
Abstract
Lipoprotein lipase (LPL) polymorphism correlated with LPL activity is associated with plasma lipid and lipoprotein levels. We aimed to investigate the frequency of LPL PvuII polymorphism and effects of LPL PvuII polymorphism and niacin intake on the prevalence of metabolic syndrome (MetSyn) in Koreans. Lifestyle questionnaires, anthropometry, and dietary records were completed, and LPL PvuII polymorphism, LPL mass, and lipid profiles were determined in 548 Koreans (MetSyn: 278, Non-MetSyn: 270). The MetSyn group showed a significantly lower frequency of P1P1 (wild type) and a higher frequency of P1P2 (hetero type) than the non-MetSyn group. The P2P2 (mutant type) group significantly showed lower levels of HDLc and LPL mass and a higher level of TG than the P1P1 group. As niacin intake increased, LPL mass decreased in the P2P2 group (r 2 = 0.07). In particular, the lowest niacin intake group (≤14.82 mg/day) increased more than 3 times with regard to a higher risk of MetSyn than the others in the P2P2 mutant groups. However, the MetSyn risk declined 74% at the optimal levels of niacin intake (14.83–17.80 mg/day) in the P2P2 group compared to those of the P1 allele group. The findings indicate that optimal levels of niacin intake effectively decreased Korean MetSyn prevalence in the P2P2 mutant group.
Similar content being viewed by others


Introduction
Metabolic syndrome is prevalent worldwide and is highly associated with morbidity and mortality for chronic diseases such as diabetes, hypertension, and cardiovascular diseases. Especially in Korea, metabolic syndrome (MetSyn) poses a serious problem; 1 of every 4 adults is affected and 30% of obese children are susceptible to this syndrome (Ministry of Health and Welfare 2006; Haung et al. 2007). Standardized criteria for the diagnosis of MetSyn can be modified according to the race and sex of the affected individuals (Ekelund et al. 2009; Pan et al. 2008; Levesque and Lamarche 2008; Motta et al. 2009). Among various criteria, lipid and lipoprotein levels are associated with lipoprotein lipase (LPL) activity. LPL is synthesized and secreted by the parenchymal cells of extrahepatic tissues, mainly the adipose tissue and then transported to the luminal surface of vascular endothelial cells of the tissues (Sakayama et al. 2001). The human LPL catalyzes a key step in the removal of TG from the circulation, generating fatty acids for storage in the adipose tissue or for oxidation in the skeletal muscle. Hydrolysis of TG by LPL raises HDLc levels (Ukkola et al. 2001). LPL PvuII polymorphism is the result of C → T transition in the restriction site of the LPL gene intron 6, 1.57 kb from the splice acceptor (Fisher et al. 1987; Gotoda et al. 1989; Ahn et al. 1993). LPL PvuII polymorphism was related to the incidence of carotid artery disease, because the P2 mutant allele was associated with high TG and low HDLc levels (Chamberlain et al. 1989). The P2P2 genotype showed higher TG and lower HDLc levels in Koreans (Chung et al. 1999). The P2 allele is also positively correlated with body mass index, which is one of the risk factors for coronary artery disease in Koreans (Park et al. 2000).
Niacin (nicotinic acid or vitamin B3) is considered a broad-spectrum lipid-modulating agent and generates significantly beneficial effects on atherogenic dyslipidemia (Chapman et al. 2010). Meanwhile, the pharmacological level of niacin required to treat lipid disorders and CVD is 1–2 g/day; it decreases the TG, VLDLc, and lipoprotein(a) levels and increases the HDLc level (Kamanna and Kashyap 2008). Niacin prevents free fatty acids from mobilizing from the peripheral adipose tissue to the liver, which leads to a decrease in hepatic synthesis of TG and VLDL, and then it causes the releasing of smaller VLDL holding less TG (Rosenson 2009). In addition, niacin decreases synthesis of apoB, which is vital to assemble VLDL particles, and promotes the catabolism of VLDL through induction of LPL (Rosenson 2009). Although useful effects of niacin on lipids have been shown in populations with MetSyn, diabetes, and atherosclerosis (Canner et al. 2006; Vittone et al. 2007), an overdose of niacin (>2,000 mg/day) causes flushing, nausea, vomiting, hepatic toxicity, and glucose intolerance (McKenney 2003; Al-Shaer and AbuSabha 2004). However, there has been no research focusing on niacin intake corresponding to the RI for prevention of MetSyn or on the correlation between LPL gene polymorphisms, LPL mass, and niacin intake. Therefore, this study was conducted to investigate the association of lipid profiles, LPL mass, and lifestyle factors related to MetSyn prevalence according to LPL PvuII polymorphism. In addition, our study aimed to determine the effects of dietary niacin, one of the suitable drugs for dyslipidemia, on MetSyn prevalence in people with the LPL PvuII polymorphism.
