
Abstract
Trajectories of poverty influence the mental health of mothers and children. Previous studies utilize objective measures despite the importance of subjective measures of poverty. Furthermore, chronic economic hardship may erode personal resources such as self-esteem which increases vulnerability to mental health issues. Trajectories of perceived family economic hardship and their relationship with common mental health disorders, as mediated by self-esteem, were investigated in 511 mother–child dyads from Singapore. Three distinct groups of economic hardship trajectories were delineated, namely the low stable, high stable and moderate decreasing group. The high stable group was found to be associated with a greater likelihood of mother’s depression, mother’s anxiety and child’s anxiety when compared to the low stable group. The moderate decreasing group was found to be associated with a greater likelihood of mother’s anxiety when compared to the low stable group. Mother’s self-esteem was found to mediate all the significant relations found. These findings indicate the existence of distinct trajectories of perceived economic hardship within low-income families and their relation with mental health outcomes in mothers and children. The mediation of these relations by mother’s self-esteem suggests the importance of enhancing self-esteem in mothers from low-income backgrounds.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low-income families experiencing financial difficulties are placed at a greater risk of developing mental health issues. The mental health of individuals from low-income families is shaped by the social, environmental and economic conditions in which they live (Alegría et al., 2018). Income inequality has been described to be related to psychosocial stress, where individuals from low-income families may be exposed to dangerous environments, present with stressful, unrewarding or depersonalizing work, lack the necessities and amenities of life, or are isolated from information and support (Murali & Oyebode, 2004). Given the multiple stressors that these individuals face, it is not surprising that poverty is associated with common mental disorders such as depression and anxiety in adults (Sareen et al., 2011) and children (Assing-Murray & Lebrun-Harris, 2020) from low-income backgrounds.
A large portion of studies on poverty and mental health utilize cross-sectional data, which omits the histories of poverty that individuals experience. Longitudinal trajectories of poverty could provide rich information on the duration of time in a state of poverty or changes to the state of poverty. Indeed, studies have found that trajectories of poverty influence the mental health of mothers and children from low-income families (Comeau & Boyle, 2018; Pryor et al., 2019; Wickham et al., 2017). In one study, transition into poverty increased the likelihood of socioemotional behavioural problems in children and psychological distress in mothers (Wickham et al., 2017). In another study, compared to children who did not experience poverty, those who experienced intermittent poverty had a greater risk of psychological difficulties such as conduct problems or stress (Pryor et al., 2019). In yet another study, children who were always poor experienced the greatest mean level of internalizing problems, followed by those who were intermittently poor and those who were never poor (Comeau & Boyle, 2018).
Literature shows that poverty can be defined both objectively and subjectively. Objective measures define poverty as having less than an absolute minimum or having less than others in society, while subjective measures define poverty as the feeling of not having enough to get along (Hagenaars & de Vos, 1988). Many of the aforementioned studies investigating longitudinal trajectories of poverty (Comeau & Boyle, 2018; Pryor et al., 2019; Wickham et al., 2017) use objective measures such as income to determine the individual’s state of poverty, omitting the individual’s subjective experience of poverty. Studies in developed countries state that the subjective well-being of the individual depends not only on the individual’s standard of living but their economic standing relative to others (Luttmer, 2005). According to Runciman (1966), individuals compare their own living standard with others in society and feel deprived as they fall below the standards of living which are attained by the majority in society. Indeed, previous studies have shown that subjective poverty is a social determinant of mental outcomes above and beyond the effects of household income (Chung et al., 2018), and that subjective measures but not objective measures of poverty are associated with mental health (Ahnquist & Wamala, 2011). These studies underscore the limitations of using income alone to define poverty and to investigate relations with mental health outcomes, particularly in developed societies where the psychological stress that results from relative deprivation could be more closely linked to mental health issues.
Family economic hardship is an alternative indicator of poverty that captures the family’s subjective experiences of material hardship and stresses arising from financial difficulties. Indeed, studies investigating family economic hardship have found significant relations with outcomes in adults (Neppl et al., 2016) and children (Zhang et al., 2020). However, given the varying developmental contexts of adults and children in the family (Berk, 2017), the effect of family economic hardship over time could impact each family member differently. Thus, it is important to study the effect of trajectories of family economic hardship on common mental health disorders (e.g., depression and anxiety) in both mothers and children.
The Stress Process Model (Pearlin et al., 1981) posits that the impact of chronic stressors such as economic hardship are not limited to the direct effect on mental health, they also impact personal resources. One such personal resource is individual self-esteem, which refers to an individual’s positive or negative attitude toward the self as a totality (Rosenberg et al., 1995). Economic hardship may erode personal resources such as self-esteem and increase vulnerability to the development of mental health problems (Pearlin et al., 1981). Indeed, studies have shown that self-esteem mediates the relationship between economic hardship and mental health in adults (Lee & Allen, 2020; Wickrama et al., 2012). However, there is a lack of studies investigating these mediating relationships in children. We were interested in investigating whether the individual self-esteem of the mother or child would play a mediating role between trajectories of family economic hardship and the mental health of the same individual (i.e., mother or child). Furthermore, separate studies have investigated relations between economic hardship and self-esteem of women (Wickrama et al., 2012), maternal self-esteem and mother–child interactions (Aunola et al., 1999) and the consequential impact of mother–child interactions on child mental health outcomes (Dietz et al., 2008). More specifically, greater economic hardship was associated with lower self-esteem of women from rural backgrounds (Wickrama et al., 2012). Lower self-esteem of mothers was associated with less authoritarian parenting (Aunola et al., 1999) and mothers who displayed more disengaged parenting had children with a higher risk of depression (Dietz et al., 2008). Thus, we were interested in exploring whether the mother’s self-esteem would serve as the mediator between family economic hardship trajectories and the mental health of the child. Lastly, based on criticisms of the unilateral model of parent–child relations, where the parent mainly influences the child in parent–child interaction, we explored the bilateral model of parent–child relations (Kuczynski, 2003). In this model, the child similarly exerts an influence on the parent through parent–child interactions. Thus, we were also interested in whether the child’s self-esteem could serve as a mediator between family economic hardship trajectories and mother’s mental health.
