Ther. 2016;33:1782–96.
Chen J, Todd DM, Hocini M, Larsen TB, Bongiorni MG, Blomström-Lundqvist C. Current periprocedural management of ablation for atrial fibrillation in Europe: results of the European Heart Rhythm Association survey. Europace. 2014;16:378–81.
Mateos JC, Mateos EI, Peña TG, et al. Simplified method for esophagus protection during radiofrequency catheter ablation of atrial fibrillation-prospective study of 704 cases. Rev Bras Cir Cardiovasc. 2015;30:139–47.
Baranowski B, Saliba W. Our approach to management of patients with pulmonary vein stenosis following AF ablation. J Cardiovasc Electrophysiol. 2011;22:364–7.
Neumann T, Kuniss M, Conradi G, et al. Pulmonary vein stenting for the treatment of acquired severe pulmonary vein stenosis after pulmonary vein isolation: clinical implications after long-term follow-up of 4 years. J Cardiovasc Electrophysiol. 2009;20:251–7.
Ouyang F, Tilz R, Chun J, et al. Long-term results of catheter ablation in paroxysmal atrial fibrillation: lessons from a 5-year follow-up. Circulation. 2010;122:2368–77.
Medi C, Sparks PB, Morton JB, et al. Pulmonary vein antral isolation for paroxysmal atrial fibrillation: results from long-term follow-up. J Cardiovasc Electrophysiol. 2011;22:137–41.
Pokushalov E, Romanov A, Corbucci G, et al. Use of an implantable monitor to detect arrhythmia recurrences and select patients for early repeat catheter ablation for atrial fibrillation: a pilot study. Circ Arrhythm Electrophysiol. 2011;4:823–31.
Stabile G, Iuliano A, Agresta A, La Rocca V, D’Ascia S, De Simone A. Antiarrhythmic therapy following ablation of atrial fibrillation. Expert Rev Cardiovasc Ther. 2013;11:837–42.
Verma A, Kilicaslan F, Pisano E, et al. Response of atrial fibrillation to pulmonary vein antrum isolation is directly related to resumption and delay of pulmonary vein conduction. Circulation. 2005;112:627–35.
Kang KW, Kim TH, Park J, et al. Long-term changes in heart rate variability after radiofrequency catheter ablation for atrial fibrillation: 1-year follow-up study with irrigation tip catheter. J Cardiovasc Electrophysiol. 2014;25:693–700.
Hussein AA, Saliba WI, Martin DO, et al. Natural history and long-term outcomes of ablated atrial fibrillation. Circ Arrhythm Electrophysiol. 2011;4:271–8.
Turco P, De Simone A, La Rocca V, et al. Antiarrhythmic drug therapy after radiofrequency catheter ablation in patients with atrial fibrillation. Pacing Clin Electrophysiol. 2007;30:S112–5.
Pappone C, Rosanio S, Augello G, et al. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation. J Am Coll Cardiol. 2003;42:185–97.
Nademanee K, Schwab MC, Kosar EM, et al. Clinical outcomes of catheter substrate ablation for high-risk patients with atrial fibrillation. J Am Coll Cardiol. 2008;51:843–9.
Hunter RJ, McCready J, Diab I, et al. Maintenance of sinus rhythm with an ablation strategy in patients with atrial fibrillation is associated with a lower risk of stroke and death. Heart. 2012;98:48–53.
Lin Y-J, Chao T-F, Tsao H-M, et al. Successful catheter ablation reduces the risk of cardiovascular events in atrial fibrillation patients with CHA2DS2-VASc risk score of 1 and higher. Europace. 2013;15:676–84.
Friberg L, Tabrizi F, Englund A. Catheter ablation for atrial fibrillation is associated with lower incidence of stroke and death: data from Swedish health registries. Eur Heart J. 2016;37:2478–87.
Saliba W, Schliamser JE, Lavi I, et al. Catheter ablation of atrial fibrillation is associated with reduced risk of stroke and mortality: a propensity score-matched analysis. Heart Rhythm. 2017;14:635–42.
Dagres N, Varounis C, Flevari P, et al. Mortality after catheter ablation for atrial fibrillation compared with antiarrhythmic drug therapy. A meta-analysis of randomized trials. Am Heart J. 2009;158:15–20.
Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure. Treatment considerations for a dual epidemic. Circulation. 2009;119:2516–25.
Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. 2003;91:2D–8D.
Gentlesk PJ, Sauer WH, Gerstenfeld EP, et al. Reversal of left ventricular dysfunction following ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2007;18:9–14.
