
Abstract
Background
Social support is a strong and consistent predictor of health outcomes, and social isolation predicts increased morbidity and mortality. The mediating processes are not completely understood.
Purpose
The purpose of the study is to investigate associations between social isolation and cardiovascular and lipid responses to acute stress in the laboratory, and cortisol profiles over the day.
Methods
Cardiovascular and lipid responses to acute stress tasks, and salivary cortisol monitoring, were carried out in 238 healthy middle-aged men and women from the Whitehall II cohort. Social isolation was measured using an adapted version of the Close Persons Questionnaire.
Results
Social isolation was associated with slower post-task recovery of systolic blood pressure in men and women, a higher cholesterol response to stress in men only, and also with larger cortisol awakening responses and greater cortisol output over the day in both men and women.
Conclusions
The impact of social isolation on cardiovascular disease risk may be mediated through stress-related dysregulation of cardiovascular, metabolic, and neuroendocrine processes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Social relationships are of fundamental importance to health, and social support is a strong and consistent predictor of health outcomes [1]. Social support can be measured from a structural or functional perspective, and these may have different effects on health outcomes. Structural support refers to the size, density, and reciprocity of the person’s social network, and social isolation is associated with increased risk of premature mortality and chronic disease morbidity [1, 2]. Functional support reflects the availability of certain types of aid, such as practical support and emotional support. Evidence suggests that both of these measures of social relationships impact on health [3]. Social networks and support may affect health both through behavioral pathways such as influences on healthy lifestyles and adherence to medical recommendations or through direct psychobiological processes [4]. Prospective epidemiological cohort studies have documented associations between lack of social engagement and risk of cardiovascular mortality that remain significant after behavioral factors, comorbidity, and socioeconomic status (SES) are taken into account [5].
Although the biological correlates of social isolation and social support can be investigated in large-scale epidemiological observational studies, more detailed insight is obtained through laboratory psychophysiological studies, in which physiological responses are assessed under controlled conditions, or by carrying out naturalistic biological monitoring in everyday life [6]. Laboratory studies investigating the effects of social support on biological responses have tended to focus on manipulating the availability of support [5]. Less is known about the impact of social isolation and prevailing social support on acute stress responses.
The influence of social networks and social support on acute stress responses has been mixed. An early study by Uchino et al. [7] showed that social support attenuated heart rate (HR) reactions to acute stress in older but not younger family caregivers for people with Alzheimer’s disease. This age effect was replicated in a later study that did not involve caregivers [8]. Knox [9] reported that diastolic blood pressure (DBP) was higher at rest and following acute stress tasks in students with low perceived support, with no differences in systolic blood pressure (SBP). In a later study involving students, there was no main effect of perceived social support on cardiovascular reactivity, but an interaction with hostility, such that greater hostility was associated with larger BP reactions among individuals with high but not low social support [10]. More recently, Nausheen et al. [11] showed no relationship between a measure of structural social support and BP or HR responses to the Trier Social Stress test, but satisfaction with support was inversely related to HR reactivity. To complicate matters further, Hughes [12] found that among female students, greater social support was related to lower BP reactivity, while in male students, the reverse effect was present. Wirtz et al. [13] reported that low perceived social support was associated with greater epinephrine responses to stress in hypertensive but not normotensive adults. Only one study has measured the effects of social support on post-stress recovery, with evidence that greater support is associated with faster BP recovery [14]. Poor blood pressure recovery has been associated with a range of poor health outcomes [15, 16] and is implicated with increased allostatic load [17]. Thus, although several studies have observed potentially protective effects on cardiovascular reactivity, results have varied with support measure, gender, age, and health status. The focus of the present study was on social connectedness and its inverse, social isolation, since these have been related consistently to health outcomes. The first aim of the current study was to assess the relationship between social isolation and acute cardiovascular responses to stress, investigating both reactivity and recovery.
Most studies have measured cardiovascular responses such as BP and HR, but another important indicator is the lipid response to stress. Cholesterol is a clinically recognized predictor of coronary heart disease and is implicated with the development of atherosclerosis. There is extensive evidence that the level of circulating lipids is raised in response to acute stress and emotional arousal [18, 19], and it has also been found that individual differences in acute cholesterol response predict future fasting lipid levels longitudinally [20]. An elevated level of circulating cholesterol is a major risk factor for coronary heart disease, leading to increased infiltration into the intima medial layer of the vessel wall. The relationship between social connectedness and lipid responses to acute mental stress has not been evaluated before. The second aim of our study was to investigate associations between social isolation and lipid responses to acute stress.
Gender differences may be important modulators of these responses. As noted earlier, cardiovascular stress responses have been related differently to social support in men and women [12], and previous work has shown gender differences in lipid response to stress [21]. There is also evidence that men and women differentially utilize social environments in stressful circumstances and that these patterns may be associated with different psychobiological responses [22]. Consequently, we tested for gender differences in associations between stress responses and social isolation.
