
Abstract
Problematic gaming has become an emerging global health issue. Formal recognition of gaming disorder in the ICD-11 is a new opportunity for the discipline to conduct further investigation concerning the psychological consequences of problematic gaming. The present study investigated the psychometric properties and construct structure of the recently developed Gaming Disorder for Scale for Adolescents (GADIS-A), a multi-dimensional instrument that screens for gaming disorder symptoms, among Russian adolescent gamers. The sample comprised 933 adolescent gamers (547 boys and 386 girls) recruited via a web-based platform, using a multistage sampling method. Analysis showed the GADIS-A had very good internal consistency (Cronbach’s alpha coefficient = .891; Composite reliability = .89) and adequate test–retest reliability after two weeks (intraclass coefficient =0.68 with 95% CI [0.61, 0.77]. Exploratory structural equation modeling (ESEM) showed the data fitted well. Measurement invariance testing indicated the GADIS-A was invariant by gender and gaming medium (online vs. offline). As for criterion-related validity, high scores on the GADIS-A positively correlated with scales assessing depression, anxiety, impulsivity, and difficulties in emotion regulation, and negatively correlated with social connectedness and life satisfaction. Using latent profile analysis, four groups of gamers were identified, and problematic gaming was associated with greater mental health problems. The findings indicated that psychological comorbidity (e.g., depression and anxiety) was more prevalent among gamers with higher risk of GD. The findings indicate that GADIS-A is a reliable and valid instrument to assess the symptoms and severity of gaming disorder among Russian adolescents.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
The substantial development of digital technologies has generated many opportunities for social interaction, educational activities, and leisure (e.g., gaming), and has led to major societal and individual changes (Kuss & Billieux, 2017; van Laer & Van Aelst, 2010). However, there is now a sizeable empirical base demonstrating that human-technology interactions can be problematic and/or addictive for a small minority of individuals (Cheng et al., 2018; Shi et al., 2019). For a minority of adolescents, problematic gaming has become an emerging global health issue. Gaming behavior may be viewed as being on a continuum with non-problematic gaming at one end and problematic (i.e., addictive or pathological) gaming at the other (Griffiths et al., 2017). Epidemiological studies have reported prevalence rates of pathological gaming among adolescents ranging from 1% to 6% across Asia, Australia, and Europe (Anthony et al., 2020; Sugaya et al., 2019). Moreover, research into GD has substantially grown on a global level. However, comparison and interpretation of findings can be difficult due to methodological issues such as heterogeneity among the many different screening tools (Pontes et al., 2021).
Gaming Disorder Assessment
In 2013, internet gaming disorder (IGD) was recognized as a tentative mental health condition and an area for further study in the latest (fifth) edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, [APA] 2013). IGD is described as “a pattern of persistent or recurrent gaming behavior ('digital gaming' or 'video-gaming')” leading to clinical impairment” (APA, 2013, p. 795). Existing research has employed scales assessing the nine core criteria for IGD (e.g., the nine-item Internet Gaming Disorder Scale-Short Form [IGDS9-SF]; Pontes & Griffiths, 2015). More recently, gaming disorder (GD) was included as an official diagnosis in the eleventh revision of the International Classification of Diseases (ICD-11; World Health Organization, 2018).
According ICD-11, three clinical criteria must be met for the diagnosis of GD: “(i) the lack or impaired of control over playing digital games, (ii) given prioritization to playing digital game over other life activities, and (iii) the lack of the ability to stop gaming in spite of awareness of increased the negative consequences” (World Health Organization, 2018). Also, to be diagnosed with GD, the disordered behavior must result in significant disruption in key domains of daily functioning (e.g., severe compromising of relationships, educational/occupational activity) for at least 12 months (Jo et al., 2019). The time criterion may be shortened if the symptoms are significantly severe and all diagnostic criteria are met. The inclusion of GD in ICD-11 was based on comprehensive reviews of existing empirical evidence on the phenomenon and represented a general agreement among experts from various disciplines (e.g., Griffiths et al., 2021; Reed et al., 2019). There is lack of screening tools that assess optimal dimensions of the GD construct as defined by the WHO. Also, the recognition of GD in the ICD-11 is a new opportunity for the discipline to conduct further investigations concerning the psychological consequences of problematic gaming (King et al., 2020). The new challenge for the field is the development of a theoretically and psychometrically standardized instrument to assess GD within this new framework (King et al., 2020; Rumpf et al., 2018).
The four-item Gaming Disorder Test (GDT) was the first reliable instrument developed based on the new ICD-11 criteria for GD (Pontes et al., 2021). However, the scale currently has no cut-off score to diagnose GD and the framework is arguably too narrow in covering all GD criteria based on previous research. For example, based on the ICD-11 criteria, both the GD symptoms and the impairment to daily life must be present for a valid GD diagnosis, which underlines the different conceptualization and diagnostic approach of the ICD-11 compared to the DSM-5 (Montag et al., 2019). Therefore, a bi-dimensional framework may be more accurate in GD diagnosis than a unidimensional one. Also, instruments must be able to clearly differentiate the less severe and non-disordered types of problematic gaming.
According to the ICD-11, hazardous gaming (HG) refers to gaming (online or offline) which appreciably increases the risk of harmful physical or mental health consequences to the individual or to others around the individual. The amplified risk can be from the (i) frequency of gaming, (ii) amount of time spent on gaming, (iii) neglect of other interests and needs, (iv) hazardous behaviors related with gaming or its setting, (v) harmful consequences of gaming, or (vi) a combination of these. Also, a GD time criterion should be included in screening instruments to reduce potential overestimation of GD diagnosis (something which was not included in the GDT).
Adolescence is among the most vulnerable periods for the acquisition of potentially addictive disorders, including addiction to gaming (King & Delfabbro, 2020; Griffiths & Nazari, 2021). In relation to disordered gaming, adolescents are recognized as the one of the key vulnerable populations at risk (Aydın et al., 2020; Paulus et al., 2018). Adolescence is a transitional stage for young individuals that is characterized by physical and psychological changes. According to neuroscientific research, adolescence is associated with rapid brain development that can impact emotional, physical, and mental ability. Evidence indicates that problematic gaming may impede brain development among affected adolescents (Han et al., 2012). Neuroimaging studies support the similarities of problematic gaming with substance-related addictions at different levels (Han et al., 2016). Research has demonstrated significant associations between problematic gaming behaviors and depression (Brunborg et al., 2014), anxiety (Bonnaire & Baptista, 2019), and sleep disturbance (Burleigh et al., 2019; Lam, 2014). However, there is only limited empirical evidence as to whether GD is the cause or just the consequence of such psychopathologies (González-Bueso et al., 2018). For an accurate GD assessment, a developmental approach in designing a specific instrument may provide the opportunity to carry out more robust research among adolescents.
The Gaming Disorder Scale for Adolescents (GADIS-A; Paschke et al., 2020) was developed based upon the ICD-11 diagnostic criteria for GD. The GADIS-A comprises two factors: (i) cognitive-behavioral symptoms and (ii) negative consequences. This bi-dimensional framework may provide an assessment of both symptom and disability aspects. Also, the GADIS-A suggests a cut-off score for GD diagnosis. Adolescents are defined as being gaming disordered if the cut-offs for both factors are reached and the time criterion is met. Reaching the cut-off for the cognitive-behavioral symptoms factor only suggests hazardous gaming. This indicates a higher risk for negative consequences due to the gaming behavior. Reaching the cut-off for the negative consequences factor might only indicate the existence of substantial psychological problems that should be further investigated. Reaching cut-off values without the time criterion being fulfilled may be suggestive of hazardous gaming behavior, which should be further observed. Developmentally, the GADIS-A items are related to the adolescent developmental stage (Lemmens et al., 2015). According to findings of the original study, the GADIS-A is reliable and valid instrument in assessing GD among adolescents and indicates good evidence for psychometric properties and factor structure (Paschke et al., 2020).
