
Abstract
Chronic Myeloid Leukaemia (CML) is characterized by expression of the constitutively active Bcr-Abl tyrosine kinase. We have shown previously that the negative growth regulator, CCN3, is down-regulated as a result of Bcr-Abl kinase activity and that CCN3 has a reciprocal relationship of expression with BCR-ABL. We now show that CCN3 confers growth regulation in CML cells by causing growth inhibition and regaining sensitivity to the induction of apoptosis. The mode of CCN3 induced growth regulation was investigated in K562 CML cells using gene transfection and treatment with recombinant CCN3. Both strategies showed CCN3 regulated CML cell growth by reducing colony formation capacity, increasing apoptosis and reducing ERK phosphorylation. K562 cells stably transfected to express CCN3 showed enhanced apoptosis in response to treatment with the tyrosine kinase inhibitor, imatinib. Whilst CCN3 expression was low or undetectable in CML stem cells, primary CD34+ CML progenitors were responsive to treatment with recombinant CCN3. This study shows that CCN3 is an important growth regulator in haematopoiesis, abrogation of CCN3 expression enhances BCR-ABL dependent leukaemogenesis. CCN3 restores growth regulation, regains sensitivity to the induction of apoptosis and enhances imatinib cell kill in CML cells. CCN3 may provide an additional therapeutic strategy in the management of CML.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic Myeloid Leukaemia (CML), a haematopoietic stem cell disorder, is characterised by the expression of the chimaeric bcr-abl fusion gene (or Philadelphia chromosome, Ph+) formed from a reciprocal translocation between the bcr and abl genes on chromosomes 9 and 22 (Nowell and Hungerford 1960; Rowley 1973). The fusion gene encodes a constitutively active Bcr-Abl protein tyrosine kinase and expression culminates in alterations of cell proliferation, differentiation and resistance to the induction of apoptosis (Deininger et al. 2000; Jorgensen and Holyoake 2001). Expansion of the leukaemic clone presents as an accumulation of immature haematopoietic progenitor cells in the bone marrow (BM) and raised levels of myeloid cells in the peripheral blood (PB) (Clarkson et al. 1997; Wong and Witte 2001). CML is regarded as a triphasic disease; an indolent chronic phase of variable duration precedes progression to an accelerated phase leading on to the more severe blast crisis. The development of tyrosine kinase inhibitors (TKIs) has revolutionised the treatment of CML. Imatinib (Glivec, Gleevec), is now the gold standard and first line treatment for CML (Deininger and Holyoake 2005). Imatinib has been effective in inducing haematopoietic response in most cases and complete cytogenetic responses have been observed for 80-95% patients with chronic phase disease and 25-37% patients with advanced disease (accelerated and blast crisis) (Kumar 2006). Imatinib and its derivatives suppress but do not fully eradicate the leukaemic clone (Deininger and Holyoake 2005) and a proportion of patients remain unresponsive. An increasing number of patients are developing resistance to TKIs and it is clear that new treatment strategies are required.
We have previously identified down regulation of the negative growth regulator, CCN3, using DNA microarray analysis for a murine stem cell CML model to identify altered gene expression caused by the initial effects of Bcr-Abl kinase activity (McCallum et al. 2006). CCN3 is a member of the CCN family of growth regulatory proteins and roles for the CCN proteins are clearly established in fundamental biological processes such as cell proliferation, attachment, migration, differentiation, wound healing, angiogenesis and tumorigenesis (Perbal 2001). CCN proteins are multi-modular mosaic proteins containing four conserved modules which are present in other unrelated extracellular proteins. CCN3 comprises five distinct structural domains, a secretory peptide (SP) followed by the 4 conserved modules; insulin–like growth factor binding protein (IGFBP), Von Willebrand type C repeat (VWC), thrombospondin type I domain (TSP-1) and a cysteine knot carboxyl terminal (CT). CCN3 is mostly associated with exerting negative growth regulation. CCN3 was first isolated in a nephroblastoma model of Wilms’s tumour where expression was associated with a differentiated phenotype and anti-proliferative activity (Chevalier et al. 1998). Although CCN3 was able to reduce the growth rate of Ewings sarcoma transfectants ex vivo (Scotlandi et al. 2003), CCN3 expression was associated with poor prognosis and shown to increase cell motility resulting in enhanced metastatic potential (Benini et al. 2005; Manara et al. 2002). Increased levels of CCN3 expression have been correlated with reduced tumorigenicity and low metastatic potential in glioblastomas (Li et al. 1996) and an inverse relationship between CCN3 expression and tumour grade has been established for neuroblastoma and echondroma (Perbal 2001). CCN3 expression in conjunction with connexin-43 impaired human choriocarcinoma cell ability to induce tumour growth in vitro (Gellhaus et al. 2003). CCN3 is most commonly associated with negative growth regulation; reduced proliferation, cell differentiation and involvement in cell adhesion (Planque and Perbal 2003).