Naturalistic monitoring studies provide a useful insight into how daily lives affect biological systems and are more ecologically valid than laboratory-based stress tasks [6]. Most previous work in this area has investigated ambulatory BP and HR in relation to social support [23–27]. However, there is some evidence suggesting that cortisol and social support are related. In a sample of Swedish adults, a steeper diurnal cortisol profile was observed in those with higher levels of social support [28]. The rate of decline of cortisol over the day is one marker of hypothalamic–pituitary–adrenocortical (HPA) axis function that may be clinically relevant [29, 30]. Stetler et al. [31] showed that cortisol slopes were flatter among students with low levels of social interaction, although in a more recent investigation, experimental manipulation of social contacts had no overall effect on cortisol slopes [32]. In addition, two other indicators of cortisol output over the day were assessed. The first is the cortisol awakening response (CAR), the rise in cortisol that occurs over the first 30–45 min after waking. Both increases and decreases in CAR have been related to psychosocial risk factors [33], but no previous research has linked the CAR and social connectedness. Second, we measured cortisol output over the day, since this has been related both to chronic stress exposure [34] and to potentially protective factors such as adaptive coping [35]. The third aim of our study was therefore to investigate the relationship between CAR, cortisol diurnal slope, and cortisol output over the day and social isolation.
Social isolation was defined in this study in terms of objective indicators of social connectedness, but it also has psychological correlates. The subjective experience of loneliness is determined in part by perceived lack of social companionship and has previously been associated with cardiovascular, neuroendocrine, and immune responses [36–38]. We therefore tested whether associations between social isolation and biological responses were due to loneliness effects by adding loneliness as a covariate to the analyses.
In summary, we expected to find disturbed cardiovascular responses to stress in more isolated participants, manifest either in greater cardiovascular reactivity or impaired recovery. We anticipated that cholesterol would be elevated post-stress and that this response would be more pronounced in more isolated participants. We also hypothesized that social isolation would be associated with larger CARs, greater cortisol output over the day, and with a flatter cortisol diurnal slope.
Methods
Participants
Participants were drawn from the Whitehall II cohort, a sample of 10,308 London-based civil servants. The original cohort was recruited between 1985 and 1988 to investigate the effects of demographic, psychosocial, and biological risk factors of coronary heart disease [39]. One hundred and twenty eight men and 110 women took part in the current study, which was originally carried out to investigate associations between socioeconomic status (SES) and psychobiological responses [40]. Inclusion criteria were age between 45 and 59 years, living in the London area, full-time working with no plans to retire within 3 years, no history of coronary heart disease, no history of hypertension or medication for hypertension, and no medication that might affect cortisol levels. Participants also agreed to take part in ambulatory blood pressure monitoring (data not discussed here). It was decided to include only participants of white European origin as there is evidence of ethnic difference in cardiovascular reactivity, and ethnic minorities are not well represented in the Whitehall II cohort. Higher (administrative and professional), intermediate (senior executive officers), and lower (executive officers, clerical, office support) grades of employment were included in this study.
Measures
A social isolation index was created using three items adapted from the Close Persons Questionnaire [41]. Participants were asked if they lived alone, saw relatives less than once a month and/or never had any contact with relatives, and saw friends less than once a month and/or never had any contact with friends. Each item was answered as “yes” (scored as 1) or “no” (scored as 0), and these responses were then summed to give a total isolation score. Social isolation scores could therefore range from 0 (no isolation) to 3 (maximum isolation). Because few participants scored the maximum of 3, the groups scoring 2 or 3 were collapsed. Comparisons were therefore made between low (0), medium (1), and high (2–3) social isolation groups.
A previous analysis of this dataset tested associations between stress reactivity and loneliness [36]. Since loneliness is related to social isolation, we included it as a covariate in the analyses. Loneliness was assessed using the UCLA loneliness scale [42]. This consists of 20 items such as “I feel that no one knows me really well” and participants rate how often they have felt that way on a scale from 1 “never” to 4 “often”. Ratings were then summed to give a total loneliness score which could range from 20 (low) to 80 (high).
Blood pressure (BP) and heart rate in the laboratory were monitored continuously using a Portapres-2, a portable version of the Finapres that shows good reliability and accuracy in a range of settings [43]. Blood was collected in serum gel tubes and centrifuged immediately at 2,500 rpm for 10 min at room temperature. The serum was removed and snap frozen at −70 until analysis. Total cholesterol was measured in a centrifugal analyzer by enzymatic colorimetric methods, and HDL cholesterol was determined after dextran sulfate–magnesium chloride precipitation of non-HDL cholesterol. LDL cholesterol is typically computed by using the Friedewald equation. However, the Friedewald equation is not accurate when triglyceride levels are high and is not recommended for studies of nonfasting values. Consequently, we assessed lipid responses in terms of total cholesterol and total:HDL-cholesterol ratio. An increase in the total:HDL cholesterol ratio implies a selective elevation in non-HDL cholesterol.
