
Abstract
Objectives
Chronic kidney disease (CKD) is a major public health problem. Epidemiological studies of the relationship between alcohol intake and CKD are scarce in Japan. This cross-sectional study aims to investigate the relationship between frequency of drinking alcohol and CKD in Japanese men.
Methods
The subjects were 9,196 men (mean ± standard deviation age, 57.9 ± 5.1 years) who underwent a health check-up. CKD was defined as estimated glomerular filtration rate <60 mL/min/1.73 m2. Frequency of alcohol drinking was obtained from questionnaire and divided into five categories: nondrinkers, once or twice a week, three or four times a week, five or six times a week, and everyday drinkers.
Results
Multivariable-adjusted [age, body mass index, hypertension, diabetes, hyper-low-density lipoprotein (LDL) cholesterolemia, smoking, and physical activity] odds ratios and 95% confidence intervals (CIs) were calculated using logistic regression analysis. Compared with the results for the nondrinkers, the multivariable-adjusted odds ratios of CKD were as follows: 0.76 (95% CI 0.60–0.95) for 1–2 drinks per week, 0.74 (95% CI 0.59–0.93) for 3–4 drinks per week, 0.79 (95% CI 0.64–0.97) for 5–6 drinks per week, and 0.60 (95% CI 0.51–0.71) for everyday drinkers. There was a significant inverse trend across increasing frequency of drinking alcohol (p = 0.001 for trend).
Conclusions
An inverse association was found between frequency of drinking alcohol and CKD in apparently healthy men.
Similar content being viewed by others

Introduction
In 2002, the Kidney Disease Outcome Quality Initiative (KDOQI) from the National Kidney Foundation (NKF) developed guidelines for detection and evaluation of chronic kidney disease (CKD) according to glomerular filtration rate (GFR) and micro/macroalbuminuria [1]. Go et al. [2] clearly showed an independent, graded association between low GFR values and high risk of death and cardiovascular events in a large community-based population. CKD is an independent risk factor for cardiovascular disease events [3–6] and all-case deaths [5–7] in the general Japanese population, suggesting that CKD represents a major public health problem. It is therefore important to identify the lifestyle risk factors associated with incidence of CKD for determining appropriate prevention methods for this disease. Smoking is a well-recognized risk factor for CKD [8–12]. However, epidemiological studies of the relationship between alcohol consumption and CKD are scarce. A few studies have indicated that moderate alcohol consumption was not associated with increased risk of renal dysfunction [13] and was associated with only a low risk of cardiovascular mortality in CKD patients [14], whereas other studies showed that heavy drinking was associated with a high risk of CKD [12] and end-stage renal disease (ESRD) [15]. In addition, a few previous studies [9, 16] showed that alcohol consumption was not associated with CKD. Thus, the relationship between alcohol intake and CKD remains unclear. The aim of the present cross-sectional study is to investigate the relationship between frequency of drinking alcohol and CKD in Japanese men.
Methods
Study population
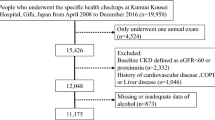
The participants were health examinees who visited the Japanese Red Cross Kumamoto Health Care Center for a multiphasic health check-up from April 2008 to March 2009. The participants consisted of workers and residents of a rural area of Kumamoto, Japan. In Japan, employees generally undergo annual check-ups at their workplace or at designated clinics. The health check-up programs involve physical examination, laboratory data collection, and interview questionnaires. Data on medical history and lifestyle information were collected by means of interview questionnaires conducted by a public health nurse. A physician examined all of the participants. Of the 18,539 men who were initially enrolled as participants, 9,826 (aged 50–69 years) were included. The following exclusion criteria were applied: (1) history of physician-diagnosed CKD, and (2) missing data on lifestyle assessments, body measurements, or laboratory tests. Of the 9,826 men, 38 (0.4%) had history of physician-diagnosed CKD and 592 (6%) had missing data, being excluded from the analysis. Finally, we analyzed 9,196 men in this study. Our research protocol was approved by the Human Ethics Committee of Kumamoto University. Informed consent was obtained from all subjects in oral format prior to the health check-up.