We have previously shown that CCN3 expression is low or absent in CML bone marrow (BM) mononuclear cells and expression increases to levels comparable with normal bone marrow (NBM) upon treatment with Imatinib (McCallum et al. 2006). This finding was also specific to the CD34+ progenitor cell population responsible for clonal expansion. In this study, we have used the human CML cell line (K562) to further investigate the mode of CCN3 induced growth regulation. We have evaluated the use of recombinant CCN3 (rCcn3) as an agent, alone and in combination with imatinib and then assessed primary human CML stem cell response to rCcn3.
Materials and methods
Cell lines
K562 cells were obtained from Deutsche Sammlung von Mikrorganismen und Zellkulturen (DSMZ, GmbH, Braunschweig, Germany) and HL-60 cells were obtained from the European Collection of Cell Cultures (ECACC, Salisbury, UK). All cell lines were maintained in RPMI-1640 medium supplemented with 10% fetal calf serum (Gibco BRL, Paisley, UK) cultured at 37°C in a humidified atmosphere (5% CO2 in air). Cells were subcultured twice weekly to maintain a log phase culture.
Primary CML samples and normal controls
Bone marrow aspirate samples and peripheral blood were obtained with informed consent from normal bone marrow donors and CML patients at diagnosis. All human samples were obtained with ethical approval from the local ethics review committee and those involved gave their informed consent for participation in accordance with the Declaration of Helsinki. Samples were collected in RPMI-1640 supplemented with 10% fetal calf serum and containing 100 IU preservative free heparin (Leo Laboratories Ltd, Princes Risborough, UK). Mononuclear and neutrophil cells were separated over Ficoll-Hypaque (Pharmacia Biotech, Uppsala, Sweden) using standard procedures (English and Andersen 1974). CD34 positive cells were prepared using the MACS Direct CD34 Progenitor Cell Isolation kit (Miltenyi Biotech Ltd, Bisley, UK).
CCN3 transfection of K562 cells
K562 cells were nucleofected following the manufacturer’s instructions using the Cell Line Nucleofector kit V, program T-16 (Amaxa, GmbH, Cologne, Germany) and transfected with 5 μg of either vector (pCb6+; Invitrogen) or vector containing CCN3 sequence. Transfection was performed in triplicate and the functional consequences of CCN3 expression were evaluated 24 hours after transfection (mean transfected cells, 97.9% ± 0.4%). Protein was extracted and Western blotting performed to confirm CCN3 expression. To obtain cells stably expressing CCN3, K562 cells were nucleofected (as above) and stable transfectants were selected in G418 (Invitrogen) at a concentration of 800 µg/ml. Cells transfected with the empty vector pCB6+ were used as a control.
Treating K562 cells with recombinant CCN3 or imatinib
K562 cells (1x106) were treated with recombinant CCN3 (rCcn3; Peprotech EC, London, U.K.) in vitro and cultured at 37°C in a humidified atmosphere (5% CO2 in air) for 24 and 48 h. After 24 h, cells were transferred to methyl cellulose culture (see below) and protein lysates were prepared (as described in Western Blotting). After 48 h, cells were fixed and prepared for flow cytometric analysis (as described in Flow cytometry). K562 cells (1 × 106) were treated with imatinib (1 µM and 5 µM) for 96 h. Cells were fixed and prepared for flow cytometric analysis (as described in Flow cytometry).
Evaluation of clonogenic capacity
Cells (1 × 104) were plated in triplicate in methyl cellulose (Miltenyi Biotech, U.K.) and incubated at 37°C in a humidified atmosphere (5% CO2 in air) for 7 days. Colonies were counted using an inverted microscope (Olympus model 214034; Olympus, Tokyo, Japan; magnification×40).