Man J, Marchlinski FE. Atrial fibrillation ablation and heart failure. Curr Cardiol Rep. 2012;14:571–6.
Di Biase L, Mohanty P, Mohanty S, et al. Ablation versus amiodarone for treatment of persistent atrial fibrillation in patients with congestive heart failure and an implanted device: results from the AATAC Multicenter Randomized Trial. Circulation. 2016;133:1637–44.
Hsu L-F, Jaïs P, Sanders P, et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004;351:2373–83.
Bunch TJ, May HT, Bair TL, et al. Five-year outcomes of catheter ablation in patients with atrial fibrillation and left ventricular systolic dysfunction. J Cardiovasc Electrophysiol. 2015;26:363–70.
Anselmino M, Matta M, Castagno D, Giustetto C, Gaita F. Catheter ablation of atrial fibrillation in chronic heart failure: state-of-the-art and future perspectives. Europace. 2016;18:638–47.
Wokhlu A, Monahan KH, Hodge DO, et al. Long-term quality of life after ablation of atrial fibrillation the impact of recurrence, symptom relief, and placebo effect. J Am Coll Cardiol. 2010;55:2308–16.
Reynolds MR, Walczak J, White SA, Cohen DJ, Wilber DJ. Improvements in symptoms and quality of life in patients with paroxysmal atrial fibrillation treated with radiofrequency catheter ablation versus antiarrhythmic drugs. Circ Cardiovasc Qual Outcomes. 2010;3:615–23.
Raine D, Langley P, Shepherd E, et al. Effect of catheter ablation on quality of life in patients with atrial fibrillation and its correlation with arrhythmia outcome. Open Heart. 2015;2:e000302.
Forleo GB, Casella M, Russo AD, et al. Monitoring atrial fibrillation after catheter ablation. J Atr Fibrillation. 2014;30(6):58–64.
Verma A, Champagne J, Sapp J, et al. Discerning the incidence of symptomatic and asymptomatic episodes of atrial fibrillation before and after catheter ablation (DISCERN AF): a prospective, multicenter study. JAMA Intern Med. 2013;173:149–56.
Gallo C, Battaglia A, Anselmino M, et al. Long-term events following atrial fibrillation rate control or transcatheter ablation: a multicenter observational study. J Cardiovasc Med (Hagerstown). 2016;17:187–93.
Ritter MA, Kochhäuser S, Duning T, et al. Occult atrial fibrillation in cryptogenic stroke: detection by 7-day electrocardiogram versus implantable cardiac monitors. Stroke. 2013;44:1449–52.
Pedrote A, Arana-Rueda E, García-Riesco L, et al. Paroxysmal atrial fibrillation burden before and after pulmonary veins isolation: an observational study through a subcutaneous leadless cardiac monitor. J Cardiovasc Electrophysiol. 2013;24:1075–82.
Deftereos S, Giannopoulos G, Kossyvakis C, et al. Colchicine for prevention of early atrial fibrillation recurrence after pulmonary vein isolation: a randomized controlled study. J Am Coll Cardiol. 2012;60:1790–6.
Koyama T, Tada H, Sekiguchi Y, et al. Prevention of atrial fibrillation recurrence with corticosteroids after radiofrequency catheter ablation: a randomized controlled trial. J Am Coll Cardiol. 2010;56:1463–72.
Roux J-F, Zado E, Callans DJ, et al. Antiarrhythmics after ablation of atrial fibrillation (5A Study). Circulation. 2009;120:1036–40.
Willems S, Khairy P, Andrade JG, et al. Redefining the blanking period after catheter ablation for paroxysmal atrial fibrillation: insights from the ADVICE (ADenosine following pulmonary Vein Isolation to target dormant Conduction Elimination) trial. Circ Arrhythm Electrophysiol. 2016;9:e003909.
Canpolat U, Aytemir K, Yorgun H, Şahiner L, Kaya EB, Oto A. A proposal for a new scoring system in the prediction of catheter ablation outcomes: promising results from the Turkish Cryoablation Registry. Int J Cardiol. 2013;169:201–6.
Mujović N, Marinković M, Marković N, et al. Prediction of very late arrhythmia recurrence after radiofrequency catheter ablation of atrial fibrillation: the MB-LATER clinical score. Sci Rep. 2017;7:40828.