Physical examination
The patients were placed in sitting position and rested for 5 min. Thereafter, trained nurses measured systolic blood pressure (SBP) and diastolic blood pressure (DBP) using an automatic digital sphygmomanometer (HEM-904; OMRON, Japan) placed on the upper arm at the level of the heart. The average of 2 measurements was used for the present analysis. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters.
Laboratory data
After an overnight fast, blood samples were obtained for measurement of serum levels of routine medical check-up markers: low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), fasting glucose, and C-reactive protein (CRP). CRP levels were measured using a high-sensitivity latex assay. Serum creatinine concentrations were obtained using the enzymatic method (Detaminar L-CRE; Kyowa Medics, Japan).
Questionnaires
Lifestyle information such as smoking history, alcohol intake, and physical activity was obtained through an interview questionnaire [17]. A detailed smoking history was used to define individuals as “never smokers” (those who denied past and current smoking), “former smokers” (those who reported smoking before the examination but denied current smoking at examination), or “current smokers” (those who reported smoking at least one cigarette per day). The frequency of alcohol drinking was divided into five categories: “nondrinkers,” “once or twice a week,” “three or four times a week,” “five or six times a week,” and “everyday drinkers.” Physical activity was divided into 2 categories: “regular physical activity” defined as physical activity performed regularly, at least twice per week for at least 30 min per session throughout the year; and “physical inactivity” defined as engaging in irregular physical activity or engaging in no form of physical activity at all.
Definition of chronic kidney disease
Estimated GFR was calculated using the equation of Matsuo et al. [18]. This equation, originating from the Modification of Diet in Renal Disease (MDRD) Study group [19], is designed for Japanese individuals and is recommended by the Japanese Society of Nephrology: estimated GFR (mL/min/1.73 m2) = 194 × Scr−1.094 × age−0.287. CKD was defined as estimated GFR <60 mL/min/1.73 m2 [3, 4].
Other variables
Hypertension was defined as SBP of 140 mm Hg or higher and/or DBP of 90 mmHg or higher or as current or previous use of antihypertensive medication according to Japanese Society of Hypertension guidelines [20].
Hyper-LDL-cholesterolemia was defined as serum LDL-cholesterol level ≥140 mg/dl (3.6 mmol/l) or as treatment with a statin, according to 2007 Japanese Atherosclerosis Society guidelines [21].
Diabetes was defined as fasting blood glucose level ≥126 mg/dl or as treatment with insulin or oral hypoglycemic agents, according to the report of the Committee of Japan Diabetes Society on the classification and diagnostic criteria of diabetes mellitus [22].
Statistical analysis
Results are presented as mean ± standard deviation (SD), and categorical variables are expressed as frequencies. Characteristics of the subjects according to presence of CKD were compared using Student’s t and Mann–Whitney U tests for continuous and categorical variables, respectively. Analysis of variance (ANOVA) with post hoc Tukey’s test and Kruskal–Wallis test with post hoc Bonferroni adjustment were used to assess differences in characteristics by frequency of drinking alcohol. The relationship between CKD and frequency of drinking alcohol was analyzed using a logistic regression model. Trend tests were performed to evaluate the impact of frequency of drinking alcohol on the odds ratios (OR). All analyses were performed using IBM SPSS Statistics 18 software.
Results
The characteristics of the subjects according to presence of CKD are presented in Table 1. The subjects were 9,196 men (mean age 57.9 ± 5.1 years). The prevalence of CKD was 11.5% in this study, similar to the results of a previous nationwide epidemiological study that found that CKD was present in 12.0% of Japanese subjects aged 60–69 years [23]. Significant differences between the 2 groups were seen in relation to age, estimated GFR, creatinine, BMI, CRP, HDL-C, prevalence of hyper-LDL-cholesterolemia and hypertension, frequency of treatment for cholesterolemia and hypertension, smoking history, frequency of drinking alcohol, and physical activity.
Table 2 presents the characteristics of the subjects according to frequency of drinking alcohol. Significant differences in frequency of drinking alcohol were seen in relation to age, estimated GFR, creatinine, BMI, HDL-C, prevalence of CKD, hyper-LDL-cholesterolemia and hypertension, frequency of treatment for cholesterolemia, hypertension, and diabetes, smoking history, and physical activity.