Western blot analysis
Protein was extracted from cells by suspending in RIPA buffer (1× PBS, 1% Nonidet NP-40, 0.1% SDS) containing a cocktail of protease inhibitors (Complete Mini Cocktail, Roche Diagnostics Ltd, Lewes, UK) at a concentration of 107 cells / ml and lysing for 10 minutes on ice. Samples were sonicated for 10 seconds to ensure complete lysis, centrifuged at 10,000 g at 4°C for 10 min and the supernatant removed for analysis. Total protein content was determined by the Bradford protein method using the BCA protein assay kit (Pierce, Cramlington, UK). Protein (15 μg) was loaded onto a pre-cast Bis-Tris polyacrylamide gel (10%) using the Novex mini gel system (Invitrogen, Paisley, UK) and subsequently transferred to a PVDF membrane. CCN3 expression was detected using an antibody raised against the C terminal of CCN3 22. Immunoblots were visualised by enhanced chemiluminescence (Supersignal West Pico and Supersignal West Dura substrates, Pierce).
Antibodies used in study
The K19M and NH5 antibodies were raised against the carboxyl terminal of CCN3 and were kindly provided by B.Perbal. Both antibodies were diluted 1/1,000 in Western Breeze Blocker Diluent (Invitrogen, Paisley, U.K.) and used in the Western blotting procedure. Total ERK1/2 and phosphorylated ERK1/2 were detected using the p44/42 MAP kinase antibody (1/1,000, Cat#9102; Cell Signaling Technology, Boston, MA, USA) and Phospho p44/42 MAP kinase antibody (1/2,000, Cat#9106; Cell Signaling Technology, USA) respectively. Anti-cleaved Caspase-3 antibody (Cat#96648; Cell Signaling Technology, USA) was used at a dilution of 1/1,000. Equivalent protein loading was controlled by monitoring actin expression using an anti-actin antibody (Cat#4968; Cell Signalling Technologies, USA).
Flow cytometry
Cells (5 × 105) were fixed in 70% ethanol for flow cytometric analysis of cell cycle status. Fixed cells were resuspended in PBS and incubated in RNase A (100 mg/mL, Qiagen) and propidium iodide (40 mg/mL, Calbiochem) for 30 minutes at 37°C. Samples were analyzed on a Coulter Epics Elite Cell Sorter (Beckman Coulter, High Wycombe, United Kingdom). Data were collected on the basis of peak signal versus integral signal to exclude doublets. Analysis was performed on 20,000 events using winMDI software (http://facs.scripps.edu/software.html) and data were generated and then ranked from a common gate in the subG0 area.
Real-time PCR analysis of BCR-ABL and CCN3 expression
RQ-PCR was performed with an ABI PRISM 7500 Sequence Detector which exploits TaqMan probe based chemistry (Applied Biosystems, Foster City, CA). The 5′ reporter used was 6-carboxyfluorescein (FAM) and the 3’ quencher was 6-carboxy-tetramethylrhodamine (TAMRA). Primers and probes for CCN3 were designed against GenBank published sequences in association with Primer Express (Applied Biosystems). Primer and probe sets for BCR-ABL were used as recommended by the Europe Against Cancer protocol (Beillard et al. 2003; Gabert et al. 2003). The amplification reactions (12.5 μL) contained 59 ng cDNA equivalents (or control), 1×Taqman universal PCR master mix, final concentrations of 5 mM MgCl2, 0.2 mM deoxyadenosine deoxycytosine deoxyguanosine triphosphate (dATP/ dCTP/ dGTP), 0.4 deoxyuridine triphosphate ( dUTP), 0.125 U AmpliTaq Gold, 2 μM primers (forward and reverse) and 200 nM TaqMan probe. Amplifications were performed following an initial 2-minute incubation at 50°C to allow uracil-N-glycosylase (UNG) to destroy any contaminating RNA, followed by treatment at 95°C for 10 min to inactivate the UNG enzyme and activate the AmpliTaq Gold DNA polymerase. This was followed by 40 to 45 cycles of denaturing at 95°C for 15 s and annealing/extension at 60°C for 1 min. Data were collected and analysed with Sequence Detector v1.6.3 software (Applied Biosystems) as previously described (McCallum et al. 2006) to generate gene copy number.
Results
CCN3 reduces cell growth and causes induction of apoptosis in K562 cells
To investigate the functional capacity of CCN3, we used both (i) transfection and (ii) recombinant protein to determine effect. Cell growth was measured using colony formation in methyl cellulose culture and was further evaluated using cell cycle analysis and Western blotting to detect the intracellular signaling events of caspase 3 cleavage and ERK phosphorylation.