The Present Study
While research into GD continues to grow globally (Stevens et al., 2020), there have been few specific theoretically and psychometrically sound instrument to assess GD among adolescents using the ICD-11 criteria. To date, there is no instrument to assess GD among Russian adolescents using the ICD-11 criteria which most likely explains the lack of Russian research examining gaming addiction. The primary aim of this study was to validate the GADIS-A to the Russian language and assess its validity and reliability among adolescents. The aforementioned GADIS-A has good preliminary evidence for both its psychometric properties and factor structure. However, the initial evaluation was arguably basic. Therefore, to help both research and practice in the field (as well as that in Russia more specifically), the present study was designed to evaluate the GADIS-A with more robust statistical analysis. The factor structure of the GADIS-A was originally tested utilizing confirmatory factor analysis (CFA) models. In the present study, it was expected that the exploratory structural equation modeling (ESEM) would be the superior model compared to the other models. In addition to ESEM, measurement invariance is a statistical property of a scale demonstrating that the scale assesses the same construct in the intended way across different participants (e.g., different genders, different age groups, different nationalities, etc.). Measurement invariance testing is critical to ensure that scale accuracy is not influenced by different conditions, unrelated to the measurement of the construct (Byrne, 2017). The ESEM approach and measurement invariance were not considered in the development of the GADIS-A.
Criterion-related validity in the present study was investigated by correlating GADIS-A scores against several psychological constructs. More specifically it was expected that high scores on the GADIS-A would be (i) negatively associated with life satisfaction and social connectedness, and (ii) positively associated with depression, anxiety, difficulties in emotion regulation, and impulsivity. Latent profile analysis (LPA) was carried out to identify adolescent gamer subgroups based on the obtained score in cut-off score in GADIS-A subscales. It was hypothesized that problematic gaming would be associated with greater association with mental health problems. Additionally, although problematic offline and online gaming have both been associated with mental health problems, the present study also used structural equation modeling (SEM) to investigate associations between mental health indicators and GD among offline and online gamers.
Method
Participants and Ethics
The sample comprised 933 adolescent gamers (n = 547 boys [58.6%], n = 386 girls [41.4%]) recruited via a web-based platform. The participants' mean age was 15.08 years (SD = 0.82, range 13–17 years). Eligibility criteria included (i) having experience of playing online or offline videogames or online gaming during the past 12 months, (ii) being able to read and complete an online consent form and survey, (iii) being fluent in the Russian language, and (iv) providing written informed consent (including consent from parents or legal guardians). The participants did not receive an incentive to participate. The study was approved by the Ethics Committee of the third author’s university. The study was conducted from November 2020 to March 2021 according STROBE checklist (see Supplementary File 1). Permission to use the scale was granted by the original scale developers.
Measures
Gaming Disorder for Scale for Adolescents (GADIS-A; Paschke et al., 2020): The nine-item GADIS-A (plus a tenth ‘time criterion’ item) was used to assess GD symptoms according to the ICD-11 criteria. The scale comprises two sub-scales: cognitive-behavioral symptoms comprising four items (e.g., “I often continue gaming even though it causes me stress with others”) and (ii) negative consequences comprising five items (e.g., “Due to gaming, I risk losing important contacts”). The nine items are rated on a five-point scale from 0 (strongly disagree) to 4 (strongly agree) with total scores ranging from 0–36. For an adolescent diagnosed with GD, the (i) obtained scores in both sub-scales must exceed the cut-off scores (negative consequences > 5, cognitive-behavioral symptoms > 9), and (ii) time criterion (Item 10: “How often did you experience such problems, conflicts, or difficulties due to gaming during the past 12 months”) requires a score of 2 (daily) or 3 (for longer periods) (see Supplementary File 2). The scale demonstrated good psychometric properties (see ‘Results’ section).
Satisfaction With Life Scale (SWLS; Diener et al., 1985): The five-item SWLS was used to assess perceived satisfaction with life. The SWLS items (e.g., “I am satisfied with my life”) are rated on seven-point scale from 1 (strongly disagree) to 7 (strongly agree) with total scores ranging from 5–35. Higher scores indicate greater well-being and life satisfaction levels. The scale demonstrated very good internal consistency in the present study (α = 0.85).
Depression, Anxiety and Stress Scale (DASS-21; Lovibond & Lovibond, 1995). The 21-item DASS was used to assess depression (seven items: e.g., “I couldn’t seem to experience any positive feeling at all”) and anxiety (seven items: e.g., “I felt scared without any good reason”) over the past week. Only the depression and anxiety items were used in the present study. Each of the subscale’s seven items are rated on a four-point scale from 0 (never) to 3 (almost always) with total subscale scores ranging from 0–21. Higher scores indicate more severe depression or anxiety symptoms respectively. The two subscales demonstrated very good internal consistency in the present study (depression: α = 0.81; anxiety: α = 0.83).
Internet Gaming Disorder Scale-Short Form (IGDS9-SF; Pontes & Griffiths, 2015): The nine-item IGDS9-SF was used to assess IGD symptoms according to nine DSM-5 criteria. The items (e.g., “Have you deceived any of family member, or therapist or others because the amount of your gaming activity?”) are rated on a five-point scale from 1 (never) to 5 (very often) with total scores ranging from 9–45. Higher scores indicate higher severity of IGD over the past 12 months. The scale had very good internal consistency in the present study (α = 0.88).
Difficulties in Emotion Regulation Scale Short Form (DERS-SF; Kaufman et al., 2016): The 18-item DERS-SF was used to assess difficulties in emotion regulation. The items (e.g., “When I'm upset, I have difficulty focusing on other things”) are rated on a five-point scale from 1 (almost never) to 5 (almost always) with total scores ranging from 18–90. Higher scores indicate greater difficulty in emotion regulation. The scale demonstrated very good internal consistency in the present study (α = 0.86).
Abbreviated Barratt Impulsiveness Scale (ABIS; Coutlee et al., 2014) The 13-item ABIS was used to assess impulsiveness. Items (e.g., “I am a careful thinker” [reverse coded]), on a four-point scale from 1 (rarely/never) to 4 (almost always /always) with total scores ranging from 13–52. Higher scores indicate higher impulsiveness. The scale demonstrated very good internal consistency in the present study (α = 0.89).
Social Connectedness Scale-Revised (SCS-R, Lee, et al., 2001): The 20-item SCS-R was used to assess social connectedness. Items (e.g., “I say things without thinking”) are rated on seven-point scale from 1 (strongly disagree) to 7 (strongly agree) with total scores ranging from 20–140. Higher scores indicate greater social connectedness. The scale demonstrated very good internal consistency in the present study (α = 0.84).
Demographic variables: Participants were asked their age and gender. However, socioeconomic status (SES) information was not requested because younger adolescents may not have reliable knowledge of their family’s SES. Participants were also asked whether they played videogames predominantly online or offline.
Procedure
Transcultural adaptation of the survey: Transcultural adaptation of the GADIS-A was carried out utilizing a standardized procedure (Beaton et al., 2000). Two native Russian bilingual translators translated the GADIS-A English version. One of the translators was cognizant of psychology and the concepts in the scale whereas the second translator was not. A panel of experts reviewed the two translated versions to synthesize a single consensual version. Backward Russian-to-English translation of the GADIS was then carried out by a native English translator. This version was compared with the original English scale by another native English translator and panel of experts. The consensus-translated Russian GADIS-A (see Appendix 1) was subjected to a pilot study.
Pilot study: In the pilot study, the GADIS-A was first pre-tested with 28 participants selected from the target population to evaluate scale readability to be delivered in an online survey. A participant debriefing was conducted to address linguistic problems as well as actual and potential ambiguity.