The present study sought to develop an understanding of the potential relationship of trajectories of perceived economic hardship and the mental health of mothers and children from low-income families using a longitudinal design. The longitudinal design of the present study utilized three waves, where data collection was conducted six months apart, similar to other studies in adults (Tan et al., 2021) and children (Demaray et al., 2005). The first aim of the study was to investigate the relationship between trajectories of family economic hardship and the risk of clinical levels of (a) depression and (b) anxiety in (i) mothers and (ii) children. We hypothesized that the latent classes of economic hardship trajectories would be associated with clinical levels of depression and anxiety in both mothers and children based on evidence investigating these relations using objective measures of poverty (Comeau & Boyle, 2018; Pryor et al., 2019; Wickham et al., 2017). The second aim of the study was to investigate, in an exploratory analysis, if the self-esteem of the mother or child would mediate the significant relationships found between the trajectories of economic hardship and mental health of mother and child. We investigated if the (a) individual’s self-esteem would mediate these relations, or if the (b) self-esteem of the other individual in the mother–child dyad would mediate these relations. Based on these aims, two possible patterns of results could occur: (a) the mother’s self-esteem would mediate the relation between trajectories of family economic hardship and mother’s mental health, or the child’s self-esteem would mediate the relation between trajectories of family economic hardship and child’s mental health; (b) the mother’s self-esteem would mediate the relation between trajectories of family economic hardship and child’s mental health, or child’s self-esteem would mediate the relation between trajectories of family economic hardship and mother’s mental health. Given the exploratory nature of this analysis, no hypotheses were made regarding it. A conceptual model summarizing the study aims is shown in Fig. 1.

Conceptual model of study aims. ‘IV’ represent the independent variable, ‘MV’ represents the mediator variable and ‘DV’ represents the dependent variable
Methods
Participants
Mother–child dyads were recruited for a study on low-income families in Singapore (Goh et al., 2019). The study recruited mother–child dyads whose families 1) were receiving government financial aid at the time of recruitment or had previously received financial aid at one point during the three years before the time of recruitment; and 2) had a child between 7 and 12 years of age. Government financial aid provided temporary financial support to low-income individuals or families who were temporarily unable to work, were looking for a job or were earning a low income and required assistance. Wave 1, wave 2 and wave 3 of the study were conducted from June 2019 to August 2019, December 2019 to February 2020, and June 2020 to October 2020. Five hundred and eleven mother–child dyads were recruited for this study at wave 1. Thirty-one mother–child dyads dropped out after wave 1 due to difficulty in contacting the mother, mother’s lack of time for the survey, child not residing with mother and mother passing away. The resulting sample size for wave 2 was 480. Eighteen mother–child dyads dropped out from wave 2 for similar reasons as those who dropped out in wave 1. The resulting sample size for wave 3 was 462.
Paper and pencil surveys were conducted at the participants’ houses for wave 1 and wave 2. Due to the national visitation restrictions imposed due to COVID-19 during the time of data collection, paper and pencil surveys for wave 3 were conducted virtually through video call instead of physically at the participants’ houses. Participants were couriered a copy of the survey booklet and surveyors would call the participants, ask them for their responses and fill them up on the surveyor’s copy of the survey booklet. We obtained informed consent from mother and child assent from the child. Each family who participated in the study received a token of $60 Singapore dollar (approximately $40 USD) at wave 1, $80 Singapore dollar (approximately $60 USD) at wave 2 and $110 Singapore dollar (approximately $80 USD) at wave 3. This study included 1) 4 major ethnic groups: Chinese, Malay, Indian and Others; and 2) male and female children.
Measures
Economic Hardship Questionnaire
The Economic Hardship Questionnaire (EHQ) (Lempers et al., 1989) was administered to mothers at wave 1, wave 2 and wave 3 to assess perceived economic hardship experienced by the family. The EHQ is a 10-item questionnaire that focuses on changes in a household’s style of living. Participants answer questions using a 4-point Likert scale from 0 (never having to cut back due to financial concerns) to 3 (having had to cut back very often). Item scores are summed up and can range from 0 to 30. Higher scores reflect greater perceived economic hardship. The EHQ has demonstrated good internal consistency in the present study at wave 1 (Cronbach’s alpha = 0.81), wave 2 (Cronbach’s alpha = 0.84) and wave 3 (Cronbach’s alpha = 0.80).
Depression, Anxiety Stress Scale-21
The Depression Anxiety Stress Scale 21 (DASS-21) was administered to mothers at wave 3 to measure the mother’s emotional distress in three subcategories (Lovibond & Lovibond, 1995) of depression (e.g., loss of self-esteem/incentives and depressed mood), anxiety (e.g., fear and anticipation of negative events), and stress (e.g., persistent state of overarousal and low frustration tolerance). It was a self-report questionnaire with 21 items (seven items for each category) based on a four-point rating scale (ranging from “did not apply to me at all” = 0, to “applied to me very much or most of the time” = 3). To calculate comparable scores with full DASS, each seven-item scale was multiplied by two which ranges from 0 to 21. Higher scores indicate more psychological distress. The present study focused on the mother’s depression and anxiety. Clinical groups of depression and anxiety were determined by the severe and extremely severe band of scores (i.e., ≥ 21 for depression and ≥ 15 for anxiety (Lovibond & Lovibond, 1995)). Within the current study, the depression scale and anxiety scale demonstrated excellent reliability of 0.88 and 0.82 respectively at wave 3.
Child Behavior Checklist 6–18
The Child Behavior Checklist 6–18 (CBCL 6–18) was administered to mothers at wave 3 to assess the emotional and behavioural problems of the children (Achenbach & Rescorla, 2001). The CBCL contains 113 items that were rated on a 3-point scale: 0 (not true), 1 (somewhat or sometimes true), and 2 (very true or often true). The CBCL contains two empirically derived broadband scales and eight syndrome scales. The present study investigated depression and anxiety in children based on the withdrawn/depressed syndrome scale and the anxious/depressed syndrome scale respectively. T-scores for both the withdrawn/depressed and anxious/depressed scales were used for the current analysis, ranging from 50 to 100, where higher scores reflect more psychological distress. Clinical groups of depression and anxiety were determined by T-scores more than or equal to 70 on the withdrawn/depressed and anxious/depressed scales. Within the current study, the withdrawn/depressed scale and anxious/depressed scale demonstrated good reliability of 0.74 and 0.78 respectively at wave 3.