Table 3 presents the relationship between CKD and frequency of drinking alcohol. Compared with the results for the nondrinkers, the multivariable-adjusted ORs of CKD were as follows: 0.76 (95% CI 0.60–0.95) for 1–2 drinks per week, 0.74 (95% CI 0.59–0.93) for 3–4 drinks per week, 0.79 (95% CI 0.64–0.97) for 5–6 drinks per week, and 0.60 (95% CI 0.51–0.71) for everyday drinkers. There was a significant inverse trend across increasing frequency of drinking alcohol (p = 0.001 for trend).
Discussion
In 2009, the Japanese Society of Nephrology established an equation for estimating GFR from serum creatinine and age for the Japanese general population [18]. Imai et al. [23] suggested that prevalence of CKD may be overestimated when using the MDRD equation multiplied by a coefficient of 0.881 for the Japanese population. To our knowledge, this is the first study to investigate the relationship between frequency of drinking alcohol and CKD using the new Japanese equation for estimated GFR. The results of this study suggest an inverse association between frequency of drinking alcohol and CKD, as indicated by logistic regression analysis after adjusting for age, BMI, hypertension, diabetes, hyper-LDL-cholesterolemia, smoking, and physical activity. This inverse relationship between frequency of drinking alcohol and CKD is similar to that in a study by Shaffner et al. [13], who conducted a 14-year prospective cohort study of 11,023 initially healthy men. Compared with men who consumed no more than 1 drink per week, men who consumed 2–4 drinks weekly had a multivariable-adjusted OR of 1.04 (95% CI 0.80–1.32) for serum creatinine elevation (>133 μmol/L), men who consumed 5–6 drinks per week had an OR of 0.92 (95% CI 0.68–1.25), and men who consumed at least 7 drinks weekly had an OR of 0.71 (95% CI 0.55–0.92) (p = 0.01 for the trend across categories). CKD is associated with a high prevalence of hypertension, diabetes, and hypercholesterolemia [7, 11]. The National High Blood Pressure Education Program of the National Heart, Lung, and Blood Institute recommended that alcohol consumption should be limited to no more than 1 oz (30 ml) of ethanol (2 drinks) per day in men for the prevention and treatment of hypertension [24]. In this study, subjects who drank every day had significantly higher prevalence of hypertension than nondrinkers. However, this group had lower prevalence of CKD and hyper-LDL-cholesterolemia, had higher HDL-C levels, and did not show higher prevalence of diabetes compared with nondrinkers. This result was also similar to those from a study by Shaffner et al. [13], who reported that subjects who consumed 7 or more alcoholic drinks per week had the highest HDL-C levels and decreased risk of renal dysfunction. Although the mechanism is not fully understood, the protective effect of alcohol against CKD may be mediated by increased HDL-C [25, 26], reduced insulin secretion [27], a possible reduction in the risk of type 2 diabetes mellitus [28], and preventive effects on the development of arteriosclerosis in patients with type 2 diabetes mellitus [29].
We could not find any potential harmful effects regarding the frequency of drinking alcohol on CKD. A case–control study of 716 patients with incident ESRD and 361 age-matched population controls conducted by Perneger et al. [15] showed the presence of a significantly increased risk of ESRD among individuals who consumed more than 2 drinks per day as compared with those who abstained from alcohol (OR: 4.0; 95% CI, 1.2–13.0). In addition, Shankar et al. [12] examined the association between CKD and heavy alcohol consumption in a 5-year longitudinal analysis of 3,392 Americans without CKD. They found that heavy alcohol consumption, defined as 4 or more servings of alcohol per day, was associated with an increased risk of CKD (OR 1.99; 95% CI 0.99–4.01). However, the subjects among these 2 studies and ours differed; their studies either used subjects who were preexisting ESRD patients [15] or combined data for both men and women [12], whereas our study examined apparently healthy men.
