
Abstract
Objective
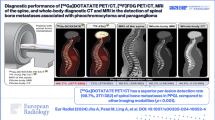
To investigate whether integrated fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) can differentiate benign from adrenal malignant lesions on the basis of maximum standardized uptake value (SUVmax), tumor/liver (T/L) SUVmax ratio, and CT attenuation value (Hounsfield Units; HU) of unenhanced CT obtained from FDG-PET/CT data.
Methods
We studied 30 patients with 35 adrenal lesions (16 adrenal benign lesions, size 16 ± 5 mm, in 15 patients; and 19 adrenal malignant lesions, 24 ± 12 mm, in 15 patients) who had confirmed primary malignancies (lung cancer in 23 patients, lymphoma in 2, esophageal cancer in 2, hypopharyngeal cancer in 1, prostate cancer in 1, and 1 patient in whom lesions were detected at cancer screening). All patients underwent PET/CT at 1 h post FDG injection. Diagnosis of adrenal malignant lesions was based on interval growth or reduction after chemotherapy. An adrenal mass that remained unchanged for over 1 year was the standard used to diagnose adrenal benign lesions. Values of FDG uptake and CT attenuation were measured by placing volumetric regions of interest over PET/CT images. Adrenal uptake of SUVmax ≥ 2.5 was considered to indicate a malignant lesion; SUVmax < 2.5 was considered to indicate a benign lesion. In further analysis, 1.8 was employed as the threshold for the T/L SUVmax ratio. Unenhanced CT obtained from PET/CT data was considered positive for adrenal malignant lesions based on a CT attenuation value ≥ 10 HU; lesions with a value < 10 HU were considered adrenal benign lesions. Mann–Whitney’s U test was used for statistical analyses.
Results
SUVmax in adrenal malignant lesions (7.4 ± 3.5) was higher than that in adrenal benign lesions (2.1 ± 0.5, p < 0.05). The CT attenuation value of adrenal malignant lesions (27.6 ± 11.9 HU) was higher than that of adrenal benign lesions (10.1 ± 12.3 HU, p < 0.05). In differentiating between adrenal benign and malignant lesions, a CT threshold of 10 HU corresponded to a sensitivity of 57%, specificity of 94%, accuracy of 74%, positive predictive value of 92% and negative predictive value of 65%. An SUVmax cut-off value of 2.5 corresponded to a sensitivity of 89%, specificity of 94%, accuracy of 91%, positive predictive value of 94% and negative predictive value of 88%. The T/L SUVmax ratio was 1.0 ± 0.2 for adrenal benign lesions and 4.5 ± 3.0 for adrenal malignant lesions. And T/L SUVmax ratio cut-off value of 1.8 corresponded to a sensitivity of 85%, specificity of 100%, accuracy of 91%, positive predictive value of 100% and negative predictive value of 83%.
Conclusions
FDG-PET/CT with additional SUVmax analysis improves the diagnostic accuracy of adrenal lesions in cancer patients.


Similar content being viewed by others


References
Inan N, Arslan A, Akansel G, Anik Y, Balci NC, Demirci A. Dynamic contrast enhanced MRI in the differential diagnosis of adrenal adenomas and malignant adrenal masses. Eur J Radiol. 2008;65:154–62.
Tsushima Y, Ishizaka H, Matsumoto M. Adrenal masses: differentiation with chemical shift, fast low-angle shot MR imaging. Radiology. 1993;186:705–9.
Miyake H, Takaki H, Matsumoto S, Yoshida S, Maeda T, Mori H. Adrenal nonhyperfunctioning adenoma and nonadenoma: CT attenuation value as discriminative index. Abdom Imaging. 1995;20:559–62.
McNicholas MM, Lee MJ, Mayo-Smith WW, Hahn PF, Boland GW, Mueller PR. An imaging algorithm for the differential diagnosis of adrenal adenomas and metastases. AJR Am J Roentgenol. 1995;165:1453–9.
Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM, Mueller PR. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol. 1998;171:201–4.
Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F. CT time-attenuation washout curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol. 1998;170:747–52.
Hamrahian AH, Ioachimescu AG, Remer EM, Motta-Ramirez G, Bogabathina H, Levin HS, et al. Clinical utility of noncontrast computed tomography attenuation value (hounsfield units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland Clinic experience. J Clin Endocrinol Metab. 2005;90:871–7.
Lee MJ, Hahn PF, Papanicolaou N, Egglin TK, Saini S, Mueller PR, et al. Benign and malignant adrenal masses: CT distinction with attenuation coefficients, size, and observer analysis. Radiology. 1991;179:415–8.
Park BK, Kim CK, Kim B, Choi JY. Comparison of delayed enhanced CT and 18F-FDG PET/CT in the evaluation of adrenal masses in oncology patients. J Comput Assist Tomogr. 2007;31:550–6.
Park BK, Kim CK, Kim B, Lee JH. Comparison of delayed enhanced CT and chemical shift MR for evaluating hyperattenuating incidental adrenal masses. Radiology. 2007;243:760–5.
Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Goodsitt M. Delayed enhanced CT for differentiation of benign from malignant adrenal masses. Radiology. 1996;200:737–42.
Caoili EM, Korobkin M, Francis IR, Cohan RH, Platt JF, Dunnick NR, et al. Adrenal masses: characterization with combined unenhanced and delayed enhanced CT. Radiology. 2002;222:629–33.
Tessonnier L, Sebag F, Palazzo FF, Colavolpe C, De Micco C, Mancini J, et al. Does (18)F-FDG PET/CT add diagnostic accuracy in incidentally identified non-secreting adrenal tumours? Eur J Nucl Med Mol Imaging. 2008;35:2018–25.
Beck JR. Likelihood ratios. Another enhancement of sensitivity and specificity. Arch Pathol Lab Med. 1986;110:685–6.
Caoili EM, Korobkin M, Brown RK, Mackie G, Shulkin BL. Differentiating adrenal adenomas from nonadenomas using (18)F-FDG PET/CT: quantitative and qualitative evaluation. Acad Radiol. 2007;14:468–75.
Yun M, Kim W, Alnafisi N, Lacorte L, Jang S, Alavi A. 18F-FDG PET in characterizing adrenal lesions detected on CT or MRI. J Nucl Med. 2001;42:1795–9.
Jana S, Zhang T, Milstein DM, Isasi CR, Blaufox MD. FDG-PET and CT characterization of adrenal lesions in cancer patients. Eur J Nucl Med Mol Imaging. 2006;33:29–35.
Gupta NC, Graeber GM, Tamim WJ, Rogers JS, Irisari L, Bishop HA. Clinical utility of PET-FDG imaging in differentiation of benign from malignant adrenal masses in lung cancer. Clin Lung Cancer. 2001;3:59–64.
Lowe VJ, DeLong DM, Hoffman JM, Coleman RE. Optimum scanning protocol for FDG-PET evaluation of pulmonary malignancy. J Nucl Med. 1995;36:883–7.
Boerner AR, Weckesser M, Herzog H, Schmitz T, Audretsch W, Nitz U, et al. Optimal scan time for fluorine-18 fluorodeoxyglucose positron emission tomography in breast cancer. Eur J Nucl Med. 1999;26:226–30.
Nakamoto Y, Higashi T, Sakahara H, Tamaki N, Kogire M, Doi R, et al. Delayed (18)F-fluoro-2-deoxy-d-glucose positron emission tomography scan for differentiation between malignant and benign lesions in the pancreas. Cancer. 2000;89:2547–54.
Acknowledgments
We thank Atsushi Kubo of Department of Radiology in Keio University school of Medicine for the advice of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okada, M., Shimono, T., Komeya, Y. et al. Adrenal masses: the value of additional fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) in differentiating between benign and malignant lesions. Ann Nucl Med 23, 349–354 (2009). https://doi.org/10.1007/s12149-009-0246-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-009-0246-4