Subjects and methods
Subjects
This Korean MetSyn Research Initiatives (KMSRI)-Seoul Study was conducted for the diagnosis and treatment of MetSyn and for the development of new techniques for MetSyn among Koreans. The inclusion criteria were as follows: sex, men or women; age, >20 years; fasting glucose (FBS) level, >5.6 mmol/L; blood pressure (BP), >130/85 mmHg; waist circumference (WC), >90 cm for men and >85 cm for women; HDLc level, <1.0 mmol/L for men and <1.3 mmol/L for women; TG level, >1.7 mmol/L. MetSyn was defined when >3 out of 5 modified NCEP ATP III and IDF criteria were fulfilled and non-MetSyn, when <2 out of 5 modified NCEP ATP III and IDF criteria were met (Pan et al. 2008; Tan et al. 2004; Lottenberg et al. 2007). Exclusion criteria consisted of previous dyslipidemia cases treated with any lipid-lowering drug, including niacin and familial lipid disorders. The study subjects comprised 548 outpatients (374 men; 174 women) who visited the Seoul Medical Center and Severance Hospital, Yonsei University, from May 2006 to June 2007. The subjects voluntarily participated in this study and provided physical measurements, underwent biochemical tests, and completed a lifestyle questionnaire at their first visit. Of the 548 subjects, only 269 underwent a nutrition examination at the second visit, since those with missing data were excluded. All the study subjects signed the consent forms for genetic examination and participation in the Seoul City R and BD program, based on the law on Bioethics and Safety.
Medical history and anthropometry
The subjects were not only asked about demographic characteristics such as age and sex but also about their history of exercise (yes/no), cigarette smoking (current smoker, ex-smoker, or non-smoker), and alcohol consumption (current drinker, ex-drinker, or non-drinker). BMI (kg/m2) was calculated from height and weight. WC was horizontally gauged at 3 cm above the umbilicus without pushing the skin. For BP, systolic blood pressure (mmHg) and diastolic blood pressure (mmHg) were measured by placing a suitably sized cuff on the arm circumference after resting for at least 5 min.
Biochemical analysis
Blood was collected after fasting for >12 h; whole blood and serum were stored at −80°C for gene and biochemical analysis, respectively. The risk factors for MetSyn—FBS, TC, TG, and HDLc levels—were measured using the Hitachi-7600 analyzer (Hitachi Ltd., Tokyo, Japan), and LDLc level was calculated using the Friedewald formula, i.e., TC—HDLc—(TG/5) (Friedewald and Gotto 2000). Insulin level was determined by enzyme-linked immunosorbent assay (ELISA; Mesdia Co., Seoul, Korea), and an index of insulin resistance, i.e., homeostasis model assessment of insulin resistance (HOMA-IR), was calculated by the formula of Matthews et al., i.e., fasting plasma insulin (μU/mL) × fasting plasma glucose (mmol/mL)/22.5 (Matthews et al. 1985).
LPL mass
Instead of LPL activity, LPL mass, which is proved to have a strongly positive correlation with LPL activity (r = 0.70, P < 0.0001), was estimated (Kastelein et al. 2000). LPL mass in the heparin-treated plasma was measured by sandwich ELISA, using a specific monoclonal antibody against bovine milk LPL, as described by Kobayashi et al. (1993, 2007). A commercial kit procured from Daiichi Pure Chemicals (Tokyo, Japan) was used.
LPL gene polymorphism analysis
LPL gene polymorphism was analyzed by polymerase chain reaction (PCR)-restriction length fragment polymorphism (RFLP) analysis (Botstein et al. 1980). After collection of blood in an ethylenediaminetetraacetic acid (EDTA) tube, template DNA was extracted using the LaboPass™ Blood Mini DNA Purification Kit (Cosmo Genetech, Seoul, Korea) and stored at −80°C until analysis.
The primers (located on intron 6) used for LPL PvuII polymorphism analysis were as follows: 5′-TAGAGGTTGAGGCACCTGTGC-3′ (forward) and 5′-GTGGGTGAATCACCTGAGG-3′ (reverse). The complex for determining the response was prepared by taking 100–200 ng of genomic DNA as the template and mixing 0.5 μM each of the forward and reverse primers, 10× PCR buffer (50 mM KCl, 10 mM Tris–HCl [pH 8.3], 2 mM MgCl2), 2.5 units of Taq DNA polymerase (KOMA Biotech Inc., Seoul, Korea), 200 μM of deoxynucleotide triphosphates (dNTPs), and 50 μL distilled water. The complex was denatured at 94°C for 5 min in iCycler iQ™ multi-color real time PCR system (Bio-Rad, Hercules, CA, USA) and then amplified (30 cycles) at 94°C for 1 min, at 65°C for 2 min, and at 72°C for 2 min. PvuII restriction enzyme was added to the amplified PCR products, after which they were incubated at 37°C for 2 h. Electrophoresis was then performed on 2% agarose gel, and the results were confirmed with an ultraviolet transilluminator after ethidium bromide staining. Only 858-bp band, both 858-bp band and division into 592- and 266-bp bands, and only division into 592- and 266-bp bands observed for the LPL PvuII gene indicated P1P1 (wild type), P1P2 (hetero type), and P2P2 (mutant type) genotypes, respectively.
