
Abstract
Introduction
Androgen deprivation therapy (ADT) is a mainstay of treatment against advanced prostate cancer (PC). As a treatment goal, suppression of plasma testosterone levels to <50 ng/dl has been established over decades. Evidence is growing though that suppression to even lower levels may add further clinical benefit. Therefore, we undertook a pooled retrospective analysis on the efficacy of 1-, 3-, and 6-month sustained-release (SR) formulations of the gonadotropin-releasing hormone (GnRH) agonist triptorelin to suppress serum testosterone concentrations beyond current standards.
Methods
Data of 920 male patients with PC enrolled in 9 prospective studies using testosterone serum concentrations as primary endpoint were pooled. Patients aged 42–96 years had to be eligible for ADT and to be either naïve to hormonal treatment or have undergone appropriate washout prior to enrolment. Patients were treated with triptorelin SR formulations for 2–12 months. Primary endpoints of this analysis were serum testosterone concentrations under treatment and success rates overall and per formulation, based on a testosterone target threshold of 20 ng/dl.
Results
After 1, 3, 6, 9, and 12 months of treatment, 79%, 92%, 93%, 90%, and 91% of patients reached testosterone levels <20 ng/dl, respectively. For the 1-, 3-, and 6-month formulations success rates ranged from 80–92%, from 83–93%, and from 65–97% with median (interquartile range) serum testosterone values of 2.9 (2.9–6.5), 5.0 (2.9–8.7), and 8.7 (5.8–14.1) ng/dl at study end, respectively.
Conclusion
In the large majority of patients, triptorelin SR formulations suppressed serum testosterone concentrations to even <20 ng/dl. Testosterone should be routinely monitored in PC patients on ADT although further studies on the clinical benefit of very low testosterone levels and the target concentrations are still warranted.
Similar content being viewed by others


Introduction
Based on recent estimates, prostate cancer (PC) ranks first among all new male cancers in both the USA and Europe (21% in 2016 and 22.8% in 2012, respectively) [1, 2]. Testosterone is known to foster PC cell growth; thus, the backbone therapy of advanced PC is androgen deprivation (ADT). Approximately 90% of tumours respond to initial ADT, which may result in a marked symptom reduction and prolonged survival, even if androgen-independent disease eventually develops [3,4,5].
ADT was initially achieved surgically via bilateral orchiectomy. Gonadotropin-releasing hormone (GnRH) analogues emerging in the 1980s offered a novel approach to medical castration through suppression of the hypothalamic-pituitary-gonadal axis. One of these was triptorelin, which was shown to be up to 100 times more potent than the native GnRH in vitro and in vivo [6,7,8]. Its clinical development started in 1982 [3] and it was registered as the first GnRH agonist SR formulation worldwide in France in 1986. Today, GnRH agonists are used worldwide for ADT [9] with survival rates similar to surgical castration [10]. They reduce serum testosterone to castrate levels via the decrease in pituitary gonadotropin secretion that follows down-regulation of the pituitary GnRH receptors [11]. The ensuing hypoandrogenic environment results in glandular and tumour shrinkage and in an increase of interglandular connective tissue [4, 12, 13].
A testosterone level of 50 ng/dl (1.7 nmol/l) has been established as the standard castration threshold, which has been applied for over 40 years [14]. This threshold is widely accepted by regulatory authorities for the approval of GnRH analogues in the treatment of advanced PC [14, 15] and is also deemed adequate by the National Comprehensive Cancer Network (NCCN) [16]. The European Association of Urology (EAU) indeed also acknowledges the 50 ng/dl cut-off, but suggests 20 ng/dl (0.7 nmol/l) to be more appropriate as “better results are repeatedly observed with lower levels compared to 50 ng/dl” [17].
In fact, there is growing evidence that the extent of testosterone suppression during ADT in hormone-sensitive PC patients predicts a lower risk of and shorter time to androgen-independent progression or castration-resistant PC (CRPC), although so far most studies have been retrospective and sample sizes were rather small [4, 11, 14, 18,19,20]. Advances in the understanding of the principal mechanisms of PC progression and resistance to castration have led to new agents for CRPC such as the testosterone synthesis inhibitor abiraterone and the androgen receptor blocker enzalutamide. The improved survival in patients with metastatic CRPC when adding these agents to first-line ADT with GnRH analogues (or surgical castration) also indicates an important role of low testosterone levels in the treatment of advanced PC [21, 22].
