
Abstract
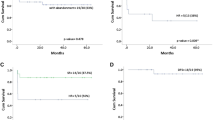
There are very limited reports about childhood acute promyelocytic leukemia (APL), especially about arsenic trioxide (ATO) treatment in both induction and post-remission regimens. 35 newly diagnosed APL patients received ATO treatment in our center and the clinical course as well as the outcome of them was investigated. The dose of intravenous ATO was 0.15–0.17 mg/kg per day, only one patient got 0.33 mg/kg per day, maximum dose was 10 mg per day in induction therapy with minimal chemotherapy treatment (CT) for hyperleukocytosis. Anthracycline or anthracycline-based CT was used for consolidation therapy and followed by 0.10–0.15 mg/kg per day ATO treatment in maintenance therapy. The continuous detection for morphology of bone marrow and PML-RARa were necessary for administrating CT or not. 3 patients died during induction therapy for intracranial hemorrhage, leukocytosis and septic shock. Total of 30 patients achieved complete remission (CR) and were followed-up for 10–108 months. The overall survival (OS) for all patients was 82.7%, whereas the OS for patients obtained CR was 95.8%. The event-free survival for 5 years was 80.3%. Disseminated intravascular coagulation could be under control to reduce induction mortality with adequate supportive care, especially in the first 2 weeks. The side effects of ATO were mild and transient. This regimen of ATO treatment both in induction and post-remission therapy was effective and safe for childhood APL to get long-term survival.

Similar content being viewed by others

References
Wang Z-Y, Chen Z. Acute promyelocytic leukemia: from highly fatal to highly curable. Blood. 2008;111:2505–15.
Bernard J, Weil M, Boiron M, et al. Acute promyelocytic leukemia: results of treatment by daunorubicin. Blood. 1973;41:489–96.
Breitman TR, Collins SJ, Keene BR. Terminal differentiation of human promyelocytic leukemic cells in primary culture in response to retinoic acid. Blood. 1981;57:1000–4.
Chen GQ, Zhu J, Shi XG, et al. In vitro studies on cellular and molecular mechanisms of arsenic trioxide (As2O3) in the treatment of acute promyelocytic leukemia: As2O3 induces NB4 cell apoptosis with downregulation of Bcl-2 expression and modulation of PML-RAR alpha/PML proteins. Blood. 1996;88:1052–61.
Tallman MS, Andersen JW, Schiffer CA, et al. All-trans retinoic acid in acute promyelocytic leukemia: long-term outcome and prognostic factor analysis from the North American Intergroup protocol. Blood. 2002;100:4298–302.
Manola KN. Cytogenetics of pediatric acute myeloid leukemia. Eur J Haematol. 2009;83:391–405.
de Botten S, Coiteux V, Chevret S, et al. Outcome of childhood acute promyelocytic leukemia with all-trans-retinoic acid and chemotherapy. J Clin Oncol. 2004;22:1404–12.
Tallman MS, Abutalib SA, Altman JK. The double hazard of thrombophilia and bleeding in acute promyelocytic leukemia. Semin Thromb Hemost. 2007;33:330–8.
Zhang ZN, Shen T. Diagnosis and therapeutic standard of hematological disease [M]. (Third Version) Beijing: Science Publishing House; 2007. pp 106–202.
Wu ZL. Treatment of acute promyelocytic leukemia and management of the main complication. J Appl Clin Pediatr. 2008;23:1153–6.
Lowenberg B, Griffin JD, Tallman M S. Acute myeloid leukemia and acute promyelocytic leukemia. Hematology Am Soc Hematol Educ Program. 2003;82–101 (review).
Ortega JJ, Madero L, Martin G, et al. Treatment with all-trans-retinoic acid and anthracycline monochemotherapy for children with acute promyelocytic anemia: a multicenter study by the PETHEMA Group. J Clin Oncol. 2005;23:632–40.
Testi AM, Biondi A, LoCoco F, et al. Gimema-A ieopaida: a protocol for the treatment of newly diagnosed acute promyelocytic leukemia (APL) in childhood. Blood. 2005;106:447–53.
Nin C, Yan H, Yu T, et al. Studies on treatment of APL with arsenic trioxide: remission induction, follow-up, and molecular monitoring in 11 newly diagnosed and 47 relapsed APL patients. Blood. 1999;94:3315–24.
Singer JW. Cardiac toxicity of arsenic trioxide. Blood. 2001;98:1633.
Fox E, Razzouk BI, Widemann BC, et al. Phase 1 trial and pharmacokinetic study of arsenic trioxide in children and adolescents with refractory or relapsed acute leukemia, including acute promyelocytic or lymphoma. Blood. 2008;111:566–73.
Tallman MS, Altman JK. Curative strategies in acute promyelocytic leukemia. Hematology Am Soc Hematol Educ Program 2008;391–399.
Ghavamzadeh A, Alimoghaddam K, Ghaffari SH, et al. Treatment of acute promyelocytic leukemia with arsenic trioxide without ATRA and/or chemotherapy. Ann Oncol. 2006;17:131–4.
Mathews V, George B, Lakshmi KM, et al. Single-agent arsenic trioxide in the treatment of newly diagnosed acute promyelocytic leukemia: durable remission with minimal toxicity. Blood. 2006;107:2627–32.
George B, Mathews V, Poonkuzhali B, et al. Treatment of children with newly diagnosed acute promyelocytic leukemia with arsenic trioxide: a single center experience. Leukemia. 2004;18:1587–90.
Zhang L, Zhao H, Zhu X, et al. Retrospective analysis of 65 Chinese children with acute promyelocytic leukemia: a single center experience. Pediatr Blood Cancer. 2008;51:210–5.
Xin L, Wan-jun S, Zeng-jun L, et al. A survival study and prognostic factors analysis on acute promyelocytic leukemia at a single center. Leuk Res. 2007;31:765–71.
Zhang XW, Yan XJ, Zhou ZR, et al. Arsenic trioxide controls the fate of the PML-RARalpha oncoprotein by directly binding PML. Science. 2010;328:240–3.
Acknowledgments
This work was technique supported by Hematology laboratory of ShengJing Hospital of China Medical University.
Conflict of interest statement
The authors declare no competing financial interests.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Wang, H., Hao, L., Wang, X. et al. Retrospective study of arsenic trioxide for childhood acute promyelocytic leukemia in China: a single-center experience. Int J Hematol 91, 820–825 (2010). https://doi.org/10.1007/s12185-010-0575-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-010-0575-z