Assessment of nutrient intake
At the first visit, a 24-h food recall recording the type and amount of food eaten in a day was conducted through a direct interview of the subjects by an investigator. Then, 3-day dietary records were assessed with a 24-h food recall method in the subjects at home (including 2 non-consecutive weekdays and 1 day on the weekend). The nutrition examination data of 269 (165 men; 104 women) of the 548 subjects, excluding those with missing values, were analyzed using the CAN-Pro 3.0 software, a commonly used nutrient analysis software for the Korean diet (The Korean Nutrition Society, Korea) to evaluate the niacin intake. Since the total calorie intake can be a primary critical factor for the risk of disease, energy-adjusted nutrients, as used by Willett et al. (1997) to explain the correlation between niacin and diseases, were used in this study.
Statistical analyses
Data were analyzed using the SPSS statistical package (Version 14.0, Chicago, IL, USA). The frequencies within our sample estimate the probability that an individual has a particular genotype, given that they are MetSyn (or not MetSyn). Bayes’ theorem provides a means to estimate probabilities associated with the inverse relationship, i.e., the probability of becoming obese given that you have a particular genotype (Wacker et al. 2008). Mean ± SD was calculated using t-test or one-way ANOVA. Frequencies of exercise, smoking, and alcohol consumption were analyzed using χ2 test. P < 0.05 was considered statistically significant. Unconditional logistic regression models were used to calculate the crude and multivariate ORs and corresponding 95% CIs. Multivariate models were simultaneously adjusted for sex (men, women), age (<50, ≥50), BMI (<25, ≥25), energy-adjusted niacin, exercise (yes, no), smoking (smoker, ex-smoker, non-smoker), and alcohol consumption (drinker, ex-drinker, or non-drinker). In addition, the P-value for linear trend was calculated by using the median of each tertile category as a continuous variable in the logistic regression models. Correlation between LPL mass and niacin intake was evaluated by linear regression analysis.
Results
Probability of LPL PvuII genotypes with regard to the existence of MetSyn
On the basis of the Korean MetSyn criteria for diagnosis used in this study, 278 (50.7%) subjects were diagnosed with MetSyn; they comprised 205 (54.8%) men and 73 (42.0%) women. The average age of the study subjects was 49.16 ± 11.52 years. The frequency of LPL PvuII polymorphism was higher in the P2 mutant allele (0.669) than in the P1 wild allele (0.331). The frequency of the P2 mutant allele in Koreans was similar to that among Asians but higher than that in Caucasians (Chung et al. 1999; Sepetiba et al. 2007; Javorsky et al. 2006; Song et al. 1999; Kosaka et al. 2006; Narita et al. 2004; Ukkola et al. 1995).
The Bayes’ theorem requires an estimate for the overall frequency of MetSyn in the background population. Therefore, we use the estimate that one-fourth of Koreans are MetSyn based on the Korea National Health and Nutrition Examination Survey (KNHANES)-III (Ministry of Health and Welfare 2006). In Table 1, the difference in genotype frequency suggests that P1P2 and P2P2 genotypes are almost 1.5 times as likely to become MetSyn compared to the P1P1 genotype in our subject. Also, the probability in women with the P1P2 genotype is about 2.25 times higher than the P1P1 and P2P2 genotypes, whereas men with P1P2 and P2P2 genotypes are slightly higher than in those with the P1P1 genotype. In particular, post-menopausal subjects with the P1P2 genotype are about 2.7 times higher than those with the P1P1 genotype.
General characteristics of the subjects
The average values of the physical measurements and lipid-related factors are shown in Table 2. In the MetSyn group, except TC level, factors such as WC, BP, FBS level, TG level, BMI, and insulin resistance-related factors such as serum insulin and HOMA-IR were significantly higher and the HDLc level was significantly lower than those in the non-MetSyn group (P < 0.001). The results did not show any correlation of the above factors with LPL PvuII polymorphism. However, in the non-MetSyn group, subjects with the P1P1 genotype had a significantly lower TG level and BMI than those with the other genotypes. The HDLc level was significantly the lowest in the subjects with the P2P2 genotype in the MetSyn group and the highest in the subjects with the P1P1 genotype in the non-MetSyn group (P < 0.001). Further, the LDLc level was the lowest in the subjects with the P2P2 genotype in the MetSyn group; this indicated that the LPL gene was not related to the LDLc level. The average LPL mass of MetSyn patients (35.98 ± 17.38 ng/mL) was significantly lower than non-MetSyn patients (43.49 ± 17.96 ng/mL; P < 0.001). It was the lowest in the MetSyn patients with the P2P2 genotype and the highest in the non-MetSyn subjects with the P1P1 genotype.
Energy intake of the MetSyn patients was significantly higher than that of the non-MetSyn group subjects (P < 0.05), but there was no significant difference with regard to LPL PvuII polymorphism. Further, there was no any significant difference with regard to niacin intake adjusted with energy intake. However, niacin intake tended to be higher in the subjects with the P1P2 genotype than in those with P1P1 and P2P2 genotypes, regardless of the existence of MetSyn.
When frequencies of lifestyle-related factors were investigated by cross-analysis, the frequency of exercise was not found to differ according to the existence of MetSyn and LPL PvuII polymorphism. However, the frequencies of smoking (non-smoker/ex-smoker/smoker) and alcohol consumption (non-drinker/ex-drinker/drinker) were higher in the MetSyn group, especially in the subjects with P2 allele than in those with P1 allele (Table 2).
