
Abstract
Introduction
We investigated the impact of reduced renal function on 24-h glucose variability in Japanese patients with type 2 diabetes mellitus (T2DM) treated with luseogliflozin.
Methods
In this double-blind, placebo-controlled, crossover study, 37 Japanese patients with T2DM [glycated hemoglobin (HbA1c) 7.0–10.0%] and estimated glomerular filtration rate (eGFR) ≥45 mL/min/1.73 m2 were randomized into two groups in which patients first received luseogliflozin then placebo, or vice versa, for 7 days each. Twenty-four-hour glucose variability was measured on day 7 in each period and was compared among patients divided into three groups according to their baseline eGFR (mL/min/1.73 m2): normal (≥90; n = 13; normal group), normal-to-mildly reduced renal function (≥75 to <90; n = 12; normal–mild group), and mild-to-moderately reduced renal function (<75; n = 9; mild–moderate group).
Results
The mean [95% confidence interval (CI)] placebo-subtracted 24-h cumulative urinary glucose excretion (g) was 82.1 (72.7, 91.5), 82.5 (73.4, 91.5), and 62.2 (51.2, 73.3); the placebo-subtracted 24-h mean glucose concentration (mg/dL) was −24.39 (−32.53, −16.26), −28.28 (−39.35, −17.22), and −11.53 (−23.93, 0.86); and the placebo-subtracted peak postprandial glucose (mg/dL) was −26.9 (−46.9, −6.9), −38.1 (−59.6, −16.6), and 1.5 (−25.5, 28.4) in the normal, normal–mild, and mild–moderate groups, respectively. The mean lowest glucose concentrations (placebo vs. luseogliflozin, mg/dL) decreased to similar levels in the normal (115.4 vs. 93.4), normal–mild (121.0 vs. 97.9), and mild–moderate (104.0 vs. 91.1) groups.
Conclusion
This post hoc subanalysis revealed that although mild-to-moderately reduced renal function attenuated the glucose-lowering effects of luseogliflozin on peak postprandial glucose, it did not attenuate the effects of luseogliflozin on fasting glucose. These findings may explain the smaller increase in urinary glucose excretion in these patients relative to patients with normal renal function or normal-to-moderately reduced renal function. Further studies may be needed to examine these findings in large populations of patients with T2DM and reduced renal function.
Trial registration
JapicCTI-142548.
Funding
Taisho Pharmaceutical Co., Ltd.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sodium–glucose cotransporter 2 (SGLT2) inhibitors are newly approved drugs that ameliorate hyperglycemia without increasing the risk of hypoglycemia or body weight gain compared with other glucose-lowering drugs [1–3]. Accordingly, they are included as one of the treatment options for combination therapy of type 2 diabetes mellitus (T2DM) in the current American Diabetes Association/European Association for the Study of Diabetes treatment recommendations [4].
Because the amount of glucose filtered through the glomerulus and urinary glucose excretion (UGE) are correlated with renal function [5], it is important to investigate the relationship between renal function/renal impairment and the efficacy of SGLT2 inhibitors. Indeed, it has been reported that the pharmacodynamics of SGLT2 inhibitors in diabetic subjects with renal impairment are consistent with the observation of reduced efficacy in these patients [6], and that some SGLT2 inhibitors are contraindicated in patients with chronic kidney disease, or their daily dose might need to be reduced [6].
Luseogliflozin is a highly selective and potent SGLT2 inhibitor [7, 8] approved for use as monotherapy or in combination with other antidiabetic drugs based on the results of the clinical trial program [9–11]. In a pharmacokinetic/pharmacodynamic study involving Japanese patients with T2DM, a single dose of luseogliflozin significantly increased 24-h UGE and significantly decreased fasting blood glucose and 2-h postprandial plasma glucose in patients with normal renal function, mildly reduced renal function, or moderately reduced renal function, but not in patients with severely reduced renal function [12]. Similar findings have been reported for other SGLT2 inhibitors in pharmacokinetic/pharmacodynamic studies and longer term studies [6].
To our knowledge, however, no studies have investigated the relationship between reduced renal function and daily glucose variability in patients treated with a SGLT2 inhibitor. Therefore, to investigate the potential impact of reduced renal function on 24-h glucose variability in patients treated with an SGLT2 inhibitor, we performed a subanalysis of our previously reported study in which patients were treated with luseogliflozin or placebo for 7 days in a crossover manner, with 24-h continuous glucose monitoring (CGM) starting on day 7 of treatment [13].