CCN3 expression exerts growth regulation in K562 cells
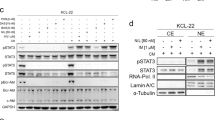
CCN3 was transfected into K562 cells using nucleofector™ technology and compared to cells transfected with empty vector (EV) and cells treated with imatinib (1 µM). Increased Ccn3 expression significantly reduced K562 cell colony formation capacity by 65.4% ± 18.8 to that of control (n = 3, p = 0.027)(Fig. 1a). In addition, increased levels of Ccn3 caused cells to accumulate in the subG0 region of cell cycle (Mean subG0 9.9% ± 4.6 for Control and 21.8% ± 0.7 for Ccn3 expressing cells (n = 3, p = 0.027) (Fig. 1b). Western blot analysis showed that Ccn3 expression was undetected in K562 cells (EV) whilst transfection with vector containing CCN3 dramatically increased expression levels (Fig. 1c). Increased expression was accompanied by an increase in the levels of cleaved caspase 3 product and a reduction in phosphorylation of Erk2 (Mean reduction 42% ± 10.4, n = 3 p = 0.01) (Fig. 1c). Optical densitometry was performed to show changes in the magnitude of Erk phosphorylation and cleaved caspase 3 (Fig. 1d).

CML cells expressing CCN3 exhibit growth regulation. K562 cells transfected with CCN3 (CCN3) were compared to cells transfected with empty vector (EV) and cells treated with imatinib (1 µM). Colony formation was measured after 7 days and is shown as a percentage of colony formation for cells transfected with empty vector (a). Induction of apoptosis was measured by the number of events within the sub G0 region of cell cycle; analysis was performed on 20,000 events using winMDI software and data were generated and then ranked from a common gate in the subG0 area (b). Western blot analysis was performed to identify Ccn3 expression, accumulation of cleaved caspase 3 and levels of phosphorylated Erk1 and Erk2 (c). Actin expression is shown as a control for protein loading. Optical densitometry was performed to show changes in Erk phosphorylation and cleaved caspase 3 (d)
K562 cells are responsive to treatment with recombinant CCN3
K562 cells were treated with recombinant Ccn3 (rCcn3, 1nM) and compared to untreated cells (Control). Cells treated with rCcn3 had reduced colony formation capacity 14% ± 2.1 compared to untreated cells (Fig. 2a) (n = 3, p = 0.015). Similarly, rCcn3 caused an accumulation of cells within the subG0 area of cell cycle (Mean for subG0 9.3% ± 3.9 and 23.7% ± 6.9 for control and rCcn3 respectively (Fig. 2b) (n = 3, p = 0.014). Western blot analysis showed reduced Erk phosphorylation and an increase in cleaved caspase 3 levels as a consequence of rCcn3 treatment (Fig. 2c) (n = 3). Optical densitometry was performed to show alterations in levels of Erk phosphorylation and cleaved caspase 3 as a result of rCCN3 treatment (Fig. 2d).

CML cells respond to treatment with recombinant Ccn3. K562 cells treated with recombinant Ccn3 (rCcn3, 1nM) were compared to untreated cells (Control) and evaluated for growth regulation. Colony formation was measured after 7 days and is shown as a percentage of colony formation by control cells (a). Induction of apoptosis was measured by the number of events within the sub G0 region of cell cycle; analysis was performed on 20,000 events using winMDI software and data were generated and then ranked from a common gate in the subG0 area (b). Western blot analysis was performed to identify accumulation of cleaved caspase 3 and levels of phosphorylated Erk1 and Erk2 (c). Actin expression is shown as a control for protein loading. Optical densitometry is shown for changes in Erk phosporylation and levels of cleaved caspase 3 for rCCN3 treated cells in comparison to control (d)
CCN3 expression enhances Imatinib induced apoptosis
Since CCN3 expression and treatment with recombinant Ccn3 restored growth regulation and induction of apoptosis in CML cells, we wished to investigate if CCN3 could augment imatinib induced cell death. K562 cells were transfected with vector or vector containing CCN3. Clones stably expressing vector constructs were selected using G418 resistance. Ccn3 expressing cells had a reduced growth rate compared to mock transfected cells (49% reduction in growth by day 5, data not shown; (p = 0.005)). Cells expressing CCN3 (CCN3) or empty vector (Mock) were then untreated (control) or treated with Imatinib (1 μM or 5 μM) for 48 h. CCN3 expression increased the number of events within the subG0 phase of cell cycle for both treatment with 1 μM imatinib (24.5% ± 4.6 subG0 events for CCN3 and 10.8% ± 4.1 for mock transfected cells respectively (n = 3, p = 0.040)) and 5 μM imatinib (32.3% ± 3.3 subG0 events for CCN3 and 16.1% ± 2.8 for mock transfected cells respectively (n = 3, p = 0.001)) at 48 h (Fig. 3a). To further evaluate the magnitude and longevity of CCN3 enhanced apoptosis, CCN3 and mock transfected cells were treated with Imatinib (5 μM) for 96 h. At 48 h, CCN3 expressing cells showed enhanced apoptosis in response to imatinib when compared to mock transfected cells (45.0% ± 6.7 and 28.2% ± 2.8 of events in sub G0 for CCN3 and mock transfected cells respectively (n = 3, p = 0.030 (Fig. 3b). CCN3 expressing cells showed enhanced susceptibility to imatinib induced apoptosis at 72 h and 96 h; (66.7% ± 0.6 and 44.2% ± 1.8 of events in sub G0 for CCN3 and mock transfected cells respectively at 72 h (n = 3, p = 0.001)) and (75.1% ± 3.9 and 52.7% ± 1.9 of events in sub G0 for CCN3 and mock transfected cells respectively at 96 h (n = 3, p = 0.002)).