Laboratory Session Procedure
Each participant underwent a psychophysiological stress testing session in the laboratory. Two challenging behavioral tasks were administered, a color-word interference task, and a mirror-tracing task (see [40] for details). In the first task, a color word (e.g.,. blue, yellow) was presented on a computer screen in an incongruous color. At the bottom of the screen, the names of four colors were displayed written in another color. Participants were required to press a computer key that corresponded to the location of the correct color for the word presented. The second task involved tracing a mirror image of a star using a metal stylus. Participants were told that the average person was able to complete five circuits of the star in the time allowed and were asked to give priority to accuracy rather than speed throughout both tasks. Participants also rated their current level of stress at baseline, immediately after each task, and during the recovery period, on a seven-point Likert scale ranging from 1 “low” to 7 “high”.
Participants were tested individually in either morning or afternoon sessions in a light and temperature-controlled laboratory. Before the study, they were asked not to drink alcohol or have exercised in the evening before or during the day of testing, and not to drink caffeinated drinks or have smoked within 2 h of their research appointment. Body measurements were taken by a research nurse including height, weight, and waist circumference. A questionnaire was used to collect data about smoking, drinking, and medication usage. The Portapres was fitted, and a 21-gauge venous cannula was inserted after which the participant rested for 30 min. Systolic and diastolic BP and heart rate were monitored over the last 5 min of this period to provide baseline values, after which the baseline blood sample was drawn. The two tasks were then performed, each lasting for 5 min. The order of tasks was randomized across participants. Cardiovascular monitoring continued throughout the tasks, and a second blood sample was taken immediately after the two tasks for the analysis of lipids. Blood pressure and heart rate recovery following tasks was indexed by a 5-min average obtained 40- to 45-min post-task.
Cortisol Measures in Daily Life
Saliva samples were collected using cotton dental rolls held in the mouth until saturated, and then stored in Salivette tubes (Sarstedt, Leicester, UK). Participants were instructed to take ten samples over a single working day, with measures on waking up, 30 min later, and then within eight 30-min time windows space at two hourly intervals through the day and evening (08.00–08.30, 10.00–10.30 … 22.00–22.30). Participants were told not to eat, drink tea or coffee, or smoke in the 30 min before each sample was collected. The time of waking was also recorded. Tubes were returned to the investigators personally or by post, and cortisol was analyzed using a biotin–streptavidin fluorescence immunoassay, with inter- and intra-assay coefficients of variation <8%.
Statistical Analyses
The participant characteristics of the three social isolation groups were compared using Chi-square tests for categorical data and univariate analysis of variance for continuous data. Mean values of systolic and diastolic BP and heart rate were calculated for the last 5 min of the baseline, the two 5-min trials, and minutes 40–45 post-tasks (recovery period). The two tasks were then averaged to produce a mean task value. Blood pressure, heart rate, and subjective stress responses were analyzed using repeated measures analysis of variance with trial (baseline, tasks, recovery) as the within-person factor and social isolation and gender as between-person factors. The Greenhouse–Geisser correction of df was applied when the sphericity assumption was violated, but unadjusted dfs are presented in the “Results” section. We also controlled for the effects of age, grade of employment, body mass index, smoking status, and baseline level in analyses of BP and heart rate reactivity (tasks—baseline), since these factors are known to influence responses [40]. Analyses of recovery (45 min—baseline) additionally controlled for reactivity, since more reactive individuals might take longer to recovery following stress. For lipid measures, we analyzed the total cholesterol and total/HDL cholesterol ratio using repeated measures analysis of variance with trial (baseline, task) as the between-person factor and social isolation and gender as between-person factors. Lipid reactivity was analyzed as change between baseline and tasks, controlling for smoking status, grade of employment, body mass index, and age. Three participants were taking statin medication, and they were excluded from the lipid analyses. Analyses were repeated with loneliness as an additional between-person factor, to discover whether associations of biological responses with social isolation remained significant once loneliness is taken into account, or interacted with loneliness. Equipment, blood sampling, or assay failure resulted in some loss of data, so the number of participants analyzed for each variable was as follows: systolic BP—224, diastolic BP—226, heart rate—223, lipids—222.
Separate analyses were carried out of the CAR, cortisol diurnal slope, and cortisol output over the working day. The CAR was defined as the difference between levels on waking and 30 min later. Based on previous analyses of this dataset, participants were excluded from the CAR analysis of the reported time between waking and taking the “waking” cortisol sample which was >10 min [44]. Cortisol was measurable on both waking and 30 min samples in 184 participants, but 31 were excluded, leaving 153 in the analysis. Separate analyses of covariance of cortisol levels on waking and the CAR were conducted, with age, gender, grade of employment, smoking status, BMI, and time of waking as covariates.