Methods
Ethics Statement
As previously described [13], the study was conducted in accordance with the ethical standards of the Helsinki Declaration of 1975, as revised in 2013, the Japanese Pharmaceutical Affairs Law, Good Clinical Practice, and institutional and national recommendations on clinical trials. The study protocol was approved by the Institutional Review Board of each institute. Written informed consent was obtained from all patients before enrolment. This study was registered with the Japan Pharmaceutical Information Center (identifier: JapicCTI-142548).
Study Design
In this double-blind, placebo-controlled, crossover study, 37 Japanese patients with T2DM inadequately controlled with diet and exercise (HbA1c 7.0–10.0%) whose estimated glomerular filtration rate (eGFR) was ≥45 mL/min/1.73 m2 were randomized into two groups in which patients first received luseogliflozin then placebo, or vice versa, for 7 days each. Each treatment period was separated by a washout period of 7–14 days. Patients were hospitalized on day 7 and consumed a standardized meal (536 kcal, with approximately 20% protein, 25% fat, and 55% carbohydrate) at breakfast, lunch, and dinner. Twenty-four-hour CGM was started on day 7. Because the data for one patient who left a relatively large amount of the standardized meal at breakfast and two patients who did not complete the 24-h CGM were excluded from this subanalysis, 34 patients were divided into three groups according to their baseline eGFR: normal (≥90 mL/min/1.73 m2; n = 13), normal-to-mildly reduced renal function (≥75 to <90 mL/min/1.73 m2; n = 12), or mild-to-moderately reduced renal function (<75 mL/min/1.73 m2; n = 9). We chose the cutoff value of 75 mL/min/1.73 m2 because this represents an intermediate value in stage 2 chronic kidney disease (defined as eGFR of ≥60 to <90 mL/min/1.73 m2) and provided similar numbers of patients in each group. To evaluate the difference between groups of patients in the difference between luseogliflozin and placebo, one-way analysis of variance (ANOVA) were used to analyze the normally distributed variables, and Kruskal–Wallis test were used to analyze the non-normally distributed variables.
Data Analysis
The primary endpoints of the original study were indices derived from CGM. Other efficacy endpoints were pharmacodynamic variables, including serum insulin concentrations, plasma glucagon concentrations, and urinary glucose concentrations (pooled urine and 24-h urine samples). The following variables were calculated using the CGM data: 24-h mean glucose, area under the curve (AUC), peak blood glucose concentration, time to peak blood glucose concentration, and blood glucose concentration in preprandial or fasting periods. The glucose concentration–time curves were analyzed for the following periods: 0–24 h, after breakfast (0–5 h), after lunch (5–11 h), after dinner (11–15 h), and the sleeping period (15–24 h). Pharmacodynamic variables included the AUC and the maximum concentration (C max) for serum insulin and plasma glucagon. Cumulative UGE was also calculated.
All statistical analyses were performed using SAS software (version 9.2; SAS Institute Inc., Cary, NC, USA). Mixed-effects models were used to analyze normally distributed variables, after visual inspection of the histogram for each variable. The mixed-effects models included treatment, sequence and period as fixed effects, and patient as a random effect. The least-squares mean differences between luseogliflozin and placebo with 95% confidence intervals (95% CI) were estimated for each variable in the mixed-effects models. Non-normally distributed variables were analyzed using Wilcoxon signed-rank test and the median and the interquartile range of differences between luseogliflozin and placebo were calculated.
To evaluate the difference between groups in the difference between luseogliflozin and placebo, ANOVA were used to analyze the normally distributed variables, and Kruskal–Wallis test were used to analyze the non-normally distributed variables.
Results
The demographic and baseline characteristics of the patients of each group are shown in Table 1. Although glucose-related variables tended to be lower in the mild–moderate group, there were no significant differences between groups.
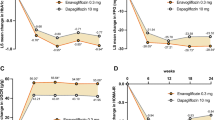
The variations in 24-h glucose concentrations measured by CGM and the UGE rates on day 7 of treatment with luseogliflozin and placebo are shown in Fig. 1. The 24-h glucose variables derived from CGM are shown in Table 2 and the pharmacodynamic variables are shown in Table 3.