CCN3 expression enhances Imatinib induced apoptosis. K562 CML cells were stably transfected with CCN3 (CCN3) or vector alone (Mock) and treated with Imatinib (1 µM or 5 µM) for 48 h. Flow cytometric analysis was performed on 20,000 events, data were then generated and ranked from a common gate in the subG0 area. The number of events in the subG0 area for CCN3 and mock transfected cells are shown (a). CCN3 and mock transfected cells were treated with 5 µM imatinib for a period of 96 h and flow cytometric analysis was performed (as above). The number of events in the subG0 area for CCN3 and mock transfected cells are shown (b)
CCN3 expression is altered in CML
We have previously shown that CCN3 expression is down-regulated as a consequence of Bcr-Abl kinase activity in CML. Further investigation of BCR-ABL and CCN3 expression was performed on BM and peripheral blood (PB) mononuclear cell extracts from CML patients at diagnosis. BCR-ABL expression was generally high (3.28 ± 4.9 × 104 copies per 5 µl cDNA for BM and 1.34 ± 1.1 × 104 copies per 5 µl cDNA for PB) whilst CCN3 expression was low (6.13 ± 5.6 × 102 copies per 5 µl cDNA for BM and 2.58 ± 3.7 × 103 copies per 5 µl cDNA for PB) (Fig. 4a). Analysis of individual patients following treatment with imatinib showed a clear trend; those with low or undetectable levels of CCN3 at diagnosis were more likely to achieve a 3 log reduction within 6 months (optimal response), whilst those with higher levels of expression had a sub-optimal response to imatinib treatment (data not shown). To further investigate this phenomenon, protein was prepared from CD34+, mononuclear and neutrophil cells derived from NBM and from CML BM where the patient had a sub-optimal response to imatinib. Western blot analysis showed that CCN3 expression was high in normal CD34+ stem and mononuclear cells whilst CCN3 expression was undetectable in CML CD34+ stem cells and neutrophils (Fig. 4b). To then determine if primary human CML stem cells were responsive to Ccn3, we treated CML CD34+ stem cells from peripheral blood samples at diagnosis with recombinant Ccn3 (rCcn3; 1nM-1pM) for 24 h. Cells were then plated in methyl cellulose and counted after seven days. Treatment with imatinib (1 μM) reduced the clonogenic capacity of CML CD34+ cells by 33.1% ± 11.4 (n = 3, p = 0.007) whilst treatment with rCcn3 showed dose dependent growth inhibition; 19.5% ± 4.0 for 1nM (n = 3, p = 0.001), 17.8% ± 2.7 for 100pM (n = 3, p < 0.001) and 16.6% ± 4.6 for 10pM rCcn3. Treatment with 1pM rCcn3 did not significantly affect colony formation capacity (Fig. 4c).

