
Abstract
Purpose
We compared biochemical control and quality of life with intermittent (6 months) versus continuous (36 months) androgen deprivation therapy (ADT) in a non-inferiority randomized phase 3 trial in patients with biochemical failure (BF) after external beam radical radiotherapy (EBRT).
Materials and methods
Patients were stratified according to the Gleason score (GS) and were classified as low risk with a GS < 6 and 7 (3 + 4) and high risk with a GS of 7 (4 + 3) and >7. Patients were followed with PSA determinations and quality-of-life assessments (QLQ C-30 and QLQ PR-25) every 6 months for a period of 3 years. BF after radiation was defined as a PSA level of nadir +2 ng/ml. Disease progression (DP) after ADT was defined as PSA ≥4 ng/ml (BF) and/or metastases.
Results
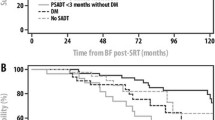
Seventy-seven patients were included in this multicenter phase 3 trial from 2005 to 2009. Thirty-eight and 39 patients were included in the intermittent and continuous groups, respectively. The median follow-up for both groups was 48 months (40–68). DP after ADT in the intermittent group was seen in three patients (distant metastases in one patient) versus 0 in the continuous group. The QLQ-C30 and QLQ PR-25 scores did not show any statistically difference between the two ADT groups.
Conclusions
No significant differences were seen in DP and QLQ between intermittent (6 months) and continuous (36 months) ADT in patients with BF after EBRT.
Similar content being viewed by others


References
Huggins C, Hodges CV. Studies on prostatic cancer. The effect of castration, of estrogen and of androgen injection on serum phosphatises in metastatic carcinoma of the prostate, 1941. J Urol. 2002;168:9–12.
Klotz LH, Herr HW, Morse MJ. Intermittent endocrine therapy for advanced prostate cancer. Cancer. 1986;58:2546–50.
Noble Rl. Hormonal control of growth and progession in tumors of NB rats and theory of action. Cancer Res. 1997;37:82–94.
Bruchowsky N, Renie PS, Coldman AJ, Godenberg SL, To M, Lawson D. Effects of androgen withdrawal on the stem cell composition of the Shionogi carcinoma. Cancer Res. 1990;50:2275–82.
Sanford NL, Searle JW, Kerr IJ. Succesive waves of apoptosis in the rat prostate alter repeated withdrawal of testosterona estimulation. Pathology. 1984;16:406–10.
Buyyounouski MK, Hanlon LH, Eisenberg DF, Horwitz EM, Feinberg SJ, Uzzo RG, et al. Defining biochemical failure alter radiotherapy with and without androgen deprivation for prostate cancer. Int J Radiat Oncol Biol Phys. 2005;63:1455–62.
Aaronson NK, Ahmedazi S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European organisation for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use international clinical trials in Oncology. J Nat Cancer Inst. 1993;85:365–76.
Van Andel G, Bottomley A, Fosså SD, Efficace F, Coen C, Guerif S, et al. An international field study of the EORTC QLQ-PR25: a questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur J Cancer. 2008;44:2418–24.
de Leval J, Boca P, Yousef E, Nicolas H, Jeukenne M, Seidel A. Intermittent versus continuous total androgen blockade in the treatment of patients with advanced hormone-naïve prostate cancer; results of a prospective randomized multicenter trial. Clini Prostate Cancer. 2002;1(3):163–71.
Klotz LH, Herr HW, Morse MJ, Whitmore WR. Intermittent endocrine therapy from advanced prostate cancer. Cancer. 1986;58:2546–50.
Tsai H-T, Penson DF, Makanbi K, Lynch JH, Van Den Eeden SK, Potosky R. Efficacy of intermittent androgen deprivation therapy vs conventional continuous androgen deprivation therapy for advanced prostate cancer: a meta-analysis. Urology. 2013;82:327–34.
Langenhuiojsen JF, Badhauser D, Scaaf B, Kiemeney ALM, Witjes A, Mulders PFA. Continuous vs intermittent androgen deprivation therapy for metastatic prostate cancer. Urol Oncol. 2013;31:549–56.
Mottet N, Van Dame J, Loulidi S, Russel C, Leifenberger A, Wolf JA. TAP 22 investigator group. Intermittent hormonal therapy in the treatment of metastatic prostate cancer: a randomized trial. BJU Int. 2012;9:1262–9.
Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, et al. Intermittent versus continous androgen deprivation in prostate cancer. N Engl J Med. 2013;368:1314–25.
Crook JM, O’Callagahm CJ, Duncan G, Dearnaley DP, HIgano CS, Horwitz EM. Intermittent androgen suppression for rising PSA level after radiotherapy. N Enl J Med. 2012;367:2262–9.
Schulman C, Cornel E, Matveev V, Tammela TL, Scraml J, Bensadoun H, et al. Intermittent versus continuous androgen deprivation therapy in patients with relapsing or locally advanced prostate cancer: a phase 3b randomised study (Iceland). Eur Urol. 2016;69:720–7.
Epstein JI, Allsbrook WC Jr, Amin MB, Egevad LL, ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol. 2005;29(9):1228–42.
Mahal BA. High PSA anxiety and low health literacy skills: drivers of early salvage ADT among men with biochemically recurrent prostate cancer after radiotherapy. Ann Oncol. 2015;26:1390–5.
Garcia-Albeniz X, Chanson JM, Paciore KA, Logan RW, Kenfield SA, Cooperberg MR, et al. Inmediate versus deferred initiation of androgen deprivation therapy with PSA-only relapse. An observational follow-up study. Eur J Cancer. 2015;51:817–24.
Duchesne G, Woo HH, Basset JK, Bowe SJ, D’Este K, Frydenberg M, et al. Timing of androgen-deprivation therapy in patients with prostate cancer with a rising PSA (TROG 03.06 and VCOG PR 01-03 (TOAD): a randomised, multicentre, non blinded, phase 3 trial). Lancet Oncol. 2016;17:727–37.
Acknowledgments
Ms Donna Pringle for English revision of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Investigational funding
Ipsen Pharma SA.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Casas, F., Henríquez, I., Bejar, A. et al. Intermittent versus continuous androgen deprivation therapy to biochemical recurrence after external beam radiotherapy: a phase 3 GICOR study. Clin Transl Oncol 19, 373–378 (2017). https://doi.org/10.1007/s12094-016-1538-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-016-1538-5