State Self-esteem Scale
The State Self-Esteem Scale (SSES) was administered to mothers at wave 3 to assess the self-esteem of mothers (Heatherton et al., 1991). The SSES is a 20-item Likert-type scale designed for measuring temporary changes in individual self-esteem based on a five-point rating scale (ranging from “Not at all” = 1, to “Extremely” = 5). Item scores are summed up and can range from 20 to 100. Higher scores reflect greater self-esteem. There are three self-esteem factors in the scale: Academic Performance, Social Evaluation, and Appearance. Within the current study, the SSES demonstrated excellent reliability of 0.84 at wave 3.
Rosenberg self-esteem scale
The Rosenberg Self-Esteem Scale was administered to children at wave 3 to assess the self-esteem of children (Rosenberg, 1965). The Rosenberg Self-Esteem Scale is a 10-item Likert-type scale designed for measuring temporary changes in individual self-esteem based on a four-point rating scale (ranging from “Strongly Disagree” = 0, to “Strongly Agree” = 3). Item scores are summed up and can range from 0 to 30. Higher scores reflect greater self-esteem. Within the current study, the Rosenberg Self-Esteem Scale demonstrated good reliability of 0.80 at wave 3.
Statistical Analysis
Latent Class Growth Analysis (LCGA) was used to identified distinct trajectories of perceived economic hardship in the family (latent classes) during the three waves of the study (Jung & Wickrama, 2008). The models were conducted using Mplus 8.5 which uses maximum likelihood estimation as default to handle data that are missing at random by using all available data. The time difference, in terms of the number of days between each wave of data collection for each participant was accounted for in the model. The number of classes was set to a single class in the initial model and follow up models were conducted with increasing the number of expected latent classes by one at a time to identify the model that best fit data.
The class assignment was used as the predictor variable in the consequent models. The mother’s and child’s depression and anxiety scores were dichotomized based on recommended cut-offs to form clinical groups and non-clinical groups. Covariate adjusted logistic regression models were used to identify whether the economic hardship trajectory classes were associated with the risk of clinical levels of depression and anxiety in mothers and children at wave 3. Logistic regression analyses were performed using SPSS 28.
Mediation analyses were used to examine whether the self-esteem of the mother or child at wave 3 was a potential link between the significant relations found between perceived economic hardships trajectories and clinical levels of depression and anxiety in mothers and children. Bootstrap mediation analysis with a multicategorical antecedent was applied through the SPSS PROCESS macro (Hayes, 2018) controlling for covariates. We utilized 10,000 bootstrap samples for estimation of the indirect effect. The indirect effect was statistically significant if the 95% bias-corrected confidence intervals (CIs) for the indirect effect did not include zero. Based on the recommendations of Zhao et al. (2010), the presence of mediation was determined by a significant indirect effect from the bootstrapping results.
Confounding Variables
This study considered variables that could potentially account for differences in the mental health of mothers and children. In the analyses involving the outcome variable of mother’s depression or anxiety (i.e., logistic regression models or mediation models): age of mother at wave 1 and mother’s ethnicity were included as common covariates. In the analysis involving the outcome variable of child’s depression or anxiety (i.e., logistic regression models or mediation models): age of child at wave 1, child’s ethnicity and child’s gender were included as common covariates.
Results
Identification of Trajectories of Economic Hardship
To determine the optimal number of latent growth classes for trajectory of economic hardship from wave 1 to wave 3, various Latent Class Growth Analysis (LCGA) models were estimated. Five hundred and eleven participants were involved in this analysis. The one-class, two-class, three-class and four-class models were compared to identify which model fit the data best. Table 1 presents the results of these analyses. The BIC values indicated that the three-class model fit the data the best as the BIC was lowest for this model. The LMR-LRT p-value was also significant, indicating that the three-class model fit the data better than the two-class model. Inspection of the growth parameters indicated that the three-class model yielded the most interpretable trajectories with reasonable class sizes. Furthermore, there was an increase in the entropy value from the two class to three class model (i.e., 0.54 to 0.61) suggesting that the three-class model had better classification than the two-class model. Lastly, the average predicted probabilities for class membership for the three classes ranged from 0.79 to 0.84.
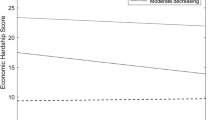
Figure 2 presents the fitted growth curve based on the estimated means for the three latent classes. Class one (Low stable) had a mean intercept of 9.36 and a slope of 0.001, Class two (High stable) had a mean intercept of 23.39 and a slope of -0.00Footnote 1 and Class three (Moderate decreasing) had a mean intercept of 17.49 and a slope of -0.01. One hundred and ninety-five families had low initial economic hardship that remained stable over time (class one), 21 families had high initial economic hardship that remained stable over time (class two) and 295 families had moderate initial levels of economic hardship that decreased over time (class three).

Trajectories of economic hardship across three waves
Descriptive Statistics
Out of the 511 participants involved in the analyses for the identification of economic hardship trajectories, 49 participants dropped out of the study between wave 1 and wave 3 and 11 multivariate outliers were found based on the mahalanobis distance (p < 0.001) of both mother’s and child’s depression, anxiety and self-esteem. Thus, the resulting sample size for the subsequent analyses was 451, with 169 participants in class one, 18 participants in class two and 264 participants in class three. Table 2 shows the descriptive statistics of the total sample and the participants in each class. Table 3 shows the correlation matrix of all the variables in the total sample. An examination of the bivariate correlations revealed significant correlations that were in the expected directions.
Economic Hardship Trajectories and Associations with Mother’s and Child’s Mental Health
Logistic regression models were utilized to investigate whether the economic hardship trajectory classes were associated with clinical levels of depression and anxiety in mothers and children at wave 3 (Table 4). Mothers who experienced high stable economic hardship had significantly greater odds (OR = 13.92, p = 0.002) of having clinical levels of depression compared to those who experienced low stable economic hardship. However, compared to mothers who experienced low stable economic hardship, mothers who experienced moderate decreasing hardship did not have significantly greater odds (OR = 3.24, p = 0.068) of having clinical levels of depression. In terms of anxiety, mothers who experienced high stable economic hardship had significantly greater odds (OR = 6.08, p = 0.004) of having clinical levels of anxiety as compared to mothers with low stable economic hardship. Mothers with moderate decreasing economic hardship had significantly greater odds (OR = 3.50, p < 0.001) of having clinical levels of anxiety as compared to mothers with low stable economic hardship.