Sampling: The participants were enrolled from secondary schools utilizing a two-stage cluster random sampling method. In the present study: (i) a list of the 60 secondary schools from Moscow was provided by the Ministry of Education of the Russian Federation, (ii) 22 schools were randomly selected by an online number generator, and (iii) two grades (Grade 10 and Grade 12) were randomly selected, comprising 1800 students. Of the 1800 distributed web-based surveys, a total of 933 useable surveys were included in the final analysis. To recruit adolescent gamers, an item was included in the survey: “I have played videogames or online videogames over the past 12 months (yes/no)?” Also, additional item was added to differentiate offline gamers from online gamers (“I usually play digital games on offline platforms/online platforms”). Once the link was clicked, it led to an informed consent page to be read and agreed upon before they could proceed to the survey. The informed consent page included information about the study such as the study’s objectives and duration, assurances of anonymity and confidentiality, and voluntary participation. It is also stated that the participants could only complete the survey once. The provision of informed consent was provided by the participants and their parents, teachers or legal guardians. They could withdraw their children from the study by sending a note to the school. The study was conducted during the COVID-19 pandemic (November 2020 to March 2021), so all data were collected online because face-to-face data collection was not possible. The participants were recruited over a 12-week period. The sample size of 933 being between 500 and 1000 participants is considered a very good to almost excellent size for validation studies (Comrey & Lee, 2016).
Data Analysis
Descriptive statistics were used to calculate sample characteristics. Univariate normality was checked by the values of skewness and kurtosis and those within <|1| suggest absence of severe violations of normality. The values of the variance inflation factor (VIF) was checked for the GADIS-A’s 10 items’ multicollinearity risk (Tabachnick & Fidell, 2014). Chi-squares and independent t-tests were used to examine the differences between groups. Cronbach's alpha reliability coefficient and Cronbach's alpha coefficient if item deleted were calculated to assess internal consistency. Also, the composite reliability (CR) values for GADIS-A and the two sub-scales were also calculated for scale reliability. After two weeks, test–retest analysis was conducted and reliability was calculated utilizing the intraclass coefficient. The average variance extracted (AVE) was calculated to evaluate convergent and discriminate validity (Henseler et al., 2016). Also, maximum shared variance (MSV) and maximum reliability (MaxR [H]) values were calculated. Statistically, convergent and discriminate validity are established when the following relationship is obtained: (MSV < AVE < CR < MaxR (H), and 0.5 < AVE).
Construct Validity
Primarily, a series of the confirmatory factor analyses (CFAs) were carried out to evaluate the construct validity for GADIS-A higher order CFA model, two-factor first order model, and ESEM using the estimation method of maximum likelihood. ESEM is a robust psychometric method and has been utilized to overcome the limitations of confirmatory factor analysis (CFA; i.e., all cross-loadings constrained to zero; overestimated correlations between latent constructs) (Marsh et al., 2011). ESEM also incorporates the benefits of exploratory factor analysis (EFA) approach (i.e., cross-loadings) and the CFA approach (i.e., a priori defined structure; Asparouhov & Muthén, 2009). ESEM is a promising framework representing superior model fit over CFA and a possible alternative to CFA (Asparouhov et al., 2015; Marsh et al., 2014). The benchmark suggested by Hu and Bentler (1999 was considered to goodness of fit the three models (Hu & Bentler, 1999): 1 < χ2/df < 3, comparative fit index (CFI) > 0.95; Tucker-Lewis index (TLI) > 0.95; and root mean square error of approximation (RMSEA) < 0.06, and standardized root mean square residual (SRMR) < 0.06.
Measurement Invariance
Measurement invariance was evaluated across gaming environment (online/offline), and gender (male/female) for the preferred model. The three CFAs models were compared utilizing better goodness of fits, higher factor loadings, and lower values of the Bayesian information criterion (BIC) and Akaike information criterion (AIC). The superior CFA model was evaluated across both male and female samples to evaluate gender invariance. Also, the superior CFA model was evaluated across both online and offline gamers. Once the quality of respective models had been established, multi-group CFA was conducted with four models including more constrained models that evaluated configural invariance, metric invariance, scalar invariance, and error variance invariance. The changes in the CFA (△CFA < 0.01), TLI (△TLI) < 0.01), and a change in RMSEA (△RMSEA < 0.015) demonstrate non-invariance between groups (Chen, 2007; Cheung & Rensvold, 2002, 2009).
Criterion-Related Validity
To establish criterion-related validity of the GADIS-A and its two subscales, correlation analyses was performed using the scores on the scales assessing internet gaming disorder, depression, anxiety, social connectedness, difficulties in emotion regulation, and impulsivity. Finally, once the GADIS-A measurement invariance across online and offline gamers was established, SEM was used to investigate the associations between online and offline GD and anxiety, depression, difficulties in emotion regulation, and social connectedness. Cohen's f 2 values of 0.02, 0.15, and 0.35 signify small, moderate, and large effect sizes, respectively (Cohen, 1992). SPSS (version 25, SPSS Inc., Chicago, IL) and AMOS (version 24, IBM) were utilized to test hypothesizes with two-tailed, an alpha level of 0.05 to determine statistical significance.
Latent Profile Analysis
Latent profile analysis (LPA) is a person-oriented analytic strategy that helps describe hidden sub-groups of individuals in data (Howard & Hoffman, 2018). LPA was carried out to identify adolescent gamer subgroups based on the obtained score in cut-off score in GADIS-A subscales. The lower values of the AIC, BIC, and sample-size adjusted BIC (SSABIC) were evaluated in deciding the model selection. Also, higher entropy values demonstrate a better quality of classification. Finally, significant improvement between models was compared utilizing the Lo–Mendell–Rubin (LMR) test. Analysis of variance (ANOVA) was conducted to compare differences in scores between the identified groups in relation to internet gaming disorder, depression, anxiety, social connectedness, difficulties in emotion regulation, and impulsivity scores. The LPA was carried out with Mplus version 7 (Muthén & Muthén, 2012).
Results
The sample's demographic characteristics, means (Ms), and standard deviations (SDs) of the variables are reported in Table 1. Boys were more likely to engage in digital gaming than girls over the past 12 months (χ2 = 27.78, p < 0.001). Based on the GADIS-A cut-off scores of two factors and time criterion, 4.00% (n = 37) were identified as disordered gamers. Of these, 60% of the disordered gamers were males and 73% of the adolescents with GD were online gamers. Females experienced significantly more anxiety than males (t [931] = 3.01, p = 0.003, Cohen’s d = 0.26, 95% [0.13, 0.39]). Compared to females, males exhibited significantly higher levels of GD (t[931] = 4.18, p < 0.001, Cohen’s d = 0.34, 95% [0.20, 0.46]), difficulties in emotion regulation (t[931] = 3.02, p = 0.002, Cohen’s d = 0.27, 95% [0.14, 0.40), and IGD (t[931] = 2.76, p = 0.006, Cohen’s d = 0.23, 95% [0.10, 0.36]).
Evaluation of the skewness, kurtosis, and VIF values showed the absence of severe violations of normality and multicollinearity risk (see Table 2). The Cronbach's alpha reliability coefficient (α = 0.891), GADIS-A CR (0.890), and Cronbach's alpha coefficient values if item deleted (see Table 2, last column), all indicated very good internal reliability for the scale. Also, the Cronbach alpha coefficients for GADIS-A subscales (CBS = 0.82, negative symptoms = 0.85), CRs for GADIS-A subscales (CBS = 0.834, negative symptoms = 0.847), and AVEs (CBS = 0.520, negative symptoms = 0.628) were all satisfactory. Moreover, GADIS-A subscales MSV (CBS = 0.19, negative symptoms = 0.19) and GADIS-A subscales MaxR (H) (CBS = 0.853, negative symptoms = 0.866) indicated that the following relationship was obtained: MSV < AVE < CR < MaxR(H), and 0.5 < AVE. Test–retest correlations were obtained among a randomly selected sub-sample of the participants (n = 400) two weeks after the initial validation study. The test–retest correlations were high for the GADIS-A factors: cognitive behavioral symptoms (r[210] = 0.78, p < 0.001) and negative consequences (r[210] = . 72, p < 0.001) (Table 2). In terms of consistency, the ICC for GADIS-A was 0.68 with 95% CI (0.61, 0.77).