Factors affecting the risk (ORs) of MetSyn prevalence
Table 3 shows the ORs (95% CIs) for the risk of MetSyn prevalence in LPL PvuII genotypes according to tertiles of LPL mass (1st, ≤34.20; 2nd, 34.21–49.50; 3rd, ≥49.51 ng/mL). After the adjustment of sex, age, BMI, and the 3 lifestyle-related factors (exercise, smoking, and alcohol consumption), the risk of MetSyn for the 3rd tertile of LPL mass was reduced to 0.494 (95% CI, 0.323–0.758), compared to that for the 1st tertile (P trend = 0.002) in all subjects. The odds ratio for the risk of MetSyn was 0.571 (95% CI, 0.340–0.959) in the P2P2 genotypes as compared to that in the P1P1/P1P2 genotypes within the 1st tertile of LPL mass. The risk of MetSyn was decreased in the P1P1/P1P2 genotype group within the 3rd tertile of LPL mass and in the P2P2 genotype group within the 2nd and 3rd tertiles of LPL mass as compared to that in the P1P1/P1P2 genotype group within the 1st tertile. However, when an energy-adjusted niacin intake was added with adjustment factors of sex, age, BMI and the 3 lifestyle-related factors, it did not cause a significant decrease in the risk of MetSyn with an increase in LPL mass (P trend = 0.489; Table 3).
Therefore, Table 4 showed that the risk of MetSyn in the LPL PvuII genotypes was investigated according to the tertile levels of energy-adjusted niacin intake (1st, ≤14.82; 2nd, 14.83–17.80; 3rd, ≥17.81 mg/day; Table 4). After the adjustment of sex, age, BMI, and the 3 lifestyle-related factors, the risk of MetSyn within the 2nd and 3rd tertiles of energy-adjusted niacin intake was significantly reduced to 0.471 (95% CI, 0.284–0.783) and 0.464 (95% CI, 0.279–0.771), respectively, compared to that within the 1st tertile (P trend < 0.01). In particular, the risk of MetSyn in the P2P2 genotype group within the 1st tertile of niacin intake increased by about 2.2 times (95% CI, 1.157–4.351) as compared to those of P1P1 or P1P2 genotype groups, even after the adjustment of sex, age, BMI, and the 3 lifestyle-related factors. However, the risk of MetSyn was reduced to 0.256 (95% CI, 0.115–0.571) in the P2P2 genotype group for the 2nd tertile of niacin intake, compared to that in the subjects with P1P1 or P1P2 genotype groups within the 1st tertile of niacin intake. This result suggested that optimal levels of niacin intake prevented MetSyn prevalence more effectively in the LPL PvuII polymorphism.
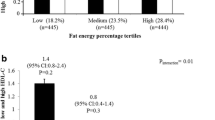
Correlation between LPL mass and energy-adjusted niacin intake was examined with LPL PvuII polymorphism with respect to gender difference. The subjects with the P1P1 genotype showed a slightly increased LPL mass with higher niacin intake, but the significance was not found (Fig. 1a). However, in the subjects with the P2P2 genotype, even more niacin intake was associated with a significant decrease in LPL mass. In particular, men with the P1P1 genotype showed a positive correlation between LPL mass level and energy-adjusted niacin intake, whereas women with the P2P2 genotype showed a significantly negative correlation (P < 0.1; Fig. 1b)

Correlation between lipoprotein lipase mass and energy-adjusted niacin intake according to lipoprotein lipase PvuII genotype (a) on gender difference (b). LPL, lipoprotein lipase; P1P1 genotype, wild type; P1P2 genotype, hetero type; P2P2 genotype, mutant type
Discussion
This study is the first to report the effects of LPL gene polymorphism, LPL mass, blood biochemical levels, niacin intake, and other factors on the risk of MetSyn prevalence in Koreans. In particular, this is the first data that suggest that the optimal levels of niacin intake reduce the risk of MetSyn prevalence.
The LPL PvuII mutant allele frequencies were recorded to be 0.672 and 0.665 for the non-MetSyn and MetSyn groups, respectively. This study is similar to those previously recorded for Japanese subjects (0.640) and Chinese subjects (0.693) (Chung et al. 1999; Shen et al. 2000; Song et al. 1999; Kosaka et al. 2006; Narita et al. 2004). However, they are higher than those recorded for Turks (0.518) and Finns (0.460) (Susleyici Duman et al. 2005; Ukkola et al. 1995). A high-frequency value was expected to cause the future occurrence of dyslipidemia in Koreans. The difference in genotype frequency suggests that those possessing the P1P2 and P2P2 genotypes are almost 1.5 times as likely to become MetSyn as those with the P1P1 genotype among our study subjects. In particular, post-menopausal women with the P1P2 genotype are about 2.7 times higher at risk than women with the P1P1 genotype.