For children, there were no significant differences in the odds of children having clinical levels of depression when the moderate decreasing and high stable groups were compared against the low stable group (p > 0.05). However, in terms of anxiety, children who experienced high stable levels of economic hardship as compared to those who experienced low stable economic hardship, had significantly greater odds (OR = 17.25, p = 0.025) of having clinical levels of anxiety. However, children who experienced moderate decreasing as compared to low stable levels of economic hardship did not have significantly greater odds (OR = 7.18, p = 0.060) of having clinical levels of anxiety.
Mediation Model: Self-esteem as a Potential Mediator Between Economic Hardship Trajectories and Mother’s and Child’s Mental Health
We sought in an exploratory analysis, to investigate if the significant relationships between economic hardship and mental health of mothers and children found previously would be mediated by the self-esteem of the mother or child at wave 3. We first investigated if the effects were mediated by the participant’s own self esteem (i.e., whether mother’s mental health was mediated by mother’s self-esteem or whether child’s mental health was mediated by child’s self-esteem). Following this, we investigated if the effects were mediated by the self-esteem of the other individual in the mother–child dyad (i.e., whether mother’s mental health was mediated by child’s self-esteem or whether child’s mental health was mediated by mother’s self-esteem).
Mediation by Own Self-Esteem
In mothers, the indirect effect of economic hardship trajectory class on mother’s depression through mother’s self-esteem was significant (b = 1.44, 95% CI [0.45, 3.02]; Fig. 3a) when the high stable class was compared with the low stable class indicating the presence of mediation. Compared to the low stable class, mothers from the high stable class had lower self-esteem (b = -10.78, p < 0.001). In addition, lower mother’s self-esteem was associated with a significantly greater odds of mother’s clinical depression (b = -0.13, OR = 0.88, p < 0.001). Mothers from the high stable class as compared to the low stable class experienced greater odds of clinical depression without controlling for mother’s self-esteem (b = 2.63, OR = 13.92, p = 0.002), although this relationship became non-significant when controlling for mother’s self-esteem (b = 1.60, OR = 4.96, p = 0.088). As the analysis comparing the moderate decreasing economic hardship with the low stable economic hardship on mother’s clinical levels of depression were not significant, the mediation results involving the comparison of these groups are not reported.

Mediation models of economic hardship trajectory group on mental health of mother or child, through self-esteem of mother or child (a) – (f)
In mothers, the indirect effect of economic hardship trajectory class on mother’s anxiety through mother’s self-esteem was significant (b = 0.81, 95% CI [0.25, 1.55]; Fig. 3b) when the high stable class was compared with the low stable class, indicating the presence of mediation. Compared to the low stable class, mothers from the high stable class had lower self-esteem (b = -10.78, p < 0.001). Lower mother’s self-esteem was associated with a greater odds of mother’s clinical anxiety (b = -0.08, OR = 0.93, p < 0.001). Mothers from the high stable class as compared to the low stable class experienced greater odds of clinical depression without controlling for mother’s self-esteem (b = 1.81, OR = 6.08, p = 0.004) although this relationship became non-significant when controlling for mother’s self-esteem (b = 1.07, OR = 2.91, p = 0.117).
The indirect effect of economic hardship trajectory class on mother’s anxiety through mother’s self-esteem was significant when the moderate decreasing class was compared to the low stable class (b = 0.22, 95% CI [0.05, 0.44]; Fig. 3b), indicating the presence of mediation. Compared to the low stable class, mothers from the moderate decreasing class had lower self-esteem (b = -2.96, p = 0.013). In addition, lower mother’s self-esteem was associated with a greater odds of mother’s clinical anxiety (b = -0.08, OR = 0.93, p < 0.001). Mothers from the moderate decreasing class as compared to the low stable class experienced greater odds of clinical depression without controlling for mother’s self-esteem (b = 1.25, OR = 3.50, p < 0.001) although this relationship became weaker when controlling for mother’s self-esteem (b = 1.04, OR = 2.83, p = 0.006).
In children, the indirect effect of economic hardship trajectory class on child’s anxiety through child’s self-esteem was non-significant (b = -0.20, 95% CI [-0.69, 0.10]; Fig. 3c) when the high stable class was compared with the low stable class, indicating that mediation was not present. As the analysis comparing the moderate decreasing economic hardship with the low stable economic hardship on child’s clinical levels of anxiety were not significant, the mediation results involving the comparison of these groups are not reported.
Mediation by Other’s Self-Esteem
The indirect effect of economic hardship trajectory class on mother’s depression through child’s self-esteem was non-significant (b = -0.10, 95% CI [-0.39, 0.09]; Fig. 3d) when the high stable class was compared with the low stable class, indicating that mediation was not present. As the analysis comparing the moderate decreasing economic hardship with the low stable economic hardship on mother’s clinical levels of depression were not significant, the mediation results are not reported.
Similarly, the indirect effect of economic hardship trajectory class on mother’s anxiety through child’s self-esteem was non-significant (b = -0.11, 95% CI [-0.35, 0.07]; Fig. 3e) when the high stable class was compared with the low stable class and the moderate decreasing class was compared to the low stable class (b = 0.03, 95% CI [-0.04, 0.12]; Fig. 3e), indicating that mediation was not present.
Lastly, the indirect effect of economic hardship trajectory class on child’s anxiety through mother’s self-esteem was significant (b = 0.53, 95% CI [0.05, 1.31]; Fig. 3f) when the high stable class was compared with the low stable class, indicating the presence of mediation. Compared to the low stable class, mothers from the high stable class had lower self-esteem (b = -10.64, p < 0.001). Lower mother’s self-esteem was associated with a greater odds of child’s clinical anxiety (b = -0.05, OR = 0.95, p = 0.017). Children from the high stable class as compared to the low stable class experienced greater odds of clinical anxiety without controlling for mother’s self-esteem (b = 2.85, OR = 17.25, p = 0.025) although this relationship became non-significant when controlling for mother’s self-esteem (b = 2.55, OR = 12.86, p = 0.053). As the analysis comparing the moderate decreasing economic hardship with the low stable economic hardship on child’s clinical levels of anxiety were not significant, the mediation results involving the comparison of these groups are not reported.