The cortisol diurnal slope was computed as the difference between values on waking and the average of the last two cortisol samples (20.00–20.30 and 22.00–22.30) over the day. Cortisol output over the day was estimated using the area under the curve method described by Pruessner and colleagues [45] using the eight measures obtained between 0800 and 2230 hours, and is expressed as output in nmol/l per hour. The relationship with social isolation was again assessed with repeated measures analysis of variance, controlling for age, gender, grade of employment, smoking status, BMI, and time of waking, since these factors all influence cortisol levels [46, 47]. The CAR and cortisol output over the day were normally distributed, but the cortisol slope were skewed so log transformed before analysis. Results are presented as means ± SD.
Results
Participant characteristics are detailed in Table 1. Just over half (129/238) participants had low social isolation scores, with 85 (36%) with medium and 24 (10%) with high social isolation scores. The three social isolation groups did not differ in proportion of men and woman, age, employment grade, smoking status, body mass index, baseline BP, heart rate, or cholesterol. As can be seen in Table 1, participants had BP and cholesterol levels in the normal range on average. Loneliness varied with social isolation, being higher in more socially isolated participants (F (2,235) = 10.18, p < 0.001, \(\eta _p^2 = .08\)).
Laboratory Stress Responses
The pattern of BP, heart rate, and cholesterol responses is summarized in Table 2. Repeated measures analysis of variance confirmed significant effects of trial for systolic BP (F (2,436) = 239.34, p < 0.001, \(\eta _p^2 = .52\)), diastolic BP (F (2,440) = 263.8, p < 0.001, \(\eta _p^2 = .55\)), heart rate (F (2,434) = 225.5, p < 0.001, \(\eta _p^2 = .51\)), total cholesterol (F (1,213) = 57.3, p < 0.001, \(\eta _p^2 = .21\)), total/HDL-cholesterol ratio (F (1,212) = 10.3, p = 0.002, \(\eta _p^2 = .04\)), and subjective stress (F (2,448) = 355.4, p < 0.001, \(\eta _p^2 = .61\)). It can be seen that the tasks induced substantial increases in cardiovascular activity and subjective stress, with return toward baseline by 45 min post-tasks. Both total cholesterol and total/HDL-cholesterol also increased in response to behavioral tasks. There were large individual differences both in responses to tasks and in rate of post-task recovery in all variables.
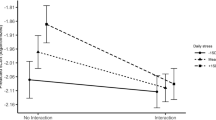
Systolic BP responses to tasks did not differ across social isolation groups either before or after adjustment for covariates (F (2,223) = 0.50, p = 0.61 and F (2,218) = 0.75, p = 0.47), and there was no interaction with gender. There was no main effect of social isolation on systolic blood pressure recovery before adjustment for covariates (F (2,220) = 2.32, p = 0.10). However, there were significant differences in post-task recovery between social isolation groups (F (2,215) = 3.05, p = 0.049, \(\eta _p^2 = .03\)), after adjustment for age, grade of employment, smoking status, BMI, baseline systolic BP, and systolic BP responses to tasks. There was no interaction with gender. As can be seen in Fig. 1, the low social isolation group had more effective systolic BP recovery than the other groups, with differences (adjusted for covariates) between recovery and baseline averaging 4.50 ± 10.1, 7.64 ± 9.2, and 7.47 ± 8.4 mmHg in the low, medium, and high social isolation groups. The social isolation effect remained significant when loneliness was entered into the model (p = 0.05), and social isolation and loneliness did not interact in determining systolic BP recovery. There were no differences related to social isolation in relation to diastolic BP, heart rate, or subjective stress ratings.

Mean systolic blood pressure at baseline (base), post-task (tasks), and recovery (recovery) for high social isolation group (solid line), medium social isolation group (dashed line), and low social isolation group (dotted line). Error bars are standard error of the mean (SEM)
The analysis of total/HDL-cholesterol ratio responses to stress showed a significant interaction between gender and social isolation, before and after adjustment for covariates (F (2,212) = 3.32, p = 0.041, \(\eta _p^2 = .03\) and F (2,207) = 3.08, p = 0.047, \(\eta _p^2 = .03\)). The adjusted means are shown in Fig. 2, controlling for baseline total/hdl level, age, grade of employment, BMI, and smoking status. It is apparent that socially isolated men had large total/HDL-cholesterol responses to stress, while social isolation was not related to responsivity in women. This was confirmed in post hoc analyses of the two genders separately, in which the difference between social isolation groups was significant in men (p = 0.025) but not women (p = 0.98). When loneliness was included as a factor in the analysis, the effect of social isolation remained significant in men (p = 0.033), and no interaction with loneliness was observed.