Kastelein et al. showed that LPL mass is strongly correlated with LPL activity (r = 0.70, P < 0.0001); hence, low LPL mass can be interpreted to inhibit the rate-limiting step in the removal of TG-rich lipoproteins from the circulation, similar to LPL activity (Kastelein et al. 2000). In a previous study, the LPL mass of Japanese subjects with type 2 diabetes was significantly lower than that of normal persons (Miyashita et al. 2002). The average LPL masses for the total number of subjects, MetSyn patients, and non-MetSyn subjects were 39.64 ± 18.05 ng/mL, 35.98 ± 17.38 ng/mL, and 43.49 ± 17.96 ng/mL, respectively, which indicated that the LPL activity was significantly low in the MetSyn patients (P < 0.001); this result was the same as that of another study that measured LPL mass with regard to the existence of MetSyn (Saiki et al. 2007). The previous study found that the MetSyn group had a significantly lower LPL mass than non-MetSyn group and more MetSyn risk factors further decreased LPL mass significantly (Saiki et al. 2007). In addition, this study revealed that the P2P2 genotype was associated with a significantly low LPL mass than other genotypes (P < 0.001). Further, Watanabe et al. reported that there was no significant gender difference in LPL mass, but showed that the LPL activity in women (45.9 ± 17.3 ng/mL) was higher than that in men (35.7 ± 17.4 ng/mL) (Watanabe et al. 1999). The LPL mass in women was slightly higher than about 40 ng/mL (35 ng/mL for males), which was the optimal serum LPL mass cutoff point shown in a study wherein the receiver operator characteristic analysis was performed to predict the presence of intra-abdominal visceral fat area (≥100 cm2) (Kobayashi et al. 2007). Men with the P2P2 genotype showed a lower LPL mass (30.45 ± 15.98 ng/mL) than the optimal LPL mass cutoff point. The results of meta-analysis conducted by Wittrup et al. revealed that the S447X variant of the LPL gene is not related to LPL activity (Wittrup et al. 1999).
In previous studies on the correlation between LPL PvuII polymorphism and lipid profiles, subjects with the P2P2 genotype, e.g., patients with cerebral infarction and Turks with coronary artery disease had higher TG levels and lower HDLc levels (Xu et al. 2008; Duman et al. 2004). Our subjects with the P2P2 genotype showed a significantly low HDLc level; a high TG level was observed only in the subjects with the P2P2 genotype in the non-MetSyn group. Other studies, like those of Susleyici et al. with Turks and of Gerdes et al. with Danes, have shown no significant correlation between LPL gene polymorphism and lipid profiles (Susleyici Duman et al. 2005; Gerdes et al. 1995). Lack of LPL due to LPL PvuII polymorphism causes inhibition of lipolysis and increases chylomicron and VLDLc levels and degradation of adipocyte TG increases free fatty acid content in the blood (Merkel et al. 2002). This elevated plasma TG level induced by reduction of useful lipids in tissues can lead to MetSyn with a decrease in HDLc level. Hitsumoto et al. revealed that LPL mass was negatively correlated with TG level and positively correlated with HDL level in Japanese subjects (Hitsumoto et al. 2000); this is the same as that of our study (data not shown). Other research that examined the correlation between intra-abdominal visceral fat and preheparin LPL mass in hyperlipidemia Japanese patients and normal persons reported that LPL mass is negatively correlated with intra-abdominal visceral fat (Kobayashi et al. 2007).
This study also investigated the correlation between LPL mass and energy-adjusted nutrients and showed that LPL mass in the P1P1 and P1P2 genotype groups was positively correlated with intakes of animal lipids and different types of fatty acids, while that in the P2P2 genotype was negatively correlated with intakes of total proteins, animal proteins, niacin, cholesterol, and polyunsaturated fatty acids (data not shown). Since niacin decreases the levels of lipoproteins such as LDLc and VLDLc, including phospholipids and apolipoprotein B, and increases those of apo AI and HDLc significantly, these are powerful predictors of the risk of coronary heart disease (National Coordinating Committee on Food and Nutrition (NCCN) 2005; McKenney 2004). National Cholesterol Education Program reported that immediate-release (IR) niacin increased the HDLc level by 15%–35% and reduced the LDLc and TG levels by 5–25 and 20–50%, respectively (National Cholesterol Education Program 2001). In addition, niacin intake of <2,000 mg/day produces nearly maximal HDLc levels (National Coordinating Committee on Food and Nutrition (NCCN) 2005). But niacin intake of ≥2,000 mg has been reported to cause side effects, such as flushing following vasodilatation, nausea, vomiting, hepatic toxicity, and glucose intolerance (McKenney 2003; Al-Shaer and AbuSabha 2004; National Coordinating Committee on Food and Nutrition (NCCN) 2005). The 2005 Korea national survey on public health and nutrition revealed that the average niacin intake of Korean adults aged >20 years was 15.4 mg/day (men, 17.1 mg/day; women, 13.7 mg/day; Korea Center for Disease Control and Prevention 2007). Sets of Dietary Reference Intakes for Koreans (KDRIs) indicated the recommended intakes (RIs) of niacin as 16 and 14 mg/day for men and women, respectively, aged >20 years (Korean Nutrition Society 2005), which is the same as RI levels recommended by the Food and Agriculture Organization (FAO)/WHO (2004), and the United States Institute of Medicine (IOM 1998) (National Coordinating Committee on Food and Nutrition (NCCN) 2005). Our female subjects with the P2P2 genotype showed a significantly negative correlation between LPL mass and energy-adjusted niacin intake. In particular, the energy-adjusted niacin intake of >14.82 mg/day significantly reduced the risk of MetSyn. The MetSyn risk in the subjects with P2P2 genotype was 2.4 times higher than that in the subjects with P1 allele when they had niacin intake lower than 14.82 mg/day. The subjects with the P2P2 genotype showed a decreased risk of MetSyn at the optimal niacin intake (14.83–17.80 mg/day) as compared to those with high intake of niacin (>17.81 mg/day) but still decreased their MetSyn risk compared to those with low intake of niacin (<14.83). The result suggests that higher niacin intake than the RI level may be protective against MetSyn, especially with regard to the P2P2 genotype group. Although an increase in LPL mass was associated with a decrease in MetSyn prevalence, there was no significant decrease in MetSyn prevalence when energy-adjusted niacin intake was considered. However, since most niacin trials used daily doses of ≤2 g to treat CVD or lipid disorders, it was difficult to compare their results with niacin intake from the usual diet and its effect on the risk of MetSyn, as shown in this study (McKenney 2004).