The current study has some limitations. First, the subjects of this study do not represent the general population because of age, gender, and health status limitations. Second, we assessed only men because of the small number of women who drink alcohol. Moreover, the interval between onset of drinking-related problems and entry into treatment appears to be shorter for women than for men [30]. Alcohol also affects women differently than men, since women metabolize alcohol more slowly [31]. Tolstrup et al. [32] reported an inverse association between frequency of drinking alcohol and risk of coronary heart disease in men; however, this relationship was not seen in women. Further studies into the sex differences in the association between alcohol consumption and CKD are required. Third, nondrinkers presumably include exdrinkers. Fourth, we did not assess association between amount of alcohol and CKD. Heavy alcohol drinking is positively associated with many problems such as cancers [33], and overall mortality [34] is higher among individuals with high alcohol intake compared with light consumers. Another study will be needed to assess heavy alcohol drinking and CKD. Fifth, our results are based on a cross-sectional analysis. However, it is unlikely that the estimated GFR would influence alcohol consumption, as people with history of physician-diagnosed CKD were excluded. A large-scale prospective study will be needed to reveal the long-term effects of alcohol consumption on CKD.
In conclusion, an inverse association was found between frequency of drinking alcohol and CKD in apparently healthy men.
References
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39:S1–226.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305.
Ninomiya T, Kiyohara Y, Kubo M, Tanizaki Y, Doi Y, Okubo K, et al. Chronic kidney disease and cardiovascular disease in a general Japanese population: the Hisayama Study. Kidney Int. 2005;68:228–36.
Kokubo Y, Nakamura S, Okamura T, Yoshimasa Y, Makino H, Watanabe M, et al. Relationship between blood pressure category and incidence of stroke and myocardial infarction in an urban Japanese population with and without chronic kidney disease: the Suita Study. Stroke. 2009;40:2674–9.
Irie F, Iso H, Sairenchi T, Fukasawa N, Yamagishi K, Ikehara S, et al. The relationships of proteinuria, serum creatinine, glomerular filtration rate with cardiovascular disease mortality in Japanese general population. Kidney Int. 2006;69:1264–71.
Nakayama M, Metoki H, Terawaki H, Ohkubo T, Kikuya M, Sato T, et al. Kidney dysfunction as a risk factor for first symptomatic stroke events in a general Japanese population—the Ohasama study. Nephrol Dial Transplant. 2007;22:1910–5.
Nakamura K, Okamura T, Hayakawa T, Kadowaki T, Kita Y, Ohnishi H, et al. NIPPON DATA 90 Research Group. Chronic kidney disease is a risk factor for cardiovascular death in a community-based population in Japan: NIPPON DATA 90. Circ J. 2006;70:954–9.
Jones-Burton C, Seliger SL, Scherer RW, Mishra SI, Vessal G, Brown J, et al. Cigarette smoking and incident chronic kidney disease: a systematic review. Am J Nephrol. 2007;27:342–51.
Stengel B, Tarver-Carr ME, Powe NR, Eberhardt MS, Brancati FL. Lifestyle factors, obesity and the risk of chronic kidney disease. Epidemiology. 2003;14:479–87.
Hallan S, de Mutsert R, Carlsen S, Dekker FW, Aasarød K, Holmen J. Obesity, smoking, and physical inactivity as risk factors for CKD: are men more vulnerable? Am J Kidney Dis. 2006;47:396–405.
Yamagata K, Ishida K, Sairenchi T, Takahashi H, Ohba S, Shiigai T, et al. Risk factors for chronic kidney disease in a community-based population: a 10-year follow-up study. Kidney Int. 2007;71:159–66.
Shankar A, Klein R, Klein BE. The association among smoking, heavy drinking, and chronic kidney disease. Am J Epidemiol. 2006;164:263–71.
Schaeffner ES, Kurth T, de Jong PE, Glynn RJ, Buring JE, Gaziano JM. Alcohol consumption and the risk of renal dysfunction in apparently health men. Arch Intern Med. 2005;165:1048–53.
Shlipak MG, Fried LF, Cushman M, Manolio TA, Peterson D, Stehman-Breen C, et al. Cardiovascular mortality risk in chronic kidney disease: comparison of traditional and novel risk factors. JAMA. 2005;293:1737–45.
Perneger TV, Whelton PK, Puddey IB, Klag MJ. Risk of end-stage renal disease associated with alcohol consumption. Am J Epidemiol. 1999;150:1275–81.