Discussion
In the present study, we delineated three distinct trajectories of perceived family economic hardship across 1.5 years. These were the low stable, high stable and moderate decreasing trajectories of economic hardship. Differences in the trajectory of economic hardship experienced was associated with mothers’ and children’s clinical levels of mental health issues. More specifically, mothers who experienced high stable economic hardship presented with a significantly greater likelihood of clinical levels of depression compared to the low stable group. Mothers who experienced high stable and moderate decreasing economic hardship were more likely to experienced clinical levels of anxiety than those with low stable economic hardship. Children who experienced high stable economic hardship had a greater likelihood of experiencing clinical levels of anxiety than those who experienced low stable economic hardship. In addition, all the mentioned relationships between economic hardship trajectories and mother’s and child’s mental health were mediated by the mother’s self-esteem but not child’s self-esteem.
Trajectories of Perceived Economic Hardship
The delineation of three distinct trajectories of perceived family economic hardship supports the importance of utilizing subjective measures of poverty. Previous studies have shown subjective poverty as a social determinant of mental outcomes above and beyond the effects of household income (Chung et al., 2018), and that subjective instead of objective measures of poverty are associated with mental health (Ahnquist & Wamala, 2011). The present study extends this line of inquiry, by showing that distinct trajectories of perceived family economic hardship exist within low-income families. Furthermore, these distinct trajectories of economic hardship were associated with mental health outcomes in mothers and children. Previous longitudinal studies using objective measures of poverty have also found differences in the likelihood of psychological distress in mothers (Wickham et al., 2017) and children (Pryor et al., 2019; Wickham et al., 2017) based on different trajectories of poverty. However, differences in the timing of measurements and sample make it difficult to make comparisons between the results of these studies and the present study. Future studies can focus on delineating the trajectories of both objective and subjective measures of poverty to see if they are comparable or have a similar effect on mental health outcomes in mothers and children.
Relationship Between Differences in Economic Hardship Trajectories and Mother’s and Child’s Mental Health
In the present study, high stable economic hardship as compared to low stable economic hardship was associated with a greater likelihood of mother’s depression, mother’s anxiety and child’s anxiety, while moderate economic hardship as compared to low stable economic hardship was only associated with a greater likelihood of mother’s anxiety. High stable economic hardship could represent sustained exposure to stress from managing uncertainty, income volatility and juggling multiple financial portfolios (Collins, 2009). The effect of this sustained stress could impact multiple domains of the mother’s mental health and the child’s mental health as compared to low stable economic hardship. In contrast, moderate decreasing hardship could represent a situation where the perceived economic situation of the family, while worse off than the low stable group, seems to be getting better over time. Moderate decreasing hardship could thus affect fewer domains of the mother’s mental health and not have an effect on child’s mental health, when compared to those experiencing low stable economic hardship.
Mother’s Self-esteem as the Mediator Between Economic Hardship Trajectories and Mother and Child’s Mental Health
The self-esteem of mothers mediated the significant relationships found between trajectories of economic hardship and the mental health of mothers and children. We found that mothers experiencing high stable or moderate decreasing economic hardship presented with lower self-esteem as compared to mothers with low stable economic hardship. A previous study found negative associations between economic hardship and self-esteem in low-income adults when investigated cross-sectionally (Frankham et al., 2020). According to the Stress Process Model (Pearlin et al., 1981), stressful experiences, such as economic hardship, can exert an influence on mental health outcomes indirectly through their influence on personal resources such as self-esteem. Several psychosocial mechanisms, such as social comparison and self-evaluation could explain the relations found in our study (Bem, 1967; Festinger, 1954). Based on the social comparison perspective (Festinger, 1954), self-esteem is a product of an individual’s comparison of himself/herself with others to make positive or negative self-evaluations. A mother experiencing a history of economic hardship may make comparisons with others in society who are more economically advantaged which erodes her sense of self-worth. Based on the self-evaluation perspective (Bem, 1967), self-esteem results from evaluating one’s success and failures. In a society that emphasizes achievement, economic failures could contribute to a negative view of self.
Consequently, lower mother’s self-esteem was associated with an increased likelihood of clinical levels of mother’s depression and anxiety as well as child’s anxiety. Mothers with low self-esteem could have an increased likelihood of depression based on their negative beliefs about themselves (Beck, 1967). Based on the vulnerability model, low self-esteem is conceptualized as a stable factor that predisposes the individual to experience depression (Klein et al., 2011). Mothers who assess their economic situation as poor, may have a negative view of themselves which increases their vulnerability to depression. In addition, mothers with low self-esteem experienced an increased likelihood of anxiety. According to terror management theory (Solomon et al., 1991), self-esteem serves as a gauge of an individual’s own sense of value in the world, which is maintained by living up to the standards of value defined by the individual’s cultural worldview. Mothers who compare themselves with others who are more economically advantaged and perceive themselves as not meeting the expectations of society may feel anxious.
Furthermore, the impact of lowered mother’s self-esteem on the child’s level of anxiety could be explained by the child’s interactions with his/her mother. Mothers with lower self-esteem could present with less positive parent–child interactions (Aunola et al., 1999). Parents with low self-esteem were found to adopt an authoritarian style of parenting, in contrast to parents with high self-esteem, who adopted an authoritative parenting style (MacPhee et al., 1996). Moreover, the authoritarian style of parenting, characterized by high demandingness and low responsiveness, was associated with greater child anxiety as compared to the authoritative style of parenting (Yaffe, 2018). As such, one possibility is that the relations between lower self-esteem of mothers and greater likelihood of clinical levels of children’s anxiety in our sample could be explained by the parenting style adopted by these mothers. There is also a lack of studies that found relations between parenting styles and child depression which could explain the lack of findings on the outcome of child’s depression in our study.
Interestingly, while a study by McLeod and Shanahan (1993) found that the effect of persistent poverty on internalizing problems in children was not explained by parenting behaviours, the study used objective measures of income to define poverty. The present study utilized subjective measures of economic hardship to define trajectories. Thus, the results showing that mother’s self-esteem mediates the relationship between economic hardship trajectories and child’s mental health could possibly be explained by parenting behaviour.
Pronounced Outcome of Mother’s Anxiety and Mediation by Mother’s Self-esteem
The relationship between economic hardship trajectories and the mental health of mothers appeared to have a more prominent effect on anxiety than depression. Garnefski and Kraaij (2018) in distinguishing the cognitive processes involved in depression and anxiety, found that depression was related to self-blame while anxiety was related to other-blame. Thus, one possible underlying explanation for the prominent results on mother’s anxiety as compared to depression is the greater effect of social comparison than self-evaluation of mothers. Mothers could be more impacted by the comparisons they make with other individuals in society who are more economically advantaged, than their own negative evaluations of their own economic situation.