Niacin inhibits elimination of HDL apoAI by blocking the putative hepatocyte HDL catabolism receptors. Since niacin intake decreases HDL apoAI catabolism, it increases HDL half-life and concentration of Lp-AI HDL subfraction, leading to increased cholesterol efflux and reverse cholesterol transport (Kamanna and Kashyap 2008). However, we found that MetSyn patients with the P2P2 genotype did not show increased LPL mass even after more niacin intake. The result suggested that niacin intake was more effective in prevention than in treatment of MetSyn.
We concluded that (1) LPL PvuII polymorphism was associated with a high TG level, low LPL mass, and low HDLc level, (2) high LPL mass decreased the risk of MetSyn prevalence, (3) niacin intake in the usual diet reduced the risk of MetSyn even in subjects with LPL PvuII polymorphism. Otherwise, more niacin intake could not increase LPL mass in subjects with the P2P2 genotype. This study was not a randomized clinical intervention design for niacin in MetSyn according to LPL PvuII polymorphism but our data showed that the low niacin intake (<14.81 mg/day) increased the prevalence of MetSyn. We suggested that our results, based on the modified Korean MetSyn criteria, might be one explanation as to why personal differences regarding the risk of MetSyn prevalence could exist. Moreover, different optimal level of niacin intake for the prevention of MetSyn might be considered in different genotype of LPL PvuII.
References
Ahn YI, Kamboh MI, Hamman RF, Cole SA, Ferrell RE (1993) Two DNA polymorphisms in the lipoprotein lipase gene and their associations with factors related cardiovascular disease. J Lipid Res 34:421–428
Al-Shaer MH, AbuSabha HS (2004) Are the effects of nicotinic acid on insulin resistance precipitated by abnormal phosphorous metabolism? Lipids Health Dis 3:23
Botstein D, White RL, Skolnick M, Davis RW (1980) Construction of a genetic linkage map in man using restriction fragment length polymorphisms. Am J Hum Genet 32:314–331
Canner PL, Furberg CD, McGovern ME (2006) Benefits of niacin in patients with versus without the metabolic syndrome and healed myocardial infarction (from the Coronary Drug Project). Am J Cardiol 97:477–479
Chamberlain JC, Thorn JA, Oka K, Galton DJ, Stocks J (1989) DNA polymorphisms at the lipoprotein lipase gene: Associations in normal and hypertriglyceridaemic subjects. Atherosclerosis 79:85–91
Chapman MJ, Redfern JS, McGovern ME, Giral P (2010) Niacin and fibrates in atherogenic dyslipidemia: pharmacotherapy to reduce cardiovascular risk. Pharmacol Ther 126:314–345
Chung HJ, Yoon YM, Han TH, Park H, Song J, Kim JQ (1999) Polymorphisms at the lipoprotein lipase gene: possible associations with coronary artery disease and blood lipid levels in Koreans. Korean J Clin Pathol 19:617–623
Duman BS, Turkoqlu C, Akpinar B, Guden M, Vertii A, Dak E, Cagatay P, Gunay D, Buyukdevrim AS (2004) Lipoprotein lipase gene polymorphism and lipid profile in coronary artery disease. Arch Pathol Lab Med 128:869–874
Ekelund U, Anderssen S, Andersen LB, Riddoch CJ, Sardinha LB, Luan J, Froberg K, Brage S (2009) Prevalence and correlates of the metabolic syndrome in a population-based sample of European youth. Am J Clin Nutr 89:90–96
Fisher KL, FitzGerald GA, Lawn RM (1987) Two polymorphisms in the human lipoprotein lipase (LPL) gene. Nucleic Acids Res 15:7657
Food and Nutrition Board, Insitute of Medicine (IOM) (1998) Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin and choline. The National Academies Press, Washington, DC, pp 123–149
Friedewald VE Jr, Gotto AM Jr (2000) Case 1: a patient with elevated low-density lipoprotein cholesterol. Am J Cardiol 85:131
Gerdes C, Gerdes LU, Hansen PS, Faergeman O (1995) Polymorphisms in the lipoprotein lipase gene and their associations with plasma lipid concentrations in 40-year-old Danish men. Circulation 92:1765–1769
Gotoda T, Senda M, Murase T, Yamada N, Takaku F, Furuichi Y (1989) Gene polymorphism identified by PvuII in familial lipoprotein lipase deficiency. Biochem Biophys Res Commun 164:1391–1396
Haung TT, Ball GD, Franks PW (2007) Metabolic syndrome in youth: current issues and challenges. Appl Physiol Nutr Metab 32:13–22