Vupputuri S, Sandler DP. Lifestyle risk factors and chronic kidney disease. Ann Epidemiol. 2003;13:712–20.
Funakoshi Y, Omori H, Mihara S, Marubayashi T, Katoh T. Airflow obstruction and the metabolic syndrome or its components in Japanese men. Intern Med. 2010;49:2093–9.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003;41:1–12.
Ogihara T, Kikuchi K, Matsuoka H, Fujita Higaki J, Horiuchi M, Imai Y, et al. The Japanese Society of Hypertension Guidelines for the management of hypertension (JSH 2009). Hypertens Res. 2009;32:3–107.
Japan Atherosclerosis Society. Japan Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases. J Atheroscler Thromb. 2007;5–57 (In Japanese).
Kuzuya T, Nakagawa S, Satoh J, Kanazawa Y, Iwamoto Y, Kobayashi M, et al. Report of the Committee on the classification and diagnostic criteria of diabetes mellitus. Diabetes Res Clin Pract. 2002;55:65–85.
Imai E, Horio M, Watanabe T, Iseki K, Yamagata K, Hara S, et al. Prevalence of chronic kidney disease in the Japanese general population. Clin Exp Nephrol. 2009;13:621–30.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint national Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–12.
Gaziano JM, Buring JE, Breslow JL, Goldhaber SZ, Rosner B, VanDenburgh M, et al. Moderate alcohol intake, increased levels of high-density lipoprotein and its subfraction, and decreased risk of myocardial infarction. N Engl J Med. 1993;329:1829–34.
Ridker PM, Vaughan DE, Stampfer MJ, Glynn RJ, Hennekens CH. Association of moderate alcohol consumption and plasma concentration of endogenous tissue-type plasminogen activator. JAMA. 1994;272:929–33.
Crandall JP, Polsky S, Howard AA, Perreault L, Bray GA, Barrett-Connor E, et al. Diabetes Prevention Program Research Group. Alcohol consumption and diabetes risk in the Diabetes Prevention Program. Am J Clin Nutr. 2009;90:595–601.
Ajani UA, Hennekens CH, Spelsberg A, Manson JE. Alcohol consumption and risk of type 2 diabetes mellitus among US male physicians. Arch Intern Med. 2000;160:1025–30.
Wakabayashi I, Kobaba-Wakabayashi R, Masuda H. Relation of drinking alcohol to atherosclerotic risk in type 2 diabetes. Diabetes Care. 2002;25:1223–8.
Hasin DS, Grant BF, Weinflash J. Male/female difference in alcohol-related problems: alcohol rehabilitation patients. Int J Addict. 1988;23:437–48.
Frezza M, di Padova C, Pozzato G, Terpin M, Baraona E, Lieber CS. High blood alcohol levels in women. The role of decrease gastric alcohol dehydrogenase activity and first-pass metabolism. N Engl J Med. 1990;322:95–9.
Tolstrup J, Jensen MK, Tjønneland A, Overvad K, Mukamal HJ, Grønbaek M. Prospective study of alcohol drinking patterns and coronary heart disease in women and men. BMJ. 2006;332:1244–8.
Inoue M, Wakai K, Nagata C, Mizoue T, Tanaka K, Tsuji I, et al. Research Group for the development and evaluation of cancer prevention strategies in Japan. Jpn J Clin Oncol. 2007;37:692–700.
Marugame T, Yamamoto S, Yoshimi I, Sobue T, Inoue M, Tsugane S, Japan Public Health Center-based Prospective Study Group. Patterns of alcohol drinking and all-cause mortality: results from a large-scale population-based cohort study in Japan. Am J Epidemiol. 2007;165:1039–46.
Acknowledgments
The authors would like to thank Ms. Yoko Wakaki and Mr. Hiroyuki Higashi for their excellent technical assistance.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Funakoshi, Y., Omori, H., Onoue, A. et al. Association between frequency of drinking alcohol and chronic kidney disease in men. Environ Health Prev Med 17, 199–204 (2012). https://doi.org/10.1007/s12199-011-0238-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12199-011-0238-6