Das M, Wynn GJ, Morgan M, et al. Recurrence of atrial tachyarrhythmia during the second month of the blanking period is associated with more extensive pulmonary vein reconnection at repeat electrophysiology study. Circ Arrhythm Electrophysiol. 2015;8:846–52.
Shah AN, Mittal S, Sichrovsky TC, et al. Long-term outcome following successful pulmonary vein isolation: pattern and prediction of very late recurrence. J Cardiovasc Electrophysiol. 2008;19:661–7.
Bertaglia E, Tondo C, De Simone A, et al. Does catheter ablation cure atrial fibrillation? Single-procedure outcome of drug-refractory atrial fibrillation ablation: a 6-year multicentre experience. Europace. 2010;12:181–7.
Sotomi Y, Inoue K, Ito N, et al. Incidence and risk factors for very late recurrence of atrial fibrillation after radiofrequency catheter ablation. Europace. 2013;15:1581–6.
Usui E, Miyazaki S, Taniguchi H, et al. Recurrence after “long-term success” in catheter ablation of paroxysmal atrial fibrillation. Heart Rhythm. 2015;12:893–8.
Kornej J, Hindricks G, Shoemaker MB, et al. The APPLE score: a novel and simple score for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation. Clin Res Cardiol. 2015;104:871–6.
Wójcik M, Berkowitsch A, Greiss H, et al. Repeated catheter ablation of atrial fibrillation: how to predict outcome? Circ J. 2013;77:2271–9.
Mohanty S, Mohanty P, Di Biase L, et al. Impact of metabolic syndrome on procedural outcomes in patients with atrial fibrillation undergoing catheter ablation. J Am Coll Cardiol. 2012;59:1295–301.
Chao TF, Ambrose K, Tsao HM, et al. Relationship between the CHADS2 score and risk of very late recurrences after catheter ablation of paroxysmal atrial fibrillation. Heart Rhythm. 2012;98:1185–91.
den Uijl DW, Delgado V, Tops LF, et al. Natriuretic peptide levels predict recurrence of atrial fibrillation after radiofrequency catheter ablation. Am Heart J. 2011;161:197–203.
Schaeffer B, Willems S, Sultan A, et al. Loss of pace capture on the ablation line during pulmonary vein isolation versus “dormant conduction”: is adenosine expendable? J Cardiovasc Electrophysiol. 2015;26:1075–80.
Masuda M, Fujita M, Iida O, et al. Steerable versus non-steerable sheaths during pulmonary vein isolation: impact of left atrial enlargement on the catheter-tissue contact force. J Interv Card Electrophysiol. 2016;47:99–107.
Hsieh M-H, Tai C-T, Lee S-H, et al. The different mechanisms between late and very late recurrences of atrial fibrillation in patients undergoing a repeated catheter ablation. J Cardiovasc Electrophysiol. 2006;17:231–5.
Saguner AM, Maurer T, Wissner E, et al. Catheter ablation of atrial fibrillation in very young adults: a 5-year follow-up study. Europace. 2016;euw378.
Namdar M, Chierchia GB, Westra S, et al. Isolating the pulmonary veins as first-line therapy in patients with lone paroxysmal atrial fibrillation using the cryoballoon. Europace. 2012;14:197–203.
Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303:333–40.
Noheria A, Kumar A, Wylie JV Jr, Josephson ME. Catheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic review. Arch Intern Med. 2008;168:581–6.
Kornej J, Hindricks G, Kosiuk J, et al. Renal dysfunction, stroke risk scores (CHADS2, CHA2DS2-VASc, and R2CHADS2), and the risk of thromboembolic events after catheter ablation of atrial fibrillation: the Leipzig Heart Center AF Ablation Registry. Circ Arrhythm Electrophysiol. 2013;6:868–74.
Acknowledgements
Funding
No funding or sponsorship was received for this study or publication of this article.
Authorship
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole and have given final approval to the version to be published.
Disclosures
Nebojša Mujović, Milan Marinković, Roland Tilz, Radosław Lenarczyk and Tatjana S. Potpara declare that they have no conflict of interest.
Compliance with Ethics Guidelines
The study was conducted in accordance with the Declaration of Helsinki of 1964 as revised in 2013. The study protocol was approved by the Institutional Review Board of each center. This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/51E8F0601AE98483.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Mujović, N., Marinković, M., Lenarczyk, R. et al. Catheter Ablation of Atrial Fibrillation: An Overview for Clinicians. Adv Ther 34, 1897–1917 (2017). https://doi.org/10.1007/s12325-017-0590-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-017-0590-z