Hitsumoto T, Ohsawa H, Uchi T, Noike H, Kanai M, Yoshinuma M, Miyashita Y, Watanabe H, Shirai K (2000) Preheparin serum lipoprotein lipase mass is negatively related to coronary atherosclerosis. Atherosclerosis 153:391–396
Javorsky M, Kozarova M, Salagovic J, Tkac I (2006) Relationship among urinary albumin excretion rate, lipoprotein lipase PvuII polymorphism and plasma fibrinogen in type 2 diabetic patients. Physiol Res 55:55–62
Kamanna VS, Kashyap ML (2008) Mechanism of action of niacin. Am J Cardiol 101:20–26
Kastelein JJ, Jukema JW, Zwinderman AH, Clee S, van Boven AJ, Jansen H, Rabelink TJ, Pters RJ, Lie KI, Liu G, Bruschke AV, Havden MR (2000) Lipoprotein lipase activity is associated with severity of angina pectoris. REGRESS Study Group. Circulation 102:1629–1633
Kobayashi J, Hashimoto H, Fukamachi I, Tashiro J, Shirai K, Saito Y, Yoshida S (1993) Lipoprotein lipase mass and activity in severe hypertriglyceridemia. Clin Chim Acta 216:113–123
Kobayashi J, Nohara A, Kawashiri MA, Inazu A, Koizumi J, Nakajima K, Mabuchi H (2007) Serum lipoprotein lipase mass: clinical significance of its measurement. Clin Chim Acta 378:7–12
Korea Center for Disease Control and Prevention (2007) In-depth analysis on the 3rd (2005) Korea health and nutrition examination survey—nutrition survey. Korea Health Industry Development Institute, Seoul, pp 1–452
Korean Nutrition Society (2005) Dietary reference intakes for Koreans. Kookjin Publishing Co, Seoul
Kosaka T, Yoshino J, Inui K, Wakabayashi T, Okushima K, Kobayashi T, Miyoshi H, Nakamura Y, Hayashi S, Shiraishi T, Watanabe M, Yamamoto T, Nakahara A, Katoh T (2006) Impact of lipoprotein lipase gene polymorphisms on ulcerative colitis. World J Gastroenterol 12:6325–6330
Levesque J, Lamarche B (2008) The metabolic syndrome: definitions, prevalence and management. J Nutrigenet Nutrigenomics 1:100–108
Lottenberg SA, Glezer A, Turatti LA (2007) Metabolic syndrome: identifying the risk factors. J Pediatr (Rio J) 83:204–208
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and β-cell function form fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
McKenney J (2003) Niacin for dyslipidemia: considerations in product selection. Am J Health Syst Pharm 60:995–1005
McKenney J (2004) New perspectives on the use of niacin in the treatment of lipid disorders. Arch Intern Med 164:697–705
Merkel M, Eckel RH, Goldberg IJ (2002) Lipoprotein lipase: genetics, lipid uptake, and regulation. J Lipid Res 43(12):1997–2006
Ministry of Health and Welfare (2006) The Third Korea National Health and Nutrition Examination Survey (KNHANES III), 2005 health examination. Ministry of Health and Welfare, Seoul
Miyashita Y, Shirai K, Itoh Y, Sasaki H, Totsuka M, Murano T, Watanabe H (2002) Low lipoprotein lipase mass in preheparin serum of type 2 diabetes mellitus patients and its recovery with insulin therapy. Diabetes Res Clin Pract 56:181–187
Motta M, Bennati E, Cardillo E, Passamonte M, Ferlito L, Malaguarnera M (2009) The metabolic syndrome (MS) in the elderly: considerations on the diagnostic criteria of the International Diabetes Federation (IDF) and some proposed modifications. Arch Gerontol Geriatr 48:380–384
Narita S, Tsuchiya N, Wang L, Matsuura S, Ohyama C, Satoh S, Sato K, Ogawa O, Habuchi T, Kato T (2004) Association of lipoprotein lipase gene polymorphism with risk of prostate cancer in a Japanese population. Int J Cancer 112:872–876
National Cholesterol Education Program (2001) The third report of the expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication no. 01-3095. National Heart, Lung, and Blood Institute, Bethesda
National Coordinating Committee on Food and Nutrition (NCCN) (2005) Ministry of health Malaysia, Putrajaya, chap. 8: niacin (Vitamin B3), pp 81–89
Pan WH, Yeh WT, Weng LC (2008) Epidemiology of metabolic syndrome in Asia. Asia Pac J Clin Nutr 17:37–42
Park JS, Sung JD, Chae IH, Kim HS, Ju JR, Son DW, Oh BH, Lee MM, Park YB, Choi YS, Lee YW (2000) Effect of lipoprotein lipase gene polymorphism on lipid profile and body mass index in healthy Korean adult. Korean J Med 58:57–66