The present findings emphasized mother’s self-esteem as the mediator of the relationship between economic hardship trajectories and mother’s and child’s mental health while no mediation effects were found with child’s self-esteem as the mediator. Indeed, previous studies support the notion that children, unlike adults, appear to be less distressed by social comparison from relative deprivation (Weisman et al., 1974). As such, given that mother’s self-esteem and not child’s self-esteem was found to be a mediator between economic hardship trajectories and mother’s and children’s mental health, the present results support a unidirectional model of parent–child relations (Kuczynski, 2003) within the context of trajectories of perceived economic hardship, self-esteem and mental health.
Implications
The present study highlights the importance of considering subjective indicators of poverty in working with low-income families. The presence of distinct trajectories of perceived family economic hardship suggests that even within the low-income context, families experience different patterns of economic hardship across time. Practitioners working with low-income families, in addition to finding out about their income levels, could ask them on their perceived experience of economic hardship over time. This could provide additional information on the family’s subjective experience of poverty, which could be indicative of the likelihood of mental health issues. Our finding that the high stable group presented with a greater likelihood of mother’s depression, mother’s anxiety and child’s anxiety as compared to the low stable group suggests the importance of targeted intervention for this small group of families (high stable group, n = 18, 4.00% of sample). Furthermore, the greater likelihood of mother’s anxiety in the moderate decreasing than low stable group suggests that this group of families (moderate decreasing group, n = 264, 58.54% of sample) would also benefit from intervention. In addition, given that the mother’s self-esteem was found to mediate the relationships between economic hardship trajectories and mental health outcomes of mothers and children, interventions focusing on the mother’s self-esteem could help to alleviate the impact of the course of economic hardship experienced on the mental health of the mothers and children. Some possible interventions to bolter self-esteem in mothers could include self-affirmation (Lannin et al., 2021), social identification with the community (Elahi et al., 2018) and the practice of gratitude (Lin, 2015), given their positive relationship with self-esteem.
At a societal level, the present research provides an understanding of how the experience of economic hardship over time is not homogenous but unique to each low-income family. Educating members of the public on the unique experiences of low-income families could provide them with a more comprehensive understanding of this group. Furthermore, given that the mother’s self-esteem explains the relationship between the trajectories of economic hardship and mental health of mothers and children, community-level action that consider how mother’s self-esteem could be impacted by comparison with others in society and the emphasis on economic success could be helpful for the mental health of both mothers and children from low-income families. For instance, community resilience prizes can be awarded to low-income families who find creative solutions to their challenges. In addition, media platforms can be utilized to showcase low-income families who made outstanding achievements against all odds.
Strengths and Limitations
The present study utilized a relatively large longitudinal sample of mother–child dyads (n = 511 at wave 1) to delineate the trajectories of perceived family economic hardship. A unique feature of this study is the delineation of distinct trajectories of family economic hardship based on subjective measures. In addition, measures on both mother and child’s self-esteem and mental health were utilized in the study. Nevertheless, our measure of family economic hardship and child’s mental health was based on the mother’s report. Future studies incorporating both mother’s and child’s perceptions of economic hardship or child’s perception of their mental health could yield interesting findings. In addition, while the Rosenberg Self Esteem Scale, which we utilized to measure child’s self-esteem, has been validated for use in adults but not children (Donnellan et al., 2015; Schmitt & Allik, 2005), studies have utilized it to measure self-esteem in children of prisoners from 7 to 17 years of age (Sharratt et al., 2014) and Asian children with a mean age of 12.93 years (Wu et al., 2017). Lastly, the inclusion of more waves of collected data could allow for more complex longitudinal analysis, where time and resources permit.
Conclusion
Three distinct trajectories of perceived family economic hardship were delineated over 1.5 years in a low-income sample. These were the low stable, high stable and moderate decreasing trajectories of economic hardship. We found that differences in the trajectory of economic hardship were associated with mother’s depression and anxiety as well as child’s anxiety. All of these relations were mediated by the mother’s self-esteem. These findings highlight the importance of enhancing mother’s self-esteem to reduce the impact of histories of economic hardship on mother and child’s mental health issues.
Data Availability
The datasets generated during and analysed during the current study are not publicly available due to the sensitive nature of the population.
Code availability
Code for the analyses conducted are not available.
Notes
Rounded off to 2 decimal places.
References
Achenbach, T. M., & Rescorla, L. (2001). Manual for the ASEBA School-age Forms & Profiles: An Integrated System of Multi-informant Assessment. ASEBA.
Ahnquist, J., & Wamala, S. P. (2011). Economic hardships in adulthood and mental health in Sweden. The Swedish National Public Health Survey 2009. BMC public health, 11(1), 788–788. https://doi.org/10.1186/1471-2458-11-788
Alegría, M., NeMoyer, A., Falgàs Bagué, I., Wang, Y., & Alvarez, K. (2018). Social Determinants of Mental Health: Where We Are and Where We Need to Go. Current Psychiatry Reports, 20(11), 95–95. https://doi.org/10.1007/s11920-018-0969-9
Assing-Murray, E., & Lebrun-Harris, L. (2020). Associations between parent-reported family economic hardship and mental health conditions in U.S. children. Journal of Children and Poverty, 26(2), 191–214. https://doi.org/10.1080/10796126.2020.1764188
Aunola, K., Nurmi, J.-E., Onatsu-Arvilommi, T., & Pulkkinen, L. (1999). The role of parents’ self-esteem, mastery-orientation and social background in their parenting styles. Scandinavian Journal of Psychology, 40(4), 307–317. https://doi.org/10.1111/1467-9450.404131
Beck, A. T. (1967). Depression: clinical, experimental, and theoretical aspects. Hoeber Medical Division, Harper & Row.
Bem, D. J. (1967). Self perception: An alternative interpretation of cognitive dissonance phenomena. Psychological Review, 74(3), 183–200. https://doi.org/10.1037/h0024835
Berk, L. E. (2017). Child development (9th ed.). Pearson.
Chung, R.Y.-N., Chung, G.K.-K., Gordon, D., Wong, S.Y.-S., Chan, D., Lau, M.K.-W., Tang, V.M.-Y., & Wong, H. (2018). Deprivation is associated with worse physical and mental health beyond income poverty: A population-based household survey among Chinese adults. Quality of Life Research, 27(8), 2127–2135. https://doi.org/10.1007/s11136-018-1863-y
Collins, D. (2009). Portfolios of the poor: How the world’s poor live on $2 a day. Princeton University Press.