a Twenty-four-hour glucose concentrations measured by continuous glucose monitoring (1 mg/dL = 0.0556 mmol/L). Values are presented as the mean (error bars were omitted for clarity). b Urinary glucose excretion rate. Values are as the mean + standard deviation. *P < 0.05 for luseogliflozin vs. placebo
Although glucose variability was consistently lower with luseogliflozin than with placebo in the normal and normal–mild groups, glucose variability was not consistently lower with luseogliflozin than with placebo in the mild–moderate group, because of the smaller change in postprandial glucose concentrations in this group.
The mean 24-h glucose was lower with luseogliflozin than with placebo in all three groups. However, the placebo-subtracted change in the mean 24-h glucose was smaller in the mild–moderate group than in the normal and normal–mild groups. The placebo-subtracted change in mean 24-h glucose was therefore significantly different between groups (P = 0.023, ANOVA).
The AUC0–24 h for glycemic variability was smaller with luseogliflozin than with placebo in all three groups. However, the placebo-subtracted change in the AUC0–24 h for glycemic variability was smaller in the mild–moderate group than in the normal and normal–mild groups. The placebo-subtracted change in the AUC0–24 h for glycemic variability was significantly different between groups (P = 0.023, ANOVA). The AUCs for glycemic variability after each meal (i.e., AUC0–5 h, AUC5–11 h, and AUC11–15 h) and during the sleeping period (AUC15–24 h) were also smaller with luseogliflozin than with placebo in all three groups. The placebo-subtracted AUCs for glycemic variability were significantly different between groups at breakfast and lunch (P = 0.006 and P = 0.026, respectively, ANOVA).
The peak glucose concentrations throughout the day and after each meal were significantly lower with luseogliflozin than with placebo in the normal and normal–mild groups, but not in the mild–moderate group. The placebo-subtracted difference in the peak glucose concentration was significantly different between groups after breakfast (P = 0.047, ANOVA), but not at the other measurement times.
The fasting glucose concentrations (i.e., glucose concentration measured before each meal and in the sleeping period) were consistently lower with luseogliflozin than with placebo in all three groups. Furthermore, the placebo-subtracted changes in the fasting glucose concentrations were not significantly different between groups.
The lowest glucose concentration from 0 to 24 h was lower with luseogliflozin than with placebo in all groups. The placebo-subtracted change in the lowest glucose concentration was not significantly different between groups.
Luseogliflozin significantly increased the cumulative UGE compared with placebo in all of the periods in all three groups (all P < 0.05). However, the placebo-subtracted changes in the cumulative UGE were smaller in the mild–moderate group than in the normal and normal–mild groups, and these differences were statistically significant between groups for all measurement times except after dinner (throughout the day: P = 0.007; after breakfast: P = 0.037; after lunch: P = 0.007; after dinner: P = 0.198; sleeping period: P = 0.050, ANOVA).
The serum insulin and plasma glucagon levels on day 7 in each treatment period are shown in Fig. 2. The serum insulin concentrations were consistently lower throughout the day with luseogliflozin than with placebo. The AUCs for serum insulin after each meal, during the sleeping period, and from 0 to 24 h were also smaller with luseogliflozin than with placebo in all three groups. The plasma glucagon concentrations were higher throughout the 24-h measurement period with luseogliflozin than with placebo, and the AUCs for plasma glucagon were higher with luseogliflozin than with placebo in almost all period in all groups. The placebo-subtracted differences in serum insulin- and plasma glucose-related variables were not significantly different between groups.

a Twenty-four-hour serum insulin levels after 7 days of once-daily administration of 2.5 mg luseogliflozin or placebo. Values are means + standard deviation. b Twenty-four-hour plasma glucagon levels after 7 days of once-daily administration of 2.5 mg luseogliflozin or placebo. Values are mean + standard deviation
Discussion
In this post hoc subanalysis, we investigated the impact of renal function decline on the glucose-lowering effects of luseogliflozin, including 24-h glucose variability, as well as pharmacodynamic variables. For the purpose of this subanalysis, we divided the patients into three groups based on their baseline eGFR: normal renal function, normal-to-mildly reduced renal function, and mild-to-moderately reduced renal function.
There were no significant differences in the demographic and baseline characteristics of between groups of patients, with the exceptions of eGFR and urinary albumin corrected for urinary creatinine.