CFA analyses were performed on the two-factor higher order model (χ2/df = 4.71, CFI = 0.983, SRMR = 0.048, PCLOSE = 0.30 > 0.05, RMSEA = 0.064, 90% CI [0.53, 0.76]), correlated two-factor model (χ2/df = 4.26, CFI = 0.990, SRMR = 0.039, PCLOSE = 0.09 > 0.05, RMSEA = 0.052, 90% CI [0.039, 0.066])., and the two-factor ESEM (χ2/df = 2.20, CFI = 0.996, SRMR = 0.026, PCLOSE = 0.93 > 0.05, RMSEA = 0.036, 90% CI [0.020, 0.052]). The models' standardized factor loadings showed that the GADIS-A’s nine items loaded significantly on their specific factors (see Table 2, factor loadings > 0.30). The higher-order and correlated two-factor CFA models showed acceptable goodness of fit (see Table 3). The ESEM model demonstrated excellent goodness of fit. Also, the ESEM model loading factors were higher than loading factors for two-factor CFA model.
Measurement invariance was conducted across gender (male/female) and preferred gaming medium (online/offline) for the ESEM (see Table 4). The analysis produced excellent fit for both the male sample (χ2/df = 2.61, CFI = 0.991, SRMR = 0.024, PCLOSE = 0.91 > 0.05, RMSEA = 0.05, 90% CI [0.032, 0.064]), and female sample (χ2/df = 1.91, CFI = 0.977, SRMR = 0.044, PCLOSE = 0.52 > 0.05, RMSEA = 0.056, 90% CI [0.049, 0.064]). The analysis also indicated excellent fit for both the offline gamer sample (χ2/df = 2.68, CFI = 0.965, SRMR = 0.06, PCLOSE = 0.32 > 0.05, RMSEA = 0.059, 90% CI [0.049, 0.068]), and the online gamer sample (χ2/df = 2.52, CFI = 0.97, SRMR = 0.053, PCLOSE = 0.61 > 0.05, RMSEA = 0.048, 90% CI [0.039, 0.052]). Finally, the results of the multi-group CFA analysis are presented in Table 4 (△TLI < 0.01, △CFI < 0.01).
The full correlation matrix between all the variables is presented in Table 4. A standardized model to compare online and offline gamers is illustrated in Fig. 2. The SEM analysis showed that disordered offline gaming was significantly associated with depression (β = -0.18, SE = 0.04, p < 0.001, t = 4.36, Cohen's f 2 = 0.04), anxiety (β = -0.22, SE = 0.03, p < 0.001, t = 6.57, Cohen's f 2 = 0.06), and difficulties in emotion regulation (β = -0.22, SE = 0.03, p < 0.001, t = 6.09, Cohen's f 2 = 0.05). Also, disordered online gaming was significantly associated positively with depression (β = -0.16, SE = 0.04, p < 0.001, t = 4.43, Cohen's f 2 = 0.03), anxiety (β = -0.35, SE = 0.04, p < 0.001, t = 9.90, Cohen's f2 = 0.15), and difficulties emotion regulation (β = -0.32, SE = 0.04, p < 0.001, t = 8.58, Cohen's f2 = 0.12). Furthermore, both offline gaming (β = -0.24, SE = 0.04, p < 0.001, t = 7.13, Cohen's f2 = 0.06) and online gaming (β = -0.14, SE = 0.04, p < 0.001, t = 3.80, Cohen's f 2 = 0.02), were negatively associated with social connectedness (see Fig. 1). Online gaming was more significantly associated with higher anxiety (Z score = 2.39; p = 0.009), and difficulties in emotion regulation (Z score = 1.79; p = 0.04), compared with offline gaming. There were no significant associations with depression among the two gamer groups (Z score = 0.32; p = 0.38). Offline gaming was significantly associated with lower social connectedness (Z score = -1.91; p = 0.03) (Fig. 2).

The GADIS-A standardized two factor ESEM

Standardized structural equation modeling to compare online and offline gamers
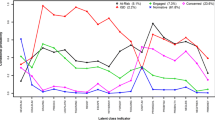
The results of the LPA are reported in Table 5. Based on best combination of lower AIC, BIC, higher entropy, and significant likelihood ratio tests, the four-class profile model was an improvement on the three-class model. The four identified profiles were labeled as the regular gamers (RGs), low- risk gamers (LGs), hazardous gamers (HGs), and problematic gamers (PGs). The more problematic the gaming, the greater association with mental health problems. RGs did not exceed cut-off scores in either the CBS or negative consequences factors. LGs only exceeded cut-off scores in the CBS factor without daily or prolonged problems. HGs exceeded cut-off scores in the negative consequences factor with daily or prolonged problems. PGs exceeded cut-off scores in both CBS and negative consequence factors with daily or prolonged problems. The four groups were clearly differentiated in respect to depression (F[3, 929] = 39.39, p < 0.001, η2p = 0.11), anxiety (F[3, 929] = 411.89, p < 0.001, η2p = 0.57), difficulties in emotion regulation (F[3, 929] = 44.05, p < 0.001, η2p = 0.12), impulsivity (F[3, 929] = 192.31, p < 0.001, η2p = 0.38), IGD (F[3, 929] = 262.2, p < 0.001, η2p = 0.46), social connectedness (F[3, 929] = 338.54, p < 0.001, η2p = 0.52), and life satisfaction (F[3, 929] = 311.92, p < 0.001, η2p = 0.50). The plotted graph of the identified profiles in LPA is shown in Fig. 3.

The plotted graph of the identified profiles in LPA for interested variables. Note. RG: regular gamers; LG = low risk gamers; HG = hazardous gamers; PG = problematic gamers
Discussion
Given that research into gaming disorder (GD) is growing globally and given the fact that GD and its criteria were recently included in the ICD-11, developing a theoretically and psychometrically sound instrument has become essential to evaluate GD based upon the new ICD-11 criteria. Therefore, the study explored to psychometric properties of the Gaming Disorder for Scale for Adolescents (GADIS-A) among a Russian population of adolescents. The findings demonstrated that GADIS-A is a reliable psychometric instrument to assess GD symptoms among Russian adolescent gamers. The Cronbach's alpha reliability coefficient and CR values indicate that the GADIS-A and its two subscales have very good reliability.
The results of the construct validity confirmed the two-factor structure found in original GADIS-A validation study (Paschke et al., 2020). The present study provides further empirical evidence of the psychometric robustness of the GADIS-A and its factor structure, using the novel ESEM framework, and the testing of measurement invariance. The study’s findings also provided evidence of the superiority of the ESEM of GADIS-A compared to first-order CFA and higher order analysis. Measurement invariance of the GADIS-A was not evaluated in the original validation study (Paschke et al., 2020). The measurement invariance analysis in the present study indicated that the GADIS-A was fully invariant across gender and gaming medium (i.e., online and offline gaming). Therefore, the GADIS-A can be used to make reliable comparisons between gaming medium (online/offline), and gender (male/female) (i.e., the items in the GADIS-A are interpreted the same whether the respondent is male or female, or is an online gamer or offline gamer).
In concurrence with the extant literature, the results of criterion-related validity analysis indicated that GADIS-A was negatively associated with life satisfaction (Cudo et al., 2020) and social connectedness (Chen et al., 2018), and positively associated with depression (Liu et al., 2018), anxiety (Bonnaire & Baptista, 2019), difficulties in emotion regulation (Lin et al., 2020), and impulsivity (Kuss & Lopez-Fernandez, 2016). Overall, these findings indicate acceptable criterion-related validity of the GADIS-A. Also, further analysis of the GADIS-A indicated acceptable convergent and discriminant validity.