Comeau, J., & Boyle, M. H. (2018). Patterns of poverty exposure and children’s trajectories of externalizing and internalizing behaviors. SSM - Population Health, 4, 86–94. https://doi.org/10.1016/j.ssmph.2017.11.012
Demaray, M. K., Malecki, C. K., Davidson, L. M., Hodgson, K. K., & Rebus, P. J. (2005). The relationship between social support and student adjustment: A longitudinal analysis. Psychology in the Schools, 42(7), 691–706. https://doi.org/10.1002/pits.20120
Dietz, L. J., Birmaher, B., Williamson, D. E., Silk, J. S., Dahl, R. E., Axelson, D. A., Ehmann, M., & Ryan, N. D. (2008). Mother-child interactions in depressed children and children at high risk and low risk for future depression. Journal of the American Academy of Child and Adolescent Psychiatry, 47(5), 574–582. https://doi.org/10.1097/CHI.0b013e3181676595
Donnellan, M. B., Trzesniewski, K. H., & Robins, R. W. (2015). Chapter 6 - Measures of Self-Esteem. In G. J. Boyle, D. H. Saklofske, & G. Matthews (Eds.), Measures of Personality and Social Psychological Constructs (pp. 131–157). Academic Press. https://doi.org/10.1016/B978-0-12-386915-9.00006-1
Elahi, A., McIntyre, J. C., Hampson, C., Bodycote, H. J., Sitko, K., White, R. G., & Bentall, R. P. (2018). Home Is Where You Hang Your Hat: Host Town Identity, But Not Hometown Identity, Protects Against Mental Health Symptoms Associated with Financial Stress. Journal of Social and Clinical Psychology, 37(3), 159–181. https://doi.org/10.1521/jscp.2018.37.3.159
Festinger, L. (1954). A Theory of Social Comparison Processes. Human Relations (new York), 7(2), 117–140. https://doi.org/10.1177/001872675400700202
Frankham, C., Richardson, T., & Maguire, N. (2020). Do Locus of Control, Self-esteem, Hope and Shame Mediate the Relationship Between Financial Hardship and Mental Health? Community Mental Health Journal, 56(3), 404–415. https://doi.org/10.1007/s10597-019-00467-9
Garnefski, N., & Kraaij, V. (2018). Specificity of relations between adolescents’ cognitive emotion regulation strategies and symptoms of depression and anxiety. Cognition and Emotion, 32(7), 1401–1408. https://doi.org/10.1080/02699931.2016.1232698
Goh, E. C. L., Chong, W. H., Mohanty, J., Law, E. C. N., Hsu, C.-Y.S., De Mol, J., & Kuczynski, L. (2019). Identifying Positive Adaptive Pathways in Low-Income Families in Singapore: Protocol for Sequential Longitudinal Mixed-Methods Design. JMIR Research Protocols, 8(2), e11629. https://doi.org/10.2196/11629
Hagenaars, A., & de Vos, K. (1988). The Definition and Measurement of Poverty. The Journal of Human Resources, 23(2), 211–221. https://doi.org/10.2307/145776
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: a regression-based approach (Second ed.). Guilford Press.
Heatherton, T. F., Heatherton, T. F., & Polivy, J. (1991). Development and validation of a scale for measuring state self-esteem. Journal of Personality and Social Psychology, 60(6), 895–910. https://doi.org/10.1037/0022-3514.60.6.895
Jung, T., & Wickrama, K. A. S. (2008). An Introduction to Latent Class Growth Analysis and Growth Mixture Modeling. Social and Personality Psychology Compass, 2(1), 302–317. https://doi.org/10.1111/j.1751-9004.2007.00054.x
Klein, D. N., Kotov, R., & Bufferd, S. J. (2011). Personality and depression: Explanatory models and review of the evidence. Annual Review of Clinical Psychology, 7(1), 269–295. https://doi.org/10.1146/annurev-clinpsy-032210-104540
Kuczynski, L. (2003). Beyond Bidirectionality: Bilateral Conceptual Frameworks for Understanding Dynamics in Parent-Child Relations. In K. Leon (Ed.), (pp. 3–24). SAGE Publications, Inc. https://doi.org/10.4135/9781452229645.n1
Lannin, D. G., Bible, J., Harris, P. R., Russell, L. T., Arellanes, J. A., & Yazedjian, A. (2021). How is spontaneous self-affirmation linked to self-esteem? A cross-lagged examination. Journal of Research in Personality, 92, 104091. https://doi.org/10.1016/j.jrp.2021.104091
Lee, J., & Allen, J. (2020). Young Adults’ Economic Weil-Being and Mental Health: The Mediation Model of Self-Esteem. The American journal of psychology, 329.
Lempers, J. D., Clark-Lempers, D., & Simons, R. L. (1989). Economic Hardship, Parenting, and Distress in Adolescence. Child Development, 60(1), 25–39. https://doi.org/10.1111/j.1467-8624.1989.tb02692.x
Lin, C.-C. (2015). Self-esteem mediates the relationship between dispositional gratitude and well-being. Personality and Individual Differences, 85, 145–148. https://doi.org/10.1016/j.paid.2015.04.045
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety Stress Scales. Psychology Foundation.
Luttmer, E. F. P. (2005). Neighbors as Negatives: Relative Earnings and Well-Being. The Quarterly Journal of Economics, 120(3), 963–1002. https://doi.org/10.1162/003355305774268255
MacPhee, D., Fritz, J., & Miller-Heyl, J. (1996). Ethnic Variations in Personal Social Networks and Parenting. Child Development, 67(6), 3278–3295. https://doi.org/10.1111/j.1467-8624.1996.tb01914.x
McLeod, J. D., & Shanahan, M. J. (1993). Poverty, Parenting, and Children’s Mental Health. American Sociological Review, 58(3), 351–366. https://doi.org/10.2307/2095905
Murali, V., & Oyebode, F. (2004). Poverty, social inequality and mental health. Advances in Psychiatric Treatment : The Royal College of Psychiatrists’ Journal of Continuing Professional Development, 10(3), 216–224. https://doi.org/10.1192/apt.10.3.216
Neppl, T. K., Senia, J. M., & Donnellan, M. B. (2016). Effects of Economic Hardship: Testing the Family Stress Model Over Time. Journal of Family Psychology, 30(1), 12–21. https://doi.org/10.1037/fam0000168
Pearlin, L. I., Menaghan, E. G., Lieberman, M. A., & Mullan, J. T. (1981). The Stress Process. Journal of Health and Social Behavior, 22(4), 337–356. https://doi.org/10.2307/2136676
Pryor, L., Strandberg-Larsen, K., Nybo Andersen, A.-M., Hulvej Rod, N., & Melchior, M. (2019). Trajectories of family poverty and children’s mental health: Results from the Danish National Birth Cohort. Social Science & Medicine, 1982(220), 371–378. https://doi.org/10.1016/j.socscimed.2018.10.023
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University Press.