Mean total:HDL cholesterol response across social isolation groups in men (solid bar) and women (clear bar). Error bars are SEM
Cortisol Over the Day
The profile of salivary cortisol in the three social isolation groups is shown in Fig. 3. Participants woke on average at 0639 hours, with no differences between groups. Cortisol levels did not differ between groups on waking, and there was no effect of social isolation before adjustment for covariates (F (2,151) = 0.85, p = 0.427), but there was a significant effect of social isolation on the CAR (F (2,143) = 3.03, p = 0.022, \(\eta _p^2 = .04\)), after adjustment for age, grade of employment, BMI, smoking status, cortisol level on waking, and time of waking. This effect did not interact with gender. The CAR averaged 8.7 ± 15.6, 8.4 ± 12.9, and 17.5 ± 15.8 nmol/l in the low, medium, and high social isolation groups, indicating that more isolated individuals had greater CARs. The association between the CAR and social isolation remained significant after loneliness was included in the analysis (p = 0.031), and did not interact with loneliness.

Mean salivary cortisol across the day for high social isolation group (solid line), medium social isolation group (dashed line), and low social isolation group (dotted line)
The analysis of cortisol output over the day also revealed a main effect of social isolation (F (2,142) = 3.03, p = 0.015, \(\eta _p^2 = .04\)), after adjustment for age, grade of employment, BMI, smoking status, and time of waking. Additional analyses showed that there was no interaction with gender. Total cortisol output averaged 99.2 ± 29.5, 103.9 ± 45.1, and 125.8 ± 52.9 nmol/l in the low, medium, and high isolation groups, after adjustment for covariates. The association remained significant after including loneliness as a factor (p = 0.036), and there was no interaction between social isolation and loneliness. Thus, the psychobiological activation of socially isolated people recorded in the laboratory was mirrored by heightened cortisol output both in the early morning and over the remainder of the day and evening. By contrast, there was no significant association between social isolation and the cortisol slope over the day (F (2,142) = 0.59, p = 0.56).
Discussion
The results of this study indicated that greater social isolation in this sample was associated with delayed post-task recovery of systolic blood pressure, larger total/HDL cholesterol ratio response to stress in socially isolated men, and a higher CAR and greater total cortisol output over the day in both men and women. These associations were independent of loneliness and other covariates.
The Close Persons Questionnaire used in this study was designed to measure amount of social contact and allowed us to compare those at opposite ends of the social isolation spectrum. It did not provide such a refined measure of social isolation as possible with an instrument such as the Social Network index [48]. Relatively few participants (10%) in this study were very socially isolated on the measures used here, as might be expected in a population of middle-aged men and women in full-time employment. Nevertheless, associations between social isolation and cardiovascular, lipid, and neuroendocrine measures were present. This suggests that the basic experience of social isolation can be relevant for health outcomes.
Delayed post-stress recovery of systolic blood pressure was associated with social isolation. There have been few studies assessing the relationship between cardiovascular reactivity and social connectedness [11], and associations with post-stress recovery have not been described. Previous findings linking social support with cardiovascular reactivity to stress have been inconsistent. Some studies have reported no relationship between social support and blood pressure reactivity [8, 9], a pattern that was also observed here. Much of the research on cardiovascular reactivity has investigated samples of young adults, and there may be important age differences [7]. Roy et al. [14] found that social support was related to both blood pressure reactivity and recovery, a finding partly replicated in the current study, since we also found an effect for systolic blood pressure recovery. Delayed post-stress recovery of systolic blood pressure has been associated with delayed recovery of a number of other biomarkers including heart rate and plasma viscosity [16] and has also been shown to predict rises in clinical blood pressure over a 3-year prospective period [49]. No differences were recorded in diastolic pressure or heart rate responses, but several studies indicate that systolic blood pressure is more sensitive to psychosocial factors [50].
In the present study, we found a significant interaction between cholesterol reactivity to stress and social isolation in men, but no effect for women. Previous work has shown males to have had a higher lipid response to stress in a laboratory setting [21], although this has not been consistently replicated [51]. Men and women did not differ in subjective response to stress or other biological measures such as blood pressure, so this cannot explain the disparity between men and women in lipid responses. The finding that socially isolated men had greater cholesterol reactivity to stress may be particularly important for health as men are at a higher risk of coronary artery disease in middle age. Individual differences in acute stress responses in LDL, HDL, and total cholesterol were found to predict fasting HDL and total:HDL cholesterol ratio in a 3-year follow-up study [20], showing that although the changes in cholesterol may be small, they are clinically relevant. Epidemiological evidence has consistently demonstrated that men seem to have a greater health benefit from marriage than women [52, 53] which further underlines the role of gender in relation to the effects of social isolation.