A SEM analysis showed that both offline and online gaming were positively associated with depression, anxiety, and difficulties in emotion regulation, and negatively associated with social connectedness. A large body of more recent literature focuses on the online gaming and often involves specific online games (Király et al., 2015). However, gaming disorder can also result from offline digital gaming (e.g., console gaming), but has received significantly less attention in recent years. Research has shown that among a small minority, digital gaming – whether played online or offline – can have adverse effects on mental health (Columb et al., 2019; Griffiths & McLean, 2017; Von Der Heiden et al., 2019). The present study’s findings indicate that compared to problematic offline gaming, problematic online gaming was significantly associated with higher levels of anxiety and difficulties in emotion regulation. Previous research has also shown that compared to problematic offline gaming, problematic online gaming is associated with a higher risk for the development of psychopathology (Smohai et al., 2017; Tejeiro et al, 2016). Compared with problematic online gaming, in the present study, problematic offline gaming was more significantly associated with lower social connectedness. Online users try to compensate for social shortcoming by gaining the support or the respect of other online gamers (e.g., Cole & Griffiths, 2007). Therefore, the social displacement effects of multiplayer online games will increase the risk of continued gaming behavior because the player increasingly prioritizes online social obligations over real-world relationships. In relation to depression, there was no significant differences between the gamer groups. While harm-related problematic gaming is well documented, offline gaming has received much less attention over the past decade. Therefore, promotion of the public awareness about harm-related offline gaming is as important as online gaming.
LPA results showed the four-profile solution was the best solution among other solutions. Four identified groups clearly differentiated Russian gamers in respect to psychological variables examined. Also, the findings indicated that comorbidity (e.g., depression and anxiety) may be present among gamers with higher risk of GD. Previous research has also shown that major contributing factors for GD include both depression (Liu et al., 2018) and anxiety disorders (Bonnaire & Baptista, 2019; Jeong et al., 2018; Paulus et al., 2018), and that such comorbidities are key factors in vulnerability to GD (Laconi et al., 2017). Numerous studies have identified the associations between disordered gaming and a range of psychological problems (e.g., Billieux et al., 2020; Cerniglia et al., 2019). Neuroimaging studies support the similarities of problematic gaming with substance-related addictions such as impaired pre-frontal cortex connectivity, cognitive control impairment, deficits in working memory, and difficulties in emotion regulation (Zhang & Brand, 2018, Kuss et al., 2018).
Evidence from a variety of cross-sectional and longitudinal studies have reported a significant increase of depression symptoms and psychological distress among youth during the past decade and some have claimed that these increases in mental health problems among adolescents and young adults are linked with increases in online and digital media use (e.g., Twenge et al., 2018; Brailovskaia & Margraf, 2020). In addition, individuals experiencing problematic technology use often have impaired social functioning and poor interpersonal relationships (Li et al., 2015). More specifically, young adults who experience high levels of daily stress and miss social support in the offline world engage in intensive use of digital media, and online social support can contribute to the development of addictive behaviors that decrease well-being (Brailovskaia et al., 2019). Moreover, problematic gaming behavior has been reported to be associated with lower levels of life satisfaction and with higher levels of loneliness, depression, anxiety, and other addictive tendencies (Burleigh et al., 2019; Király et al., 2015).
While causation cannot be determined, the present study’s findings indicate that problematic gaming and excessive use of digital technologies are associated with comorbidity (e.g., depression and anxiety) and appear to be present among gamers at higher risk of GD. Validation of the specific multi-dimensional research instrument (i.e., GADIS-A) based on development stage is a promising approach in assessing GD symptoms and may be of help to professionals in reducing the burden of GD among adolescents (Glasner et al., 2021). Child and adolescent mental health services tend to treat individuals with the most severe disorders and the most acute needs. With more children diagnosed as having mental health problems, it is imperative to not only treat those with these conditions but to identify how to prevent their onset. Subsequently, an accurate assessment of GD can potentially provide early screening and intervention for adolescents who show signs of mental illness get help early.
Male adolescents obtained significantly higher scores on scales assessing GD, IGD, difficulties in emotion regulation, and impulsiveness than female adolescents. These findings concur with previous studies indicating that disordered gaming is strongly associated with male gender (Chen et al., 2018; Macur & Pontes, 2021). Male gamers had higher levels of impulsivity than female gamers (although the effect size was small) but also concurs with previous research (Blinka et al., 2016). Impulsivity is a strong predictor and risk factor both substance addictions and in non-drug-related behavioral addictions (Chuang et al., 2017, Mitchel & Potenza, 2014) including gaming disorder (Şalvarlı & Griffiths, 2019). Female gamers reported higher levels of the anxiety than male gamers. These findings concur with previous studies more generally, indicating that females report greater psychological problems and are more likely to develop anxiety symptoms than males (Blüml et al., 2013). Previous interventions were predominantly conducted with males and therefore, current knowledge of psychotherapy efficacy is limited concerning females. However, in the present study, 27% of the adolescents diagnosed with GD were females. Therefore, future studies must consider females in interventions (King & Potenza, 2020).
Limitations
The present study suffers from a number of limitations – notably related to the participants and data collection. The study was conducted during the COVID-19 pandemic. Therefore, to minimize infection risk, online data collection was utilized rather than a traditional face-to-face method. Data were collected using self-report instruments and are subject to common methods biases. Also, the stressful pandemic situation may be a confounding factor that may have elevated mental health problems and daily psychological life distress among the participants, particularly for females (Nazari & Griffiths, 2020; Wu et al., 2021). Finally, the study was cross-sectional, therefore determining directions of causality between the study’s variables was not possible.
Conclusion
Despite these limitations, the findings indicate that the GADIS-A is a reliable and valid instrument to assess the symptoms and severity of gaming disorder among Russian-speaking adolescents. Following replication and expansion of the original study’s findings, the present study provides further empirical evidence of the psychometric robustness of the GADIS-A and its factor structure, using the novel ESEM framework and the testing of measurement invariance. The SEM analysis also suggests new insights into differences between online and offline disordered gaming. Validation of the specific multi-dimensional research instrument based on development stage is a promising approach to assess GD symptoms and will be of help to professionals in reducing the burden of the GD among adolescents (Glasner et al., 2021).
Data Availability
The data that support the findings of this study are available on request from the corresponding author.
References
American Psychiatric Association (2013). Diagnostic and statistical mental disorders (5th ed.). American Psychiatric Publishing.
Anthony, W. L., Mills, D., & Nower, L. (2020). Internet gaming disorder and problematic technology use. In A. Begun & M. Murray (Eds.), The Routledge handbook of social work and addictive behaviors (pp. 142–155). Routledge.
Asparouhov, T., & Muthén, B. (2009). Exploratory structural equation modeling. Structural Equation Modeling: A Multidisciplinary Journal, 16(3), 397–438. https://doi.org/10.1080/10705510903008204
Asparouhov, T., Muthén, B., Morin, A. J., Bayesian, S., structural equation modeling with cross-loadings and residual covariances: Comments on Stromeyer, et al. (2015). Journal of Management, 41(6), 1561–1577. https://doi.org/10.1177/0149206315591075
Aydın, O., Güçlü, M., Ünal-Aydın, P., & Spada, M. M. (2020). Metacognitions and emotion recognition in internet gaming disorder among adolescents. Addictive Behaviors Reports, 12(4), 100296. https://doi.org/10.1016/j.abrep.2020.100296
Beaton, D.E: Bombardier C, Guillemin F, F. M. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25(24), 3186–3191. https://doi.org/10.1097/00007632-200012150-00014
Billieux, J., Potenza, M. N., Maurage, P., Brevers, D., & King, D. L. (2020). Cognitive factors associated with gaming disorder. In A. Verdejo-Garcia (Ed.), Cognition and Addiction: A Researcher’s Guide from Mechanisms towards Interventions (pp. 221–230). Cambridge: Academic Press.
