
Abstract
Objective
To describe the clinical profile of interstitial lung disease in infancy.
Methods
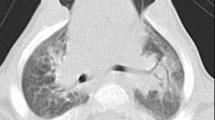
A retrospective analysis of cases diagnosed to have ILD was carried out in Kanchi Kamakoti CHILDS Trust hospital over a period of 2 yr. Infants aged 1 month to 1 yr of age were included if they had (1) respiratory symptoms (Cough, tachypnea or crepitations) for at least 1 month (2) diffuse infiltrates on chest radiography (3) Hypoxemia as defined by oxygen saturation less than 90% by pulse oximetry and (4) High Resolution Computed Tomography (HRCT) of the chest revealing findings of interstitial infiltrates of ground glass pattern. Their case records were analyzed for clinical data, treatment and follow up details.
Results
Of the 9 children, who were diagnosed to have ILD, 5 were boys and 4 were girls. The male: female ratio was 1.25: 1. The median age of onset of symptoms was 5 month. The common clinical features observed were tachypnea associated with chest indrawing (100%), cough (100%), hypoxia (100%), failure to thrive and fever (55%) each. The following radiographic patterns were observed in the chest skiagrams: reticulo-nodular pattern in 6(67%) and ground glass pattern in 3(33%). HRCT showed interstitial infiltrates in 6 (67%) and ground glass pattern in 3(33%). Evidence for cyto megalo virus (CMV) infection was detected in 5(56%), Adenovirus in 1 (11%) and Pneumocystis carinii (PCP) in 1(11%) infant. Open lung biopsy was performed in 2 infants, which detected CMV in 1 and PCP in the other. All children received oxygen therapy and systemic corticosteroids (oral/IV) in addition to specific therapy for infection and 3 of these infants succumbed to respiratory failure.
Conclusion
CMV Infection was the commonest cause of ILD in infancy in our study. However, the consequences on long term follow up in these infants need to be ascertained.
Similar content being viewed by others


References
James S. Hagood. Interstitial lung disease in children. Available from URL: http://www.emedicine.com/ped/topic.htm. Accessed December, 2, 2005.
Crystal RG, Bitterman PB, Rennard SI, Hance AJ, Koegh BA. Interstitial lung diseases of unknown cause. Disorders characterised by chronic malformation of the lower respiratory tract. N Engl J Med 1884; 310: 154–166.
Clement A. Task force on chronic interstitial lung disease in immunocompetant children. Eur Respir J 2004; 24: 686–697.
Fan LL, Kozinetz AC, Deterding RR and Brugman MS. Evaluation of a diagnostic approach to Pediatric Interstitial lung disease. Pediatr 1998; 101: 82–85.
Coren ME, Nicholson AG, Goldstraw P, Rosenthal M and Bush A. Open lung biopsy for diffuse Interstitial lung disease in children. Eur Respir J 1999; 14: 817–821.
Raghu G. Interstitial lung disease: a diagnostic approach. Are CT scan and Lung biopsy indicated in every patient? Am J Respir Crit Care Med 1995; 151: 909–914.
Coultas DB, Zumwalt RE, Black WC, Sobonya RE. The epidemology of interstitial lung disease. Am J Respir Crit Care Med 1994; 150: 967–972.
Michelle S. Howenstine. Interstitial lung diseases. In Richard E. Behrman, Robert M. Kliegman, Hal B. Jenson, eds. Nelson textbook of Pediatrics. 17 ed. Philadelphia; WB Saunders, 2004; 1451–1453.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Balasubramanian, S., Janakiraman, L., Ganesh, R. et al. Interstitial lung disease in infancy. Indian J Pediatr 74, 637–639 (2007). https://doi.org/10.1007/s12098-007-0113-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-007-0113-z