We noted some differences in the variables derived from 24-h CGM among the three groups of patients. Although luseogliflozin decreased the fasting glucose concentrations (i.e., before each meal and in the sleeping period) in all three groups, it did not significantly reduce the postprandial glucose concentrations relative to placebo in the mild–moderate group. Furthermore, consistent with our original findings [13], luseogliflozin significantly increased the cumulative UGE compared with placebo in each of the three groups. However, the placebo-subtracted change in UGE was slightly smaller in the mild–moderate group than in the other two groups. This result is consistent with those of a previous study showing that UGE is attenuated in patients with renal impairment, owing to a reduction in glucose filtered through the glomeruli [12]. It seems feasible that luseogliflozin could not suppress the sharp glucose fluctuations in the postprandial periods in the mild–moderate group owing to the reduced amount of glucose that can be filtered through the glomerulus in individuals with reduced renal function. In normal conditions, the kidney can filter about 180 g of glucose per day, and this amount is likely to be reduced in individuals with reduced renal function. In fasting conditions (i.e., before each meal and overnight), the amount of glucose filtered through the kidney is likely to be relatively stable and manageable in all patients, albeit at a lower level in patients with reduced renal function than in patients with normal renal function. However, in patients with reduced renal function, the kidney is less able to respond to sudden increases in glucose concentrations, especially after a meal, limiting the impact of SGLT2 inhibitors on UGE. Nevertheless, the placebo-subtracted change in fasting glucose was smaller in the mild–moderate group than in the other groups, probably because of the lower baseline value in this group, being closer to the renal threshold for glucose reabsorption in the kidney [14]. The fasting glucose concentrations with luseogliflozin were similar between groups, which might be related to the renal threshold for glucose and the low risk of hypoglycemia in patients treated with SGLT2 inhibitors.
Luseogliflozin also decreased insulin concentrations and decreased the AUC of insulin in all of the groups. It is possible that these changes were driven by the reductions in circulating glucose concentrations. These findings suggest that luseogliflozin may reduce insulin secretion in patients with normal renal function or mildly reduced renal function. It is also notable that luseogliflozin increased plasma glucagon concentrations throughout the day in all three groups. This effect of luseogliflozin may be due to enhanced gluconeogenesis to prevent excessive reductions in circulating glucose, especially in fasting conditions.
Several pharmacokinetic/pharmacodynamic studies have demonstrated that the effects of SGLT2 inhibitors on UGE and plasma glucose concentrations are attenuated by reduced renal function, especially severely reduced renal function or chronic kidney disease [6, 15–18], consistent with our findings using 24-h CGM. Our results provide further insight into the impact of reduced renal function on the glucose-lowering effects of SGLT2 inhibitors, and that co-administration of a SGLT2 inhibitor with another antidiabetic drug, which improves postprandial glucose, might be useful for the patients with reduced renal function if improvements in glucose concentrations are not observed with monotherapy. It is particularly notable that the effects of luseogliflozin on postprandial glucose concentrations were attenuated in individuals with mild–moderate reductions in renal function relative to the other groups, but the reduction in fasting blood glucose was essentially unaffected by reduced renal function. Therefore, the reduced efficacy of SGLT2 inhibitors on overall glycemic control (i.e., HbA1c) is likely to be driven by the smaller reductions in postprandial glucose fluctuations, a major contributor to overall glycemic variability.
It is also important to consider that reduced renal function may increase systemic exposure to luseogliflozin, as has been demonstrated for dapagliflozin [19]. An increase in exposure may increase the risk of unwanted side effects, and dose adjustments may be necessary in individuals with moderate-to-severely reduced renal function, although this possibility must be evaluated in longer term studies of patients with moderate-to-severely reduced renal function.