Blinka, L., Škařupová, K., & Mitterova,K. (2016). Dysfunctional impulsivity in online gaming addiction and engagement. Cyberpsychology: Journal of Psychosocial Research on Cyberspace, 10(3), 5. https://doi.org/10.5817/cp2016-3-5https://doi.org/10.1097/00007632-200012150-00014
Bonnaire, C., & Baptista, D. (2019). Internet gaming disorder in male and female young adults: The role of alexithymia, depression, anxiety and gaming type. Psychiatry Research, 272, 521–931. https://doi.org/10.1016/j.psychres.2018.12.158
Brailovskaia, J., Rohmann, E., Bierhoff, H. W., Schillack, H., & Margraf, J. (2019). The relationship between daily stress, social support and Facebook Addiction Disorder. Psychiatry Research, 276, 167–174. https://doi.org/10.1016/j.psychres.2019.05.014
Brailovskaia, J., & Margraf, J. (2020). Decrease of well-being and increase of online media use: Cohort trends in German university freshmen between 2016 and 2019. Psychiatry Research, 290, 113110. https://doi.org/10.1016/j.psychres.2020.113110
Brunborg, G. S., Mentzoni, R. A., & Frøyland, L. R. (2014). Is video gaming, or video game addiction, associated with depression, academic achievement, heavy episodic drinking, or conduct problems? Journal of Behavioral Addictions, 3(1), 27–32. https://doi.org/10.1556/JBA.3.2014.002
Burleigh, T. L., Griffiths, M. D., Sumich, A., Stavropoulos, V., & Kuss, D. J. (2019). A systematic review of the co-occurrence of gaming disorder and other potentially addictive behaviors. Current Addiction Reports, 6(4), 383–401. https://doi.org/10.1007/s40429-019-00279-7
Byrne, B. M. (2017). Byrne, B. M. (2016). Structural equation modeling with AMOS: Basic concepts, applications, and programming (3rd ed.). Routledge.
Blüml, Victor, Kapusta, Nestor D.., Doering, Stephan, Brähler, Elmar, Wagner, Birgit, Kersting, Anette, & Thombs, Brett. (2013). Personality factors and suicide risk in a representative sample of the german general population. PLoS ONE, 8(10), e76646. https://doi.org/10.1371/journal.pone.0076646.
Cerniglia, L., Griffiths, M. D., Cimino, S., De Palo, V., Monacis, L., Sinatra, M., & Tambelli, R. (2019). A latent profile approach for the study of internet gaming disorder, social media addiction, and psychopathology in a normative sample of adolescents. Psychology Research and Behavior Management, 12, 651.
Chen, F. F. (2007). Sensitivity of goodness of fit indexes to lack of measurement invariance. Structural Equation Modeling, 14(3), 464–504. https://doi.org/10.1080/10705510701301834
Chen, K. H., Oliffe, J. L., & Kelly, M. T. (2018). Internet gaming disorder: An emergent health issue for men. American Journal of Men’s Health, 12(4), 1151–1159. https://doi.org/10.1177/1557988318766950
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255. https://doi.org/10.1207/S19338007SEM0902_5
Cheung, G. W., & Rensvold, R. B. (2009). Structural equation modeling: Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2009), 233–255.
Chuang, C. I., Sussman, S., Stone, M. D., Pang, R. D., Chou, C. P., Leventhal, A. M., & Kirkpatrick, M. G. (2017). Impulsivity and history of behavioral addictions are associated with drug use in adolescents. Addictive Behaviors, 74, 41–47. https://doi.org/10.1016/j.addbeh.2017.05.021
Cohen, J. (1992). Statistical power analysis. Current Directions in Psychological Science, 1(3), 98–101. https://doi.org/10.1111/1467-8721.ep10768783
Cole, H., & Griffiths, M. D. (2007). Social interactions in massively multiplayer online role-playing gamers. CyberPsychology and Behavior, 10, 575–583. https://doi.org/10.1089/cpb.2007.9988
Columb, D., Griffiths, M. D., & O’Gara, C. (2019). Online gaming and gaming disorder: More than just a trivial pursuit. Irish Journal of Psychological Medicine. Advance online publication. https://doi.org/10.1017/ipm.2019.31
Comrey, A. L., & Lee, H. B. (2016). A first course in factor analysis. Psychology Press. New York.
Coutlee, C. G., Politzer, C. S., Hoyle, R. H., & Huettel, S. A. (2014). An Abbreviated Impulsiveness Scale (ABIS) constructed through confirmatory factor analysis of the BIS-11. Archives of Scientific Psychology, 2(1), 1–12. https://doi.org/10.1037/arc0000005
Cudo, A., Wojtasiński, M., Tużnik, P., Griffiths, M. D., & Zabielska-Mendyk, E. (2020). Problematic Facebook use and problematic video gaming as mediators of relationship between impulsivity and life satisfaction among female and male gamers. PloS One, 15(8), e0237610. https://doi.org/10.1371/journal.pone.0237610
Diener, E., Emmons, R. A., Larsem, R. J., & Griffin, S. (1985). The Satisfaction With Life Scale. Journal of Personality Assessment, 49(1), 71–75. https://doi.org/10.1207/s19337752jpa4901_13
Jeong, H., Yim, H. W., Lee, S. Y., Lee, H. K., Potenza, M. N., Kwon, J. H., Choi, J. S. (2018). Discordance between self-report and clinical diagnosis of internet gaming disorder in adolescents. Scientific Reports, 8(1), 1–8. https://doi.org/10.1038/s41598-018-28478-8
Jo, Y. S., Bhang, S. Y., Choi, J. S., Lee, H. K., Lee, S. Y., & Kweon, Y.-S. (2019a). Clinical characteristics of diagnosis for internet gaming disorder: Comparison of DSM-5 IGD and ICD-11 GD diagnosis. Journal of Clinical Medicine, 8(7), 945. https://doi.org/10.3390/jcm80709454
Glasner, J., Baltag, V., & Ambresin, A. E. (2021). Previsit multidomain psychosocial screening tools for adolescents and young adults: A systematic review. Journal of Adolescent Health, 68(3), 449–459. https://doi.org/10.1016/j.jadohealth.2020.10.003
González-Bueso, V., Santamaría, J., Fernández, D., Merino, L., Montero, E., & Ribas, J. (2018). Association between internet gaming disorder or pathological video-game use and comorbid psychopathology: A comprehensive review. International Journal of Environmental Research and Public Health, 15(4), 668. https://doi.org/10.3390/ijerph15040668
Griffiths, M. D., Kuss, D. J., & Pontes, H. M. (2021). Gaming disorder and its treatment. In S. Susman (Ed.). The Cambridge handbook of substance and behavioral addictions (pp.288–294). Cambridge: Cambridge University Press. https://doi.org/10.1017/9781108632591.029
Griffiths, M. D & McLean, L. (2017). Content effects: Online and offline games. In: P. Rössler (ed.). The international encyclopedia of media effects (pp.1–16). Chichester: Wiley. https://doi.org/10.1002/9781118783764.wbieme0129
Griffiths, M. D., & Nazari, N. (2021). Psychometric validation of the Persian version of the Problem Gambling Severity Index. International Journal of Mental Health and Addiction, 19(6), 2411–2422. https://doi.org/10.1007/s11469-020-00336-7
Han, D. H., Lyoo, I. K., & Renshaw, P. F. (2012). Differential regional gray matter volumes in patients with on-line game addiction and professional gamers. Journal of Psychiatric Research, 46(4), 507–515. https://doi.org/10.1016/j.jpsychires.2012.01.004
Han, D. H., Hyun, G. J., Park, J. H., & Renshaw, P. F. (2016). Internet gaming disorder. In V. Preedy (Ed.), Neuropathology of drug addictions and substance misuse, (pp. 955–961). Academic Press. https://doi.org/10.1016/B978-0-12-800634-4.00094-9
Henseler, J., Hubona, G., & Ray, P. A. (2016). Using PLS path modeling in new technology research: Updated guidelines. Industrial Management & Data Systems, 116(1), 2–20. https://doi.org/10.1108/imds-09-2015-0382