Efficacy results of triptorelin 1-, 3-, and 6-month formulations in patients with advanced PC have been published based on the standard castration limit of serum testosterone of 50 ng/dl. Reports suggesting that serum testosterone levels below this standard threshold might lead to improved clinical outcomes [4, 11, 14, 18,19,20] prompted us to re-examine testosterone data from nine phase II to IV studies, which is so far the largest analysis examining the efficacy of ADT at a cut-off level of 20 ng/dl [3, 9, 23].
Methods
This is a retrospective pooled analysis of nine prospective clinical studies on the efficacy of triptorelin 1-, 3-, and 6-month SR formulations for advanced PC with overall 920 evaluable patients. Four studies were randomised controlled phase II studies, two were randomised controlled phase III studies, and three were non-controlled phase II to IV studies (Table 1). Primary endpoints always included testosterone assessments measured by either validated radioimmunoassay (RIA) or liquid chromatography tandem mass spectrometry (LC-MS/MS) [3, 9, 24, 25], which proved to show comparable results at both high and low testosterone concentrations. At the very low levels expected in men under ADT, RIA and LC–MS/MS are considered the most accurate and reliable methods.
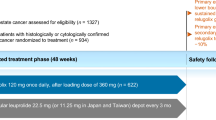
Patients were recruited in Europe and South Africa and had to have an indication for ADT, i.e., advanced or metastatic PC or rising prostate-specific antigen (PSA) after failed local therapy, were naïve to hormonal treatment or had undergone a 6-month washout period prior to study treatment, and presented with a normal baseline testosterone level at study entry. None of the patients except those in study E28-52014-701 (flutamide for 10 days) received any ADT. Concomitant treatments affecting the metabolism or secretion of testosterone were prohibited in all studies. Patients were treated with only one of the triptorelin formulations and investigated for 2–12 months (Fig. S1) except in study E28-52014-701 in which some patients were switched from the 1-month to the 3-month formulation (Table 1). All procedures performed in the original studies were in accordance with the ethical standards of institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all patients enrolled in the original studies; for the retrospective pooled analysis no formal consent is required.
Descriptive statistics were used to present demographic data, testosterone concentrations, and success rates. For the calculation of mean testosterone levels over various ranges of months, first the mean value for all available measurements over the indicated range of months was calculated for each patient without imputation for missing values, and then the mean and standard error (SE) for each group were calculated based on these means. For the comparison of baseline characteristics, Student’s t test and chi-square test were used. Data pooling and data management were done in SAS® (version 9.4) and MS Access 2013. Analyses were performed and figures created with R Core Team (2016).
Results
Mean age was similar among formulation groups with ages ranging from 42 to 96 years. Overall, half of the patients were Caucasian and one quarter black (Table 2). The 6-month formulation group had significantly higher testosterone levels as compared to the other two groups at baseline, i.e., means (95% CIs): 358.6 (345.8; 371.4) ng/dl in the 1-month formulation group and 383.1 (363.5; 402.7) ng/dl in the 3-month formulation as compared to 502.6 (467.4; 537.8) ng/dl in the 6-month formulation group (Table 2). The mean BMI was also higher in the 6-month formulation group as compared to the others.
The pooled data of all studies showed that a high proportion of patients achieved a testosterone level <20 ng/dl at the time points pre-defined in the protocols (i.e., months 1, 3, 6, 9, and 12), regardless of the formulation. Overall success rates based on the castration limit of 20 ng/dl reached 79% (95% CI: 75.9–81.3%) at month 1, 92% (89.7–93.6%) at month 3, 93% (90.4–94.4%) at month 6; 90% (87.2–92.0%) at month 9, and 91% (84.6–95.8%) at month 12. The success rates based on the standard castration limit of 50 ng/dl ranged from 95–99% (Fig. 1).

a Proportion of patients achieving a testosterone level <20 or <50 ng/dl at months 1, 3, 6, 9, and 12 after treatment with any triptorelin formulation. b Proportion of patients achieving a testosterone level <20 ng/dl overall and per each formulation (TRI1M: 1-month; TRI3M: 3-month; TRI6M: 6-month, the only formulation with 12-month data available). Tick marks indicate the exact 95% CI. N number of patients with testosterone data
Overall, mean testosterone levels were maintained <20 ng/dl over study periods for all formulations except for the 6-month formulation at months 1 and 12 (Fig. 2) because of single patients with exceptionally high levels (patient DEB-TRI6M-301-11-11613 with a value 422 ng/dl at month 1 and patient DEB-TRI6M-301-04-04602 with a value of 1213 ng/dl at month 12). Excluding those as outliers would result in mean values of 18.5 and 13.1 ng/dl, respectively.