Some limitations of this study warrant mention. In particular, because these subanalyses were conducted in a post hoc exploratory manner, the number of patients differed between groups. Accordingly, it will be necessary to conduct prospective studies of larger numbers of patients to examine the impact of reduced renal function on the glucose-lowering effects of luseogliflozin and the implications, if any, on the clinical use of luseogliflozin. In addition, we did not enroll patients with moderate-to-severely reduced renal function. Considering that the changes in glucose-related variables were lower in the mild–moderate group than in the normal and normal–moderate groups, it is possible that moderate-to-severely reduced renal function will attenuate the clinical efficacy of luseogliflozin by reducing UGE and affecting glucose variability. Indeed, in a 24-week randomized, placebo-controlled trial of Japanese patients with T2DM, ipragliflozin significantly improved glycemic control in patients with mildly reduced renal function but not in patients with moderately reduced renal function [20]. However, it was reported that canagliflozin significantly reduced HbA1c, body weight, and blood pressure among patients with stage 3 chronic kidney disease (defined as eGFR ≥30 to <60 mL/min/1.73 m2) [21]. Therefore, it will be necessary to evaluate the efficacy of luseogliflozin in patients with moderate-to-severely reduced renal function and in patients with mildly reduced renal function. Finally, patients were only administered luseogliflozin and placebo for 7 days each. Therefore, longer studies are required to examine the clinical relevance of the present results in terms of the changes in HbA1c.
Conclusions
The results of this post hoc subanalysis indicate that the effects of luseogliflozin on lowering postprandial glucose are attenuated in patients with mild-to-moderately reduced renal function (eGFR <75 mL/min/1.73 m2). Nevertheless, the improvements in fasting glucose concentrations measured before each meal and during the sleeping period and the reductions in insulin concentrations in patients with mild-to-moderately reduced renal function were similar to those in patients with normal renal function or patients with normal-to-mildly reduced renal function. These findings suggest that luseogliflozin improves fasting glucose concentrations, at least, without increasing the burden on pancreatic β-cells in patients with mild-to-moderately reduced renal function. Furthermore, the results suggest that luseogliflozin can be used in combination with other oral antidiabetic agents, which improve postprandial glucose, in patients with reduced renal function.
References
Bays H. Sodium glucose co-transporter type 2 (SGLT2) inhibitors: targeting the kidney to improve glycemic control in diabetes mellitus. Diabetes Ther. 2013;4:195–220.
Kurosaki E, Ogasawara H. Ipragliflozin and other sodium-glucose cotransporter-2 (SGLT2) inhibitors in the treatment of type 2 diabetes: preclinical and clinical data. Pharmacol Ther. 2013;139:51–9.
Tahrani AA, Barnett AH, Bailey CJ. SGLT inhibitors in management of diabetes. Lancet Diabetes Endocrinol. 2013;1:140–51.
American Diabetes Association. Standards of medical care in diabetes—2015. Diabetes Care. 2015;38(Suppl. 1):S1–94.
Rave K, Nosek L, Posner J, Heise T, Roggen K, van Hoogdalem EJ. Renal glucose excretion as a function of blood glucose concentration in subjects with type 2 diabetes-results of a hyperglycaemic glucose clamp study. Nephrol Dial Transpl. 2006;21:2166–71.
Scheen AJ. Pharmacokinetics, pharmacodynamics and clinical use of SGLT2 inhibitors in patients with type 2 diabetes mellitus and chronic kidney disease. Clin Pharmacokinet. 2015;54:691–708.
Takahashi T, Yamamoto K. Pharmacological and clinical profile of a new SGLT2 inhibitor, luseogliflozin (Lusefi(®)). Nihon Yakurigaku Zasshi. 2015;146:150–8.
Markham A, Elkinson S. Luseogliflozin: first global approval. Drugs. 2014;74:945–50.
Seino Y, Inagaki N, Haneda M, et al. Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus. J Diabetes Investig. 2015;6:443–53.
Seino Y, Kaku K, Inagaki N, et al. Fifty-two-week long-term clinical study of luseogliflozin as monotherapy in Japanese patients with type 2 diabetes mellitus inadequately controlled with diet and exercise. Endocr J. 2015;62:593–603.
Seino Y, Sasaki T, Fukatsu A, Ubukata M, Sakai S, Samukawa Y. Efficacy and safety of luseogliflozin as monotherapy in Japanese patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled, phase 3 study. Curr Med Res Opin. 2014;30:1245–55.
Haneda M, Seino Y, Sasaki T, et al. The effect of luseogliflozin (TS-071), a selective SGLT2 inhibitor, on pharmacodynamics and pharmacokinetics in Japanese type 2 diabetic subjects with renal impairment. Diabetes. 2012;61:A273.
Nishimura R, Osonoi T, Kanada S, et al. Effects of luseogliflozin, a sodium-glucose co-transporter 2 inhibitor, on 24-h glucose variability assessed by continuous glucose monitoring in Japanese patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled, crossover study. Diabetes Obes Metab. 2015;17:800–4.