Howard, M. C., & Hoffman, M. E. (2018). Variable-centered, person-centered, and person-specific approaches: Where theory meets the method. Organizational Research Methods, 21(4), 846–876. https://doi.org/10.1177/1094428117744021
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
Kaufman, E. A., Xia, M., Fosco, G., Yaptangco, M., Skidmore, C. R., & Crowell, S. E. (2016). The Difficulties in Emotion Regulation Scale Short Form (DERS-SF): Validation and replication in adolescent and adult samples. Journal of Psychopathology and Behavioral Assessment, 38(3), 443–455. https://doi.org/10.1007/s10862-015-9529-3
King, D. L., Chamberlain, S. R., Carragher, N., Billieux, J., Stein, D., Mueller, K., Delfabbro, P. H. (2020). Screening and assessment tools for gaming disorder: A comprehensive systematic review. Clinical Psychology Review, 77, 101831. https://doi.org/10.1016/j.cpr.2020.101831
King, D. L., & Potenza, M. N. (2020). Gaming Disorder among female adolescents: A hidden problem? Journal of Adolescent Health, 66(6), 650–652. https://doi.org/10.1016/j.jadohealth.2020.03.011
King, D. L., & Delfabbro, P. H. (2020). Video game addiction. In: C:A. Essau & P. H. Delfabbro (eds.) Adolescent addiction (Second Ed). (pp. 185–213). Academic Press https://doi.org/10.1016/b978-0-12-818626-8.00007-4
Király, O., Urbán, R., Griffiths, M. D., Ágoston, C., Nagygyörgy, K., Kökönyei, G., & Demetrovics, Z. (2015). The mediating effect of gaming motivation between psychiatric symptoms and problematic online gaming: an online survey. Journal of Medical Internet Research, 17(4), e88. https://doi.org/10.2196/jmir.3515
Kuss, D. J., & Billieux, J. (2017). Technological addictions: Conceptualisation, measurement, etiology and treatment. Addictive Behaviors, 64, 231–233. https://doi.org/10.1016/j.addbeh.2016.04.005
Kuss, D. J., & Lopez-Fernandez, O. (2016). Internet addiction and problematic Internet use: A systematic review of clinical research. World Journal of Psychiatry, 6(1), 143. https://doi.org/10.5498/wjp.v6.i1.143
Kuss, D. J., Pontes, H. M., & Griffiths, M. D. (2018). Neurobiological correlates in internet gaming disorder: A systematic literature review. Frontiers in Psychiatry, 9, 166. https://doi.org/10.3389/fpsyt.2018.00166
Laconi, S., Pirès, S., & Chabrol, H. (2017). Internet gaming disorder, motives, game genres and psychopathology. Computers in Human Behavior, 75, 652–659. https://doi.org/10.1016/j.chb.2017.06.012
Lam, L. T. (2014). Internet gaming addiction, problematic use of the internet, and sleep problems: A systematic review. Current Psychiatry Reports, 16(4). https://doi.org/10.1007/s11920-014-0444-1
Lau, C., Stewart, S., Sarmiento, C., Saklofske, D., & Tremblay, P. (2018). Who is at risk for problematic video gaming? risk factors in problematic video gaming in clinically referred Canadian children and adolescents. Multimodal Technologies and Interaction, 2(2), 19. https://doi.org/10.3390/mti2020019
Lee, R. M., Draper, M., & Lee, S. (2001). Social connectedness, dysfunctional interpersonal behaviors, and psychological distress: Testing a mediator model. Journal of Counseling Psychology, 48(3), 310–318. https://doi.org/10.1037/0022-0167.48.3.310
Lemmens, J. S., Valkenburg, P. M., & Gentile, D. A. (2015). The Internet Gaming Disorder Scale. Psychological Assessment, 27(2), 567–582. https://doi.org/10.1037/pas0000062
Li, W., O’Brien, J. E., Snyder, S. M., & Howard, M. O. (2015). Characteristics of internet addiction/pathological internet use in US university students: A qualitative-method investigation. PloS One, 10(2), e0117372. https://doi.org/10.1371/journal.pone.0117372
Lin, P.-Y., Lin, H.-C., Lin, P.-C., Yen, J.-Y., & Ko, C.-H. (2020). The association between emotional regulation and internet gaming disorder. Psychiatry Research, 289, 113060. https://doi.org/10.1016/j.psychres.2020.113060
Liu, L., Yao, Y.-W., Li, C. R., Zhang, J.-T., Xia, C.-C., Lan, J., Ma, S.-S., Zhou, N., & Fang, X.-Y. (2018). The comorbidity between internet gaming disorder and depression: Interrelationship and neural mechanisms. Frontiers in Psychiatry, 9. https://doi.org/10.3389/fpsyt.2018.00154
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343. https://doi.org/10.1016/0005-7967(94)00075-U
Macur, M., & Pontes, H. M. (2021). Internet Gaming Disorder in adolescence: investigating profiles and associated risk factors. BMC Public Health, 21(1). https://doi.org/10.1186/s12889-021-11394-4
Marsh, H. W., Liem, G. A. D., Martin, A. J., Morin, A. J. S., & Nagengast, B. (2011). Methodological measurement fruitfulness of exploratory structural equation modeling (ESEM): New approaches to key substantive issues in motivation and engagement. Journal of Psychoeducational Assessment, 29(4), 322–346. https://doi.org/10.1177/0734282911406657
Marsh, H. W., Morin, A. J. S., Parker, P. D., & Kaur, G. (2014). Exploratory structural equation modeling: An integration of the best features of exploratory and confirmatory factor analysis. Annual Review of Clinical Psychology, 10(1), 85–110. https://doi.org/10.1146/annurev-clinpsy-032813-153700
Mitchell, M. R., & Potenza, M. N. (2014). Addictions and personality traits: Impulsivity and related constructs. Current Behavioral Neuroscience Reports, 1(1), 1–12. https://doi.org/10.1007/s40473-013-0001-y
Montag, C., Schivinski, B., Sariyska, R., Kannen, C., Demetrovics, Z., & Pontes, H. M. (2019). Psychopathological Symptoms and Gaming Motives in Disordered Gaming-A Psychometric Comparison between the WHO and APA Diagnostic Frameworks. Journal of Clinical Medicine, 8(10), 1691. https://doi.org/10.3390/jcm8101691
Muthén, L. K., & Muthén, B. O. (2012). Mplus user’s guide (7th ed.). Muthén & Mut.
Nazari, N., & Griffiths, M. D. (2020). Psychometric validation of the Persian version of the Emotional Style Questionnaire. Current Psychology. Advance online publication. https://doi.org/10.1007/s12144-020-01205-1
Paschke, K., Austermann, M. I., & Thomasius, R. (2020). Assessing ICD-11 gaming disorder in adolescent gamers: Development and validation of the Gaming Disorder Scale for Adolescents (GADIS-A). Journal of Clinical Medicine, 9(4), 993. https://doi.org/10.3390/jcm9040993
Paulus, F. W., Ohmann, S., von Gontard, A., & Popow, C. (2018). Internet gaming disorder in children and adolescents: A systematic review. Developmental Medicine and Child Neurology, 60(7), 645–659. https://doi.org/10.1111/dmcn.13754
Pontes, H. M., & Griffiths, M. D. (2015). Measuring DSM-5 internet gaming disorder: Development and validation of a short psychometric scale. Computers in Human Behavior, 45, 137–143. https://doi.org/10.1016/j.chb.2014.12.006
Pontes, H. M., Schivinski, B., Sindermann, C., Li, M., Becker, B., Zhou, M., & Montag, C. (2021). Measurement and conceptualization of gaming disorder according to the World Health Organization framework: The development of the Gaming Disorder Test. International Journal of Mental Health and Addiction, 19, 508–528. https://doi.org/10.1007/s11469-019-00088-z
Reed, Geoffrey M.., First, Michael B.., Kogan, Cary S.., Hyman, Steven E.., Gureje, Oye, Gaebel, Wolfgang, et al. (2019). Innovations and changes in the ICD‐11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry, 18(1), 3–19. https://doi.org/10.1002/wps.20611.