Mean serum testosterone levels (ng/dl) versus selected time points (months) for each and all formulations—partly zoomed scale. The time values for the different formulations (all, TRI1M: 1-month, TRI3M: 3-month, and TRI6M: 6-month formulation) are slightly offset to distinguish the corresponding measurements for each formulation
Success rates per formulation in terms of the proportion of patients with testosterone <20 ng/dl ranged from 80–92% for the 1-month formulation, 83–93% for the 3-month formulation, and 65–97% for the 6-month formulation (Fig. 1b). The large majority of patients (89.7%) maintained stable low testosterone levels without two consecutive increases in serum testosterone to ≥20 ng/dl. Only very few patients (1.1%) experienced such testosterone escapes to ≥50 ng/dl. Pooling data from all formulations resulted in mean testosterone levels just above 10 ng/dl for months 1–6, 1–9, and 1–12. Testosterone still decreased between months 1 and 2 and mean values were <10 ng/dl for months 2–6, 2–9, and 2–12 (Fig. S2). At the end of the studies, median (IQR) serum testosterone values were 2.9 (2.9–6.5) ng/dl for the 1-month formulation, 5.0 (2.9–8.7) ng/dl for the 3-month formulation, and 8.7 (5.8–14.1) ng/dl for the 6-month formulation.
Discussion
Our analysis of pooled testosterone data was based on a total of almost 1000 patients and is, so far, the largest of its kind. The great majority of patients treated with triptorelin were shown to achieve and maintain testosterone levels <20 ng/dl. This is in line with two other retrospective studies reassessing testosterone levels achieved by either orchiectomy [14] or by use of polymer-delivered subcutaneous leuprolide acetate formulations [26]. Suppression of testosterone levels <20 ng/dl through ADT may thus be common and regardless of the formulation, although in our study, the testosterone decrease with the 6-month formulation appeared less rapid. However, this might have been due to a slightly different patient population as reflected by higher baseline BMI and testosterone levels. In fact, obese patients were reported to respond less to GnRH agonist treatment as compared to patients with normal BMI [27]. By contrast, the efficacy of the triptorelin 6-month formulation has recently been confirmed by a Danish study with patients under triptorelin showing significantly lower testosterone levels at months 3 and 6 than after subcapsular orchiectomy [28].
Still, some limitations of our study may need to be considered: Safety data of the nine studies were not pooled and re-analysed as the overall safety profile of triptorelin treatment in PC has recently been confirmed to be well-established and consistent among formulations as well [29]. A more relevant limitation might be inherent to the retrospective design. Although all included clinical trials were quite homogeneous in terms of design, quality, enrolled populations, and analytical methods for the measurement of testosterone, they were of rather short duration and did therefore not allow for an assessment of the time to androgen-independent progression (AIP) or death. Thus, the clinical benefit of achieving testosterone levels <20 ng/dl could actually not be addressed. However, evidence is growing that such a benefit indeed exists, even though most studies so far have been retrospective as well and rather small in size.
In 73 PC patients on ADT followed up for 51 months (range 1–20 years) the lowest serum testosterone cut-off that was able to discriminate regarding AIP-free survival was 32 ng/dl (88 vs. 137 months; P < 0.03). However, only breakthrough testosterone increases >50, but not >20 ng/dl had a significant impact on AIP-free survival [18]. In 225 Japanese PC patients treated with combined androgen blockade and followed up for 45.8 months, multivariate analysis revealed nadir testosterone <20 ng/dl to be the most significant prognostic factor of overall survival [20]. The risk of death was also shown to significantly correlate with 6-month serum testosterone levels in 129 patients with metastatic PC treated with goserelin and followed up for 47.5 months (range 22–72) [11]. In the largest and longest retrospective study so far with 626 PC patients having received ADT for a median of 8 years, nadir testosterone levels <20 ng/dl were shown to be associated with longer times to disease progression [30]. Conversely, patients with a median testosterone level >20 ng/dl had a significantly higher risk of developing CRPC. Maximum testosterone levels ≥50 ng/dl (23% of patients) were associated with a significantly higher rate of progression to CRPC as compared to patients with maximum testosterone <20 ng/dl (27%) and patients with nadir testosterone levels ≥50 ng/dl (1%) had a significantly higher risk of dying from disease as compared to patients with nadir testosterone 20–50 (21%) and <20 ng/dl (78%).
By contrast, there have been only two prospective studies on the additional benefit of suppressing testosterone to lower serum thresholds or minimum levels: In 32 patients followed up for about 2 years, time to CRPC was significantly longer in those with 9-month testosterone <32 ng/dl as compared to those with >32 ng/dl; however no additional predictive value was found for those <20 ng/dl [4]. In the second study, 153 patients with advanced PC were treated with GnRH agonists for 65 months. Testosterone levels <20 ng/dl after 6 months were found to be associated with a significantly lower risk of death and a trend towards a lower risk of disease progression (P = 0.12) as compared to those >20 ng/dl [19].