Gerich JE. Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: therapeutic implications. Diabet Med. 2010;27:136–42.
O’Connor-Semmes R, Walker S, Kapur A, et al. Pharmacokinetics and pharmacodynamics of the SGLT2 inhibitor remogliflozin etabonate in subjects with mild and moderate renal impairment. Drug Metab Dispos. 2015;43:1077–83.
Zambrowicz B, Lapuerta P, Strumph P, et al. LX4211 therapy reduces postprandial glucose levels in patients with type 2 diabetes mellitus and renal impairment despite low urinary glucose excretion. Clin Ther. 2015;37(71–82):e12.
Sarashina A, Ueki K, Sasaki T, et al. Effect of renal impairment on the pharmacokinetics, pharmacodynamics, and safety of empagliflozin, a sodium glucose cotransporter 2 inhibitor, in Japanese patients with type 2 diabetes mellitus. Clin Ther. 2014;36:1606–15.
Macha S, Mattheus M, Halabi A, Pinnetti S, Woerle HJ, Broedl UC. Pharmacokinetics, pharmacodynamics and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, in subjects with renal impairment. Diabetes Obes Metab. 2014;16:215–22.
Kasichayanula S, Liu X, Pe Benito M, et al. The influence of kidney function on dapagliflozin exposure, metabolism and pharmacodynamics in healthy subjects and in patients with type 2 diabetes mellitus. Br J Clin Pharmacol. 2013;76:432–44.
Kashiwagi A, Takahashi H, Ishikawa H, Yoshida S, Kazuta K, Utsuno A, Ueyama E. A randomized, double-blind, placebo-controlled study on long-term efficacy and safety of ipragliflozin treatment in patients with type 2 diabetes mellitus and renal impairment: results of the long-term ASP1941 safety evaluation in patients with type 2 diabetes with renal impairment (LANTERN) study. Diabetes Obes Metab. 2015;17(2):152–60.
Yamout H, Perkovic V, Davies M, et al. Efficacy and safety of canagliflozin in patients with type 2 diabetes and stage 3 nephropathy. Am J Nephrol. 2014;40:64–74.
Acknowledgments
This study was supported by Taisho Pharmaceutical Co., Ltd, Tokyo, Japan. The article processing charges and open access fee for this publication were funded by Taisho Pharmaceutical Co., Ltd. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. The authors wish to thank Nicholas D. Smith, PhD, of Edanz Group Ltd., for providing editorial support, which was funded by Taisho Pharmaceutical Co., Ltd.
Disclosures
Hideaki Jinnouchi has received consultancy fees, research support fees or lecture fees from Abbott Diabetes Care, Inc., Astellas Pharma US, Inc., AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim Pharmaceuticals, Inc., Daiichi Sankyo Co., Ltd., Eli Lilly Japan K.K., Kyowa Hakko Kirin Co., Ltd., Novo Nordisk Pharma Ltd., Pfizer inc., Sanofi K.K., Kowa Pharmaceuticals, MSD, K.K., Taisho Toyama Pharmaceutical Co., Ltd., and Takeda Pharmaceutical Company Limited. Kazunari Nozaki, Hirotaka Watase, Hirohisa Omiya, Soichi Sakai, and Yoshishige Samukawa are employees of Taisho Pharmaceutical Co., Ltd., which is developing luseogliflozin.
Compliance with Ethics Guidelines
The study was conducted in accordance with the ethical standards of the Helsinki Declaration of 1975, as revised in 2013, the Japanese Pharmaceutical Affairs Law, Good Clinical Practice, and institutional and national recommendations on clinical trials. The study protocol was approved by the Institutional Review Board of each institute. Written informed consent was obtained from all patients before enrolment. This study was registered with the Japan Pharmaceutical Information Center (identifier: JapicCTI-142548).
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Jinnouchi, H., Nozaki, K., Watase, H. et al. Impact of Reduced Renal Function on the Glucose-Lowering Effects of Luseogliflozin, a Selective SGLT2 Inhibitor, Assessed by Continuous Glucose Monitoring in Japanese Patients with Type 2 Diabetes Mellitus. Adv Ther 33, 460–479 (2016). https://doi.org/10.1007/s12325-016-0291-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-016-0291-z