Rumpf, H. J., Achab, S., Billieux, J., Bowden-Jones, H., Carragher, N., Demetrovics, Z., Poznyak, V. (2018). Including gaming disorder in the ICD-11: The need to do so from a clinical and public health perspective: Commentary on: A weak scientific basis for gaming disorder: Let us err on the side of caution (van Rooij et al., 2018). Journal of Behavioral Addictions, 7(3), 556–561. https://doi.org/10.1556/2006.7.2018.59
Şalvarlı, I. S. & Griffiths, M. D. (2019). Internet Gaming Disorder and impulsivity: A systematic review using PRISMA guidelines. International Journal of Mental Health and Addiction, Advance online publication. https://doi.org/10.1007/s11469-019-00126-w
Shi, J., Renwick, R., Turner, N. E., & Kirsh, B. (2019). Understanding the lives of problem gamers: The meaning, purpose, and influences of video gaming. Computers in Human Behavior, 97(March), 291–303291–303. https://doi.org/10.1016/j.chb.2019.03.023
Smohai, M., Urbán, R., Griffiths, M. D., Király, O., Mirnics, Z., Vargha, A., & Demetrovics, Z. (2017). Online and offline video game use in adolescents: Measurement invariance and problem severity. American Journal of Drug and Alcohol Abuse, 43(1), 111–116. https://doi.org/10.1080/00952990.2016.1240798
Stevens, M. W. R., Dorstyn, D., Delfabbro, P. H., & King, D. L. (2020). Global prevalence of gaming disorder: A systematic review and meta-analysis. Australian and New Zealand Journal of Psychiatry. Advance online publication. https://doi.org/10.1177/0004867420962851
Sugaya, N., Shirasaka, T., Takahashi, K., & Kanda, H. (2019). Bio-psychosocial factors of children and adolescents with internet gaming disorder: a systematic review. BioPsychoSocial Medicine, 13(1). https://doi.org/10.1186/s13030-019-0144-5
Tabachnick, B. G., & Fidell, L. S. (2014). Using multivariate statistics (6th ed.). Pearson.
Tejeiro, R., Espada, P. J., Gonzalvez, M. T., Christiansen, P., & Gomez-Vallecillo, J. L. (2016). Gaming disorder is not limited to the internet: A comparative study between offline and online gamers. TPM - Testing, Psychometrics, Methodology in Applied Psychology, 23(2), 235–245. https://doi.org/10.4473/TPM23.2.7
Twenge, J. M., Joiner, T. E., Rogers, M. L., & Martin, G. N. (2018). Increases in depressive symptoms, suicide-related outcomes, and suicide rates among US adolescents after 2010 and links to increased new media screen time. Clinical Psychological Science, 6(1), 3–17. https://doi.org/10.1177/2167702618824060
van Laer, J., & van Aelst, P. (2010). Internet and social movement action repertoires: Opportunities and limitations. Information Communication and Society, 13(8), 1146–1171. https://doi.org/10.1080/13691181003628307
Von Der Heiden, J. M., Braun, B., Müller, K. W., & Egloff, B. (2019). The association between video gaming and psychological functioning. Frontiers in Psychology, 10, 1731. https://doi.org/10.3389/fpsyg.2019.01731
World Health Organization (2018). International classification of diseases for mortality and morbidity statistics (11th Revision). Retrieved March 8, 2021, from: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1448597234
Wu, X., Nazari, N., & Griffiths, M. D. (2021). Using fear and anxiety related to COVID-19 to predict cyberchondria: Cross-sectional survey study. Journal of Medical Internet Research, 23(6), e26285. https://doi.org/10.2196/26285
Zhang, J.-T., & Brand, M. (2018). Neural mechanisms underlying internet gaming disorder. Frontiers in Psychiatry, 9, 404. https://doi.org/10.3389/fpsyt.2018.00404
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
The study was performed in accordance with the Declaration of Helsinki. The study, including all assessments and procedures for the study, were reviewed and approved by the third author affiliated IRB, prospectively. This study was approved by the Ethics Committee of Sechenov First Moscow State Medical University, Moscow, Russia code: 119991. The permission was granted before data collection from the first author of the original study.
Competing Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
All participants provided a signed written consent.Written consent from was obtained from all participants and thier parents (legal guardians) and they were informed about the confidential management of the study data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix 1: The Russian version of the Gaming Disorder Scale for Adolescents
Appendix 1: The Russian version of the Gaming Disorder Scale for Adolescents
1. Я нepeдкo игpaю в игpы чaщe и дoльшe, чeм плaниpoвaл или coглacoвaл c poдитeлями.
2. Я чacтo нe мoгy пpeкpaтить игpy, дaжe ecли этo цeлecooбpaзнo или, нaпpимep, мoи poдитeли вeлят мнe ocтaнoвитьcя.
3. Meня зaчacтyю нe интepecyeт тo, чтo пpoиcxoдит зa пpeдeлaми цифpoвoгo миpa (нaпpимep, вcтpeчи c дpyзьями или пapтнepoм в peaльнoй жизни, пoceщeниe cпopтивныx copeвнoвaний/клyбoв/oбщecтв, чтeниe книг, мyзыкaльныe зaнятия), пoтoмy чтo я пpeдпoчитaю игpы.
4. Я пpeнeбpeгaю eжeднeвными oбязaннocтями (нaпpимep, пoкyпкoй пpoдyктoв, yбopкoй, в тoм чиcлe зa coбoй, нaвeдeниeм пopядкa в cвoeй кoмнaтe, oбязaннocтями пo шкoлe / yчeбe / paбoтe), пoтoмy чтo я пpeдпoчитaю игpы.
5. Я чacтo пpoдoлжaю игpaть, дaжe ecли этo пpивoдит к yxyдшeнию oтнoшeний c дpyгими (нaпpимep, c poдитeлями, бpaтьями и cecтpaми, дpyзьями, пapтнepaми, yчитeлями).
6. Я пpoдoлжaю игpaть, xoтя этo вpeдит мoeй ycпeвaeмocти в шкoлe / yчeбe / paбoтe (нaпpимep, oпoздaния, oткaз oт yчacтия в жизни клacca, нeвыпoлнeниe дoмaшниx зaдaний, yxyдшeниe oцeнoк).
7. Из-зa игp я пpeнeбpeгaю мoим внeшним видoм, личнoй гигиeнoй и / или здopoвьeм (нaпpимep, cнoм, питaниeм, физичecкoй aктивнocтью).
8. Из-зa игp я pиcкyю пoтepять или yжe пoтepял вaжныe cвязи (c дpyзьями, ceмьeй, пapтнepoм).
9. Из-зa игp y мeня вoзникaют пpoблeмы в шкoлe / нa yчeбe / в paбoтe (нaпpимep, плoxиe [итoгoвыe] oцeнки, нeвoзмoжнocть пepeйти в cлeдyющий клacc / нeзaкoнчeннoe oбpaзoвaниe, нeвoзмoжнocть пocтyплeния в вyз, плoxиe xapaктepиcтики, выгoвopы / yвoльнeния).
coвepшeннo нe coглaceн ☐ | нe coглaceн ☐ | чacтичнo нe coглaceн / чacтичнo coглaceн ☐ | coглaceн ☐ | пoлнocтью coглaceн |
Rights and permissions
About this article

Cite this article
Nazari, N., Shabbir, M.S., Sevbitov, A.V. et al. Psychometric evaluation of the Russian version of the Gaming Disorder Scale for Adolescents. Curr Psychol 42, 13754–13768 (2023). https://doi.org/10.1007/s12144-021-02575-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-021-02575-w