There was no relationship between social isolation and awakening cortisol level; however, we did find a significant effect of social isolation on the rise in cortisol after waking. Examination of the mean CAR shows that this effect was due to differences between the high compared with the middle and low isolation groups. This effect was also found in the analysis of cortisol output over the day. The high social isolation group had a higher cortisol output compared to the low and middle groups. Our previous analysis found an association between loneliness and CAR, but no effect for cortisol level over the day [36]. Turner-Cobb et al. [54] reported that mean salivary cortisol level was related to quality of social support but not social network size, and this is supported in other work [55]. However, our findings show that a high level of social isolation is related to an elevated cortisol profile. A heightened CAR has previously been associated with psychosocial factors such as general and work stress, and financial strain and psychological traits including high neuroticism and low optimism [33, 56]. We were not, however, able to confirm previous findings that greater social contact is associated with steeper cortisol rhythms over the day [31].
The associations we observed between social isolation and biological responses were independent of loneliness. Our results imply that the impact of low social connectedness on biological responses was not mediated through the subjective experience of isolation and loneliness. It could be that other unmeasured correlates of social isolation are responsible. But feelings of loneliness are experienced to some extent independently of objective social activity and discrepancies between the two are observed [57]. Other studies have also demonstrated independent associations between biological responses and loneliness and social networks [58]. Additionally, loneliness may arise through a perceived lack of intimacy (emotional loneliness) or lack of companionship (social loneliness). Our social isolation measure may be a stronger reflection of lack of companionship, and it is possible that the health-related biological correlates of loneliness involve lack of intimacy and emotional loneliness.
There are a number of limitations to this study. Firstly, the design was cross-sectional in nature, so it is not possible to infer causality. Secondly, the sample was restricted to middle-aged participants from White European ethnicity, and therefore, we cannot generalize our findings to other age groups, socioeconomic groups, or ethnic groups. We found that there were significant effects of social isolation on blood pressure recovery, but it was not possible to test for the recovery effects in the cholesterol analysis, as no sample was collected at recovery time. Third, even though the measure of social isolation allowed us to examine effects across three categories, other measures could have provided greater gradations, allowing for more subtle differences to be tested. Finally, there were only 24 participants in the high social isolation group, and the sample size was further reduced when carrying out the between-gender analysis. Although we found gender differences in the cholesterol analyses, it is possible that significant effects may have emerged for other variables if we had greater power.
Despite these considerations, this study builds upon the literature examining the effects of social isolation on health outcomes using both laboratory and naturalistic methods. High levels of social isolation were associated with negative cardiovascular, metabolic, and neuroendocrine process and, therefore, suggests that the impact of social isolation on cardiovascular disease risk may be mediated by dysregulation of these systems. It is important to identify areas for further research and practical application. Interventions aimed at increasing perceived social support such as the Enhancing Recovery in Coronary Heart Disease (ENRICHD) trial have not found that increasing social support in post-myocardial infarction patients leads to favorable cardiovascular outcomes [59]. However, the impact of interventions designed to increase social connectedness and reduce isolation on stress responsivity has not yet been evaluated. Studies of this type would clarify the causal relationships between biological stress responsivity and social isolation.
References
House JS, Landis KR, Umberson D. Social relationships and health. Science. 1988; 241: 540–545.
Lett HS, Blumenthal JA, Babyak MA, Strauman TJ, Robins C, Sherwood A. Social support and coronary heart disease: Epidemiologic evidence and implications for treatment. Psychosom Med. 2005; 67: 869–878.
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985; 98: 310–357.
Uchino BN, Cacioppo JT, Kiecolt-Glaser JK. The relationship between social support and physiological processes: A review with emphasis on underlying mechanisms and implications for health. Psychol Bull. 1996; 119: 488–531.
Ramsay S, Ebrahim S, Whincup P, et al. Social engagement and the risk of cardiovascular disease mortality: Results of a prospective population-based study of older men. Ann Epidemiol. 2008; 18: 476–483.
Steptoe A. Tools of psychosocial biology in health care research. In: Bowling A, Ebrahim S, eds. Handbook of Health Research Methods. Oxford: Oxford University Press; 2005: 471–493.
Uchino BN, Kiecolt-Glaser JK, Cacioppo JT. Age-related changes in cardiovascular response as a function of a chronic stressor and social support. J Pers Soc Psychol. 1992; 63: 839–846.
Uchino BN, Holt-Lunstad J, Uno D, Flinders JB. Heterogeneity in the social networks of young and older adults: Prediction of mental health and cardiovascular reactivity during acute stress. J Behav Med. 2001; 24: 361–382.
Knox SS. Perception of social support and blood pressure in young men. Percept Mot Skills. 1993; 77: 132–134.
Chen YY, Gilligan S, Coups EJ, Contrada RJ. Hostility and perceived social support: interactive effects on cardiovascular reactivity to laboratory stressors. Ann Behav Med. 2005; 29: 37–43.