In conclusion, evidence is growing that sustainable testosterone suppression <20 ng/dl is beneficial in patients with PC. Reassuringly, this is widely achieved with all triptorelin SR formulations. Still, regular assessment of testosterone levels should be routine clinical practice for men on ADT and patients who under GnRH therapy do not succeed in achieving an appropriate testosterone suppression may qualify for an alternative method of ADT. Well-designed and sufficiently powered prospective studies using accurate and reliable testosterone assays are warranted to further evaluate the clinical benefit of a more rigorous testosterone suppression to minimum levels and to establish a new target threshold for testosterone levels.
References
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–403.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30.
Lundstrom EA, Rencken RK, van Wyk JH, Coetzee LJ, Bahlmann JC, Reif S, et al. Triptorelin 6-month formulation in the management of patients with locally advanced and metastatic prostate cancer: an open-label, non-comparative, multicentre, phase III study. Clin Drug Investig. 2009;29(12):757–65.
Dason S, Allard CB, Tong J, Shayegan B. Defining a new testosterone threshold for medical castration: results from a prospective cohort series. Can Urol Assoc J. 2013;7(5–6):E263–7.
Helgstrand JT, Berg KD, Lippert S, Brasso K, Roder MA. Systematic review: does endocrine therapy prolong survival in patients with prostate cancer? Scand J Urol. 2016;50(3):135–43 (Epub 2016/02/26).
Coy DH, Labrie F, Savary M, Coy EJ, Schally AV. LH-releasing activity of potent LH-RH analogs in vitro. Biochem Biophys Res Commun. 1975;67(2):576–82.
Nestor JJ Jr, Ho TL, Simpson RA, Horner BL, Jones GH, McRae GI, et al. Synthesis and biological activity of some very hydrophobic superagonist analogues of luteinizing hormone-releasing hormone. J Med Chem. 1982;25(7):795–801 (Epub 1982/07/01).
Millar RP, Troskie BE, Flanagan CA. Comparative receptor binding affinity and inositol phosphate production potency of D-Leu6 and D-Trp6 GnRH agonists on COS-1 cells transfected with the human GnRH receptor. XIII International congress of comparative endocrinology; 16–21 November; Yokohoma, Japan: Monduzzi Editore S.p.A. 1997; p. 559–62.
Heyns CF, Simonin MP, Grosgurin P, Schall R, Porchet HC. South African Triptorelin Study G. Comparative efficacy of triptorelin pamoate and leuprolide acetate in men with advanced prostate cancer. BJU Int. 2003;92(3):226–31.
Seidenfeld J, Samson DJ, Hasselblad V, Aronson N, Albertsen PC, Bennett CL, et al. Single-therapy androgen suppression in men with advanced prostate cancer: a systematic review and meta-analysis. Ann Intern Med. 2000;132(7):566–77.
Perachino M, Cavalli V, Bravi F. Testosterone levels in patients with metastatic prostate cancer treated with luteinizing hormone-releasing hormone therapy: prognostic significance? BJU Int. 2010;105(5):648–51.
Civantos F, Marcial MA, Banks ER, Ho CK, Speights VO, Drew PA, et al. Pathology of androgen deprivation therapy in prostate carcinoma. A comparative study of 173 patients. Cancer. 1995;75(7):1634–41.
Murphy WM, Soloway MS, Barrows GH. Pathologic changes associated with androgen deprivation therapy for prostate cancer. Cancer. 1991;68(4):821–8.
Oefelein MG, Feng A, Scolieri MJ, Ricchiutti D, Resnick MI. Reassessment of the definition of castrate levels of testosterone: implications for clinical decision making. Urology. 2000;56(6):1021–4.
Tombal B. The importance of testosterone control in prostate cancer. Eur Urol Suppl. 2007;6(15):834–9.
NCCN. Guidelines for treatment of cancer by site: prostate cancer. National comprehensive cancer network (NCCN), 2016 MT/W/0001/pdWS/001.
EAU. European association of urology (EAU) Guidelines on prostate cancer. 2016 MT/W/0001/pdWS/001.
Morote J, Orsola A, Planas J, Trilla E, Raventos CX, Cecchini L, et al. Redefining clinically significant castration levels in patients with prostate cancer receiving continuous androgen deprivation therapy. J Urol. 2007;178(4 Pt 1):1290–5.