Primary CML cells express low levels of CCN3 and respond to recombinant Ccn3. CCN3 and BCR-ABL levels at diagnosis were evaluated using Real-time PCR (EAC protocol for BCR-ABL expression). Gene copy number for CCN3 and BCR-ABL expression levels were compared for BM (n = 16) and PB (n = 9) samples (a). Western blot analysis was performed to detect Ccn3 expression levels in extracts from CD34 + (1), mononuclear (2) and neutrophil (3) cell preparations derived from NBM and CML BM at diagnosis. Ccn3 was detected using the NH5 antibody and expression is shown compared with levels of actin (b). Primary CML CD34+ cells (n = 3) were isolated from CML peripheral blood (PB) at diagnosis. Cells were treated with rCcn3 (1nM – 1pM) or untreated (Control) for 24 h prior to plating in methyl cellulose. Colonies were counted after 7 days and are expressed as a percentage of colony formation compared to control (c *denotes p < 0.05)
Discussion
CCN3, a member of the CCN family of growth regulatory proteins has been shown to exert growth enhancing and growth inhibitory properties in a cell context specific manner. CCN3 is associated with increased invasive potential and metastasis in Ewings sarcoma (Benini et al. 2005; Manara et al. 2002) and is linked with expression of the multi drug resistant proteins in osteosarcoma (Perbal et al. 2008). CCN3 is also a marker for prostatic cell transformation and early detection of malignancy (Maillard et al. 2001). In contrast, CCN3 acts as a tumour suppressor in melanoma, glioblastoma, adrenocortical tumours and in CML (McCallum and Irvine 2009). Reduced CCN3 expression is associated with the disorganized structure and increased proliferative capacity in the epidermis in melanoma and increased aggressiveness in glioblastomas (Fu et al. 2004; Fukunaga-Kalabis et al. 2007; Sin et al. 2007). CCN3 secretion is a recognised mechanism used in metastatic adrenocortical tumours and in CML cells to evade growth regulation. In CML, reduced expression of CCN3 is a direct consequence of Bcr-Abl kinase activity and cellular Ccn3 is rapidly exported to evade growth inhibition. In this report we have investigated CCN3 mode of regulation in CML cells.
In a human CML cell line model (K562), over-expression of CCN3 or treatment with the recombinant protein results in a significant reduction in cell growth. The discrepancy between CCN3 expression and treatment with rCCN3 may be due to sustained CCN3 expression over the experimental period for colony formation (7 days) as opposed to a 24 h pre-treatment prior to plating in methyl cellulose culture. CCN3 reduced phosphorylation of Erk and increased apoptosis by enhancing caspase 3 cleavage. We have previously shown that reduced Erk phosphorylation as a consequence of the U0126 inhibitor, correlates with reduced clonogenic and proliferative capacity of K562 cells. CCN3 may compromise cell survival by reducing Erk phosphorylation causing decreased expression of pro-survival factors such as BCL-2, BCL-xL and MCL-1 (Balmanno and Cook 2009). CCN3 expression was shown to augment imatinib induced apoptosis and suggests CCN3 acts a tumour suppressor or pro-apoptotic factor.
We have previously shown CML patients at diagnosis have low or undetectable levels of CCN3 and CML CD34+ stem cells have low CCN3 expression which increases in response to imatinib treatment (McCallum et al. 2006). Ongoing monitoring of CML patients has subsequently demonstrated that a sub-population of patients have higher levels of CCN3 at diagnosis. These patients did not achieve a 3 log reduction in BCR-ABL levels within 6 months which is known to be associated with poorer prognosis. Analysis of Ccn3 protein within these samples showed that although mononuclear cells expressed Ccn3, the stem cell population had low or undetectable levels of Ccn3 expression. Since Ccn3 is clearly expressed in stem, mononuclear and neutrophil cells in NBM, CCN3 down-regulation is a key event in BCR-ABL leukaemogenesis. CCN3 appears to compromise BCR-ABL+ cell resistance to the induction of apoptosis. Primary CML CD34+ stem cells were responsive to recombinant Ccn3 which demonstrates a novel avenue for further evaluation in the management of CML.
CCN3 is a key regulator of haematopoiesis; de-regulation within this pathway enhances BCR-ABL leukaemogenesis by promoting cell survival and eliminating pro-apoptotic factors through the Erk signalling pathway. Manipulation of Ccn3, provides a novel strategy for therapeutic intervention to overcome oncogene mediated survival signals and restore apoptosis.
References
Balmanno K, Cook SJ (2009) Tumour cell survival signalling by the ERK1/2 pathway. Cell Death Differ 3:368–377
Beillard E, Pallisgaard N, van der Velden VH, Bi W, Dee R, van der Schoot E, Delabesse E, Macintyre E, Gottardi E, Saglio G et al (2003) Evaluation of candidate control genes for diagnosis and