Nausheen B, Gidron Y, Gregg A, Tissarchondou HS, Peveler R. Loneliness, social support and cardiovascular reactivity to laboratory stress. Stress. 2007; 10: 37–44.
Hughes BM. Social support in ordinary life and laboratory measures of cardiovascular reactivity: Gender differences in habituation-sensitization. Ann Behav Med. 2007; 34: 166–176.
Wirtz PH, von Kanel R, Mohiyeddini C, et al. Low social support and poor emotional regulation are associated with increased stress hormone reactivity to mental stress in systemic hypertension. J Clin Endocrinol Metab. 2006; 91: 3857–3865.
Roy MP, Steptoe A, Kirschbaum C. Life events and social support as moderators of individual differences in cardiovascular and cortisol reactivity. J Pers Soc Psychol. 1998; 75: 1273–1281.
Steptoe A, Donald AE, O’Donnell, et al. Delayed blood pressure recovery after psychological stress is associated with carotid intima–media thickness: Whitehall psychobiology study. Arterioscler Thromb Vasc Biol. 2006; 26: 2547–2551.
Steptoe A, Marmot M. Psychosocial, hemostatic, and inflammatory correlates of delayed poststress blood pressure recovery. Psychosom Med. 2006; 68: 531–537.
McEwen BS. Protective and damaging effects of stress mediators. N Engl J Med. 1998; 338: 171–179.
Bachen EA, Muldoon MF, Matthews KA, Manuck SB. Effects of hemoconcentration and sympathetic activation on serum lipid responses to brief mental stress. Psychosom Med. 2002; 64: 587–594.
Dimsdale JE, Herd JA. Variability of plasma lipids in response to emotional arousal. Psychosom Med. 1982; 44: 413–430.
Steptoe A, Brydon L. Associations between acute lipid stress responses and fasting lipid levels 3 years later. Health Psychol. 2005; 24: 601–607.
Stoney CM, Matthews KA, McDonald RH, Johnson CA. Sex differences in lipid, lipoprotein, cardiovascular, and neuroendocrine responses to acute stress. Psychophysiology. 1988; 25: 645–656.
Taylor SE, Klein LC, Lewis BP, Gruenewald TL, Gurung RA, Updegraff JA. Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychol Rev. 2000; 107: 411–429.
Linden W, Chambers L, Maurice J, Lenz JW. Sex differences in social support, self-deception, hostility, and ambulatory cardiovascular activity. Health Psychol. 1993; 12: 376–380.
Brownley KA, Light KC, Anderson NB. Social support and hostility interact to influence clinic, work, and home blood pressure in black and white men and women. Psychophysiology. 1996; 33: 434–445.
Horsten M, Ericson M, Perski A, Wamala SP, Schenck-Gustafsson K, Orth-Gomer K. Psychosocial factors and heart rate variability in healthy women. Psychosom Med. 1999; 61: 49–57.
Steptoe A. Stress, social support and cardiovascular activity over the working day. Int J Psychophysiol. 2000; 37: 299–308.
Rodriguez CJ, Burg MM, Meng J, et al. Effect of social support on nocturnal blood pressure dipping. Psychosom Med. 2008; 70: 7–12.
Sjogren E, Leanderson P, Kristenson M. Diurnal saliva cortisol levels and relations to psychosocial factors in a population sample of middle-aged Swedish men and women. Int J Behav Med. 2006; 13: 193–200.
Sephton SE, Sapolsky RM, Kraemer HC, Spiegel D. Diurnal cortisol rhythm as a predictor of breast cancer survival. J Natl Cancer Inst. 2000; 92: 994–1000.
Abercrombie HC, Giese-Davis J, Sephton S, Epel ES, Turner-Cobb JM, Spiegel D. Flattened cortisol rhythms in metastatic breast cancer patients. Psychoneuroendocrinology. 2004; 29: 1082–1092.
Stetler C, Dickerson SS, Miller GE. Uncoupling of social zeitgebers and diurnal cortisol secretion in clinical depression. Psychoneuroendocrinology. 2004; 29: 1250–1259.
Stetler CA, Miller GE. Social integration of daily activities and cortisol secretion: A laboratory based manipulation. J Behav Med. 2008; 31: 249–257.
Chida Y, Steptoe A. Cortisol awakening response and psychosocial factors: A systematic review and meta-analysis. Biol Psychol. 2009; (in press).
McEwen BS, Biron CA, Brunson KW. The role of adrenocorticoids as modulators of immune function in health and disease: Neural, endocrine and immune interactions. Brain Res Brain. 1997; 23: 79–133.
O’Donnell K, Badrick E, Kumari M, Steptoe A. Psychological coping styles and cortisol over the day in healthy older adults. Psychoneuroendocrinology. 2008; 33: 601–611.
Steptoe A, Owen N, Kunz-Ebrecht SR, Brydon L. Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses in middle-aged men and women. Psychoneuroendocrinology. 2004; 29: 593–611.