Rosenson RS (2009) Management of non-high-density lipoprotein abnormalities. Atherosclerosis 207:328–335
Saiki A, Oyama T, Endo K, Ebisuno M, Ohira M, Koide N, Murano T, Miyashita Y, Shirai K (2007) Preheparin serum lipoprotein lipase mass might be a biomarker of metabolic syndrome. Diabetes Res Clin Pract 76:93–101
Sakayama K, Masuno H, Kidani T, Matsuda Y, Yamamoto H, Okuda H (2001) Synthesis of active high mannose-type lipoprotein lipase in human adipose tissues. Atherosclerosis 155:29–35
Sepetiba RJ, Andrade J, Hirata RD, Hirata MH, Sepetiba CR, Nakamura Y, Matsumoto LO, Cavalli SA, Bertolami MC (2007) Lipoprotein lipase PvuII polymorphism is associated with variations in serum lipid levels in non-diabetic pregnant women. Braz J Med Biol Res 40:919–926
Shen H, Yu S, Xu Y, Yu R, Jiang W, Chen W (2000) DNA polymorphism of PvuII site in the lipoprotein lipase gene in patients with type 2 diabetes mellitus. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 17:24–27
Song HJ, Kim JM, Kim J (1999) Association of lipoprotein lipase gene polymorphisms with plasma lipids in ischemic stroke patients. J Korean Neurol Assoc 17:340–346
Susleyici Duman B, Ozturk M, Yilmazer S, Cagatay P, Hatemi H (2005) DNA polymorphism of PvuII site in the lipoprotein lipase gene in patients with non-insulin dependent diabetes mellitus. Cell Biochem Funct 23:399–404
Tan CE, Ma S, Wai D, Chew SK, Tai ES (2004) Can we apply the National Cholesterol Education Program Adult Treatment Panel definition of the metabolic syndrome to Asians? Diabetes Care 27:1182–1186
Ukkola O, Savolainen MJ, Salmela PI, von Dickhoff K, Kesaniemi YA (1995) DNA polymorphisms at the lipoprotein lipase gene are associated with macroangiopathy in type 2 (non-insulin-dependent) diabetes mellitus. Atherosclerosis 115:99–105
Ukkola O, Garenc C, Perusse L, Bergeron J, Despres JP, Rao DC, Bouchard C (2001) Genetic variation at the lipoprotein lipase locus and plasma lipoprotein and insulin levels in the Quebec Family Study. Atherosclerosis 158:199–206
Vittone F, Chait A, Morse JS, Fish B, Brown BG, Zhao XQ (2007) Niacin plus simvastatin reduces coronary stenosis progression among patients with metabolic syndrome despite a modest increase in insulin resistance: a subgroup analysis of the HDL-Atherosclerosis Treatment Study (HATS). J Clin Lipidol 1:203–210
Wacker MJ, Godard MP, McCabe EH, Donnelly JE, Kelly JK (2008) Sex difference in the association of the angiotensin converting enzyme I/D polymorphism and body mass index. Med Sci Monit 14:353–357
Watanabe H, Miyashita Y, Murano T, Hiroh Y, Itoh Y, Shirai K (1999) Preheparin serum lipoprotein lipase mass level: the effects of age, gender, and types of hyperlipidemias. Atherosclerosis 145:45–50
Willett WC, Howe GR, Kushi LH (1997) Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr 65:1220–1228
Wittrup HH, Tybjaerj-Hansen A, Nordestgaard BG (1999) Lipoprotein lipase mutations, plasma lipids and lipoproteins, and risk of ischemic heart disease. A meta-analysis. Circulation 99:2901–2907
World Health Organization and Food and Agriculture Organization of the United Nations (2004) Vitamin and mineral requirements in human nutrition. 2nd edn. World Health Organization, Geneva, pp 173–175
Xu E, Li W, Zhan L, Guan G, Wang X, Chen S, Shi Y (2008) Polymorphisms of the lipoprotein lipase gene are associated with atherosclerotic cerebral infarction in the Chinese. Neuroscience 155:403–408
Acknowledgments
We appreciate the help of all the staff members at the Seoul Medical Center and Severance Hospital, Yonsei University, in the screening and/or recruitment of the patients. This study was funded by the Korean Seoul City Research and Business Development program (10526), Ministry of Health and Welfare (A000385) and Korea Food and Drug Administration (11162KFDA154), Republic of Korea.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Shin, E., Park, NY., Jang, Y. et al. The association of lipoprotein lipase PvuII polymorphism and niacin intake in the prevalence of metabolic syndrome: a KMSRI-Seoul study. Genes Nutr 7, 331–341 (2012). https://doi.org/10.1007/s12263-011-0251-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12263-011-0251-9