Rosenberg, M., Schooler, C., Schoenbach, C., & Rosenberg, F. (1995). Global Self-Esteem and Specific Self-Esteem: Different Concepts Different Outcomes. American Sociological Review, 60(1), 141–156. https://doi.org/10.2307/2096350
Runciman, W. G. H. (1966). Relative deprivation and social justice: A study of attitudes to social inequality in twentieth-century England. University of California Press.
Sareen, J., Afifi, T. O., McMillan, K. A., & Asmundson, G. J. G. (2011). Relationship Between Household Income and Mental Disorders: Findings From a Population-Based Longitudinal Study. Archives of General Psychiatry, 68(4), 419–427. https://doi.org/10.1001/archgenpsychiatry.2011.15
Schmitt, D. P., & Allik, J. (2005). Simultaneous Administration of the Rosenberg Self-Esteem Scale in 53 Nations: Exploring the Universal and Culture-Specific Features of Global Self-Esteem. Journal of Personality and Social Psychology, 89(4), 623–642. https://doi.org/10.1037/0022-3514.89.4.623
Sharratt, K., Boduszek, D., Jones, A., & Gallagher, B. (2014). Original articleConstruct validity, dimensionality and factorial invariance of the Rosenberg Self-Esteem Scale: A bifactor modelling approach among children of prisoners [journal article]. Current Issues in Personality Psychology, 2(4), 228–236. https://doi.org/10.5114/cipp.2014.47447
Solomon, S., Greenberg, J., & Pyszczynski, T. (1991). A Terror Management Theory of Social Behavior: The Psychological Functions of Self-Esteem and Cultural Worldviews. In M. P. Zanna (Ed.), Advances in Experimental Social Psychology (Vol. 24, pp. 93–159). Academic Press. https://doi.org/10.1016/S0065-2601(08)60328-7
Tan, Z., Mun, E.-Y., Nguyen, U.-S.D.T., & Walters, S. T. (2021). Increases in social support co-occur with decreases in depressive symptoms and substance use problems among adults in permanent supportive housing: An 18-month longitudinal study. BMC Psychology, 9(1), 6–6. https://doi.org/10.1186/s40359-020-00507-0
Weisman, C. S., Rosenberg, M., & Simmons, R. G. (1974). Black and White Self-Esteem: The Urban School Child. In (Vol. 52, pp. 424–424): University of North Carolina Press.
Wickham, S., Whitehead, M., Taylor-Robinson, D., & Barr, B. (2017). The effect of a transition into poverty on child and maternal mental health: A longitudinal analysis of the UK Millennium Cohort Study. The Lancet. Public Health, 2(3), e141–e148. https://doi.org/10.1016/S2468-2667(17)30011-7
Wickrama, K. A. S., Surjadi, F. F., Lorenz, F. O., Conger, R. D., & O’Neal, C. W. (2012). Family Economic Hardship and Progression of Poor Mental Health in Middle-Aged Husbands and Wives. Family Relations, 61(2), 297–312. https://doi.org/10.1111/j.1741-3729.2011.00697.x
Wu, Y., Zuo, B., Wen, F., & Yan, L. (2017). Rosenberg Self-Esteem Scale: Method Effects, Factorial Structure and Scale Invariance Across Migrant Child and Urban Child Populations in China. Journal of Personality Assessment, 99(1), 83–93. https://doi.org/10.1080/00223891.2016.1217420
Yaffe, Y. (2018). Establishing Specific Links Between Parenting Styles and the S-Anxieties in Children: Separation, Social, and School. Journal of Family Issues, 39(5), 1419–1437. https://doi.org/10.1177/0192513X17710286
Zhang, X., Krishnakumar, A., & Narine, L. (2020). Family Economic Hardship and Child Outcomes: Test of Family Stress Model in the Chinese Context. Journal of Family Psychology, 34(8), 960–968. https://doi.org/10.1037/fam0000670
Zhao, X., Lynch, J. G., Chen, Q., & Deighton, J. (2010). Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. Journal of Consumer Research, 37(2), 197–206. https://doi.org/10.1086/651257
Acknowledgements
We thank Dr Mike Cheung (National University of Singapore), Dr Jungup Lee (National University of Singapore) and Dr Jiang Nan (National University of Singapore) for their statistical advice on the Latent Growth Curve Model analysis.
Funding
This research project is funded by the Singapore Ministry of Education Social Science Research Thematic Grant MOE2016-SSRTG-039 granted to the second author.
Author information
Authors and Affiliations
Contributions
D.J. Wen and E.C.L. Goh developed the study concept. Data collection was performed by D.J. Wen and E.C.L. Goh. D.J. Wen performed the data analysis. All of the authors contributed to the interpretation of results. D.J. Wen drafted the manuscript. All of the authors reviewed and edited several versions of the manuscript and provided critical revisions. All of the authors approved the final manuscript for submission.
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the University Institutional Review Board (IRB number: S-18–003) and is in line with the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
Mother and child dyads were surveyed in this study. We obtained informed consent from the mother and child assent from the child.
Consent for publication
Mothers provided informed consent to participate in the research study and for their data to be published.
Disclaimer
We are grateful to the Ministry of Social and Family Development (MSF) in facilitating the collection of data for this paper. MSF does not endorse the research project or its findings, methods or results in any way, and any views, findings or results arising from the research project in the publication or presentation are strictly the authors’ own.
Conflicts of interest/Competing interests
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wen, D.J., Goh, E.C.L. & De Mol, J. Trajectories of perceived economic hardship: Relations with mother’s and child’s mental health and the role of self-esteem. Curr Psychol 42, 21565–21577 (2023). https://doi.org/10.1007/s12144-022-03009-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03009-x