Cacioppo JT, Hawkley LC, Crawford LE, et al. Loneliness and health: Potential mechanisms. Psychosom Med. 2002; 64: 407–417.
Adam EK, Hawkley LC, Kudielka BM, Cacioppo JT. Day-to-day dynamics of experience–cortisol associations in a population-based sample of older adults. Proc Natl Acad Sci USA. 2006; 103: 17058–17063.
Marmot MG, Smith GD, Stansfeld S, et al. Health inequalities among British civil servants: The Whitehall II study. Lancet. 1991; 337: 1387–1393.
Steptoe A, Feldman PJ, Kunz S, Owen N, Willemsen G, Marmot M. Stress responsivity and socioeconomic status: A mechanism for increased cardiovascular disease risk? Eur Heart J. 2002; 23: 1757–1763.
Stansfeld S, Marmot M. Deriving a survey measure of social support: The reliability and validity of the close persons questionnaire. Soc Sci Med. 1992; 35: 1027–1035.
Russell D, Peplau LA, Cutrona CE. The revised UCLA loneliness scale: Concurrent and discriminant validity evidence. J Pers Soc Psychol. 1980; 39: 472–480.
Imholz BP, Wieling W, van Montfrans GA, Wesseling KH. Fifteen years experience with finger arterial pressure monitoring: Assessment of the technology. Cardiovasc Res. 1998; 38: 605–616.
Kunz-Ebrecht SR, Kirschbaum C, Marmot M, Steptoe A. Differences in cortisol awakening response on work days and weekends in women and men from the Whitehall II cohort. Psychoneuroendocrinology. 2004; 29: 516–528.
Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology. 2003; 28: 916–931.
Steptoe A, Kunz-Ebrecht S, Owen N, et al. Socioeconomic status and stress-related biological responses over the working day. Psychosom Med. 2003; 65: 461–470.
Steptoe A, Ussher M. Smoking, cortisol and nicotine. Int J Psychophysiol. 2006; 59: 228–235.
Cohen S, Doyle WJ, Skoner DP, Rabin BS, Gwaltney JM Jr. Social ties and susceptibility to the common cold. Jama. 1997; 277: 1940–1944.
Steptoe A, Marmot M. Impaired cardiovascular recovery following stress predicts 3-year increases in blood pressure. J Hypertens. 2005; 23: 529–536.
Chida Y, Hamer M. Chronic psychosocial factors and acute physiological responses to laboratory induced stress in the healthy populations: A quantitative review of 30 years of investigations. Psychol Bull. 2009; 134(6): 829–885.
van Doornen LJP, Snieder H, Boomsma DI. Serum lipids and cardiovascular reactivity to stress. Biol Psychol. 1998; 47: 279–297.
Ben-Shlomo Y, Smith GD, Shipley M, Marmot MG. Magnitude and causes of mortality differences between married and unmarried men. J Epidemiol Community Health. 1993; 47: 200–205.
Lund R, Holstein BE, Osler M. Marital history from age 15 to 40 years and subsequent 10-year mortality: A longitudinal study of Danish males born in 1953. Int J Epidemiol. 2004; 33: 389–397.
Turner-Cobb JM, Sephton SE, Koopman C, Blake-Mortimer J, Spiegel D. Social support and salivary cortisol in women with metastatic breast cancer. Psychosom Med. 2000; 62: 337–345.
Seeman TE. Social ties and health: The benefits of social integration. Ann Epidemiol. 1996; 6: 442–451.
Portella MJ, Harmer CJ, Flint J, Cowen P, Goodwin GM. Enhanced early morning salivary cortisol in neuroticism. Am J Psychiatry. 2005; 162: 807–809.
Fees BS, Martin P, Poon LW. A model of loneliness in older adults. J Gerontol B Psychol Sci Soc Sci. 1999; 54: P231–P239.
Pressman SD, Cohen S, Miller GE, Barkin A, Rabin BS, Treanor JJ. Loneliness, social network size, and immune response to influenza vaccination in college freshmen. Health Psychol. 2005; 24: 297–306.
Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: The enhancing recovery in coronary heart disease patients (ENRICHD) randomized trial. J Am Med Assoc. 2003; 289: 3106–3116.
Acknowledgements
This study was supported by the Medical Research Council, UK, and by the British Heart Foundation. Nina Grant is supported by the Economic and Social Research Council and the Medical Research Council. We are grateful to Gonneke Willemsen, Sabine Kunz-Ebrecht, Pamela J Feldman, Natalie Owen, and Bev Murray for their contribution to data collection and analysis.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Grant, N., Hamer, M. & Steptoe, A. Social Isolation and Stress-related Cardiovascular, Lipid, and Cortisol Responses. ann. behav. med. 37, 29–37 (2009). https://doi.org/10.1007/s12160-009-9081-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-009-9081-z