Bertaglia V, Tucci M, Fiori C, Aroasio E, Poggio M, Buttigliero C, et al. Effects of serum testosterone levels after 6 months of androgen deprivation therapy on the outcome of patients with prostate cancer. Clin Genitourin Cancer. 2013;11(3):325–30.
Kamada S, Sakamoto S, Ando K, Muroi A, Fuse M, Kawamura K, et al. Nadir testosterone after long-term followup predicts prognosis in patients with prostate cancer treated with combined androgen blockade. J Urol. 2015;194(5):1264–70.
Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424–33.
Ryan CJ, Smith MR, de Bono JS, Molina A, Logothetis CJ, de Souza P, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138–48.
Teillac P, Heyns CF, Kaisary AV, Bouchot O, Blumberg J. Pharmacodynamic equivalence of a decapeptyl 3-month SR formulation with the 28-day SR formulation in patients with advanced prostate cancer. Horm Res. 2004;62(5):252–8.
Vesper HW, Botelho JC, Wang Y. Challenges and improvements in testosterone and estradiol testing. Asian J Androl. 2014;16(2):178–84.
Wang C, Catlin DH, Demers LM, Starcevic B, Swerdloff RS. Measurement of total serum testosterone in adult men: comparison of current laboratory methods versus liquid chromatography-tandem mass spectrometry. J Clin Endocrinol Metab. 2004;89(2):534–43 (Epub 2004/02/07).
Shore ND, Chu F, Moul J, Saltzstein D, Concepcion R, McLane JA, et al. Polymer-delivered subcutaneous leuprolide acetate formulations achieve and maintain castrate concentrations of testosterone in four open-label studies in patients with advanced prostate cancer. BJU Int. 2016. doi:10.1111/bju.13482 (Epub ahead of print).
Smith MR. Obesity and sex steroids during gonadotropin-releasing hormone agonist treatment for prostate cancer. Clin Cancer Res Off J Am Assoc Cancer Res. 2007;13(1):241–5.
Østergren P, Kistorp C, Fode M, Bennedbæk F, Faber J, Sonksen J. Luteinizing hormone releasing hormone agonists lower testosterone levels more than subcapsular orchiectomy: results from a randomized trial. J Urol. 2016;195(4):e324–5.
Merseburger AS, Hupe MC. An update on triptorelin: current thinking on androgen deprivation therapy for prostate cancer. Adv Ther. 2016;33(7):1072–93. doi:10.1007/s12325-016-0351-4.
Klotz L, O’Callaghan C, Ding K, Toren P, Dearnaley D, Higano CS, et al. Nadir testosterone within first year of androgen-deprivation therapy (ADT) predicts for time to castration-resistant progression: a secondary analysis of the PR-7 trial of intermittent versus continuous ADT. J Clin Oncol. 2015;33(10):1151–6.
Acknowledgements
Sponsorship for this study and article processing charges were funded by Debiopharm International, Switzerland, and Ipsen Pharma, France. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship of this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. Editorial assistance in the preparation of this manuscript was provided by Camilla Hansson of Debiopharm International and Uwe Totzke of Totzke & Dreher Scientific (TDS). Support for this assistance was funded by Debiopharm International.
Disclosures
E. Lundström is employed by Debiopharm International. D. Purcea is employed by Debiopharm International. W.P. Venetz is employed by Debiopharm International. P. Cabri is employed by Ipsen Pharma. P. Dutailly is employed by Ipsen Pharma. J. Breul and E. R. Goldfischer declare that they have no conflict of interest.
Compliance with Ethics Guidelines
This article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors.
Data Availability
The data sets generated during and/or analysed during the current study are not publicly available but may be made available by the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/6A47F06000FB6D7F.
Electronic supplementary material
Below is the link to the electronic supplementary material.
12325_2016_466_MOESM1_ESM.tif
Figure S1 Study duration per triptorelin formulation (TRI1M: 1-month; TRI3M: 3-month; TRI6M: 6-month). n = Number of patients (TIFF 1333 kb)
12325_2016_466_MOESM2_ESM.tif
Figure S2 Mean and 95% CI of SE of testosterone levels [ng/dL] over various ranges of months for all formulations combined. The mean value for all available measurements over the indicated range of months was calculated for each patient (missing values were not imputed). The mean and SE for each group (e.g. all patients with values between month 1 and month 6, the M1-6 group) was then calculated based on these means (TIFF 1334 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Breul, J., Lundström, E., Purcea, D. et al. Efficacy of Testosterone Suppression with Sustained-Release Triptorelin in Advanced Prostate Cancer. Adv Ther 34, 513–523 (2017). https://doi.org/10.1007/s12325-016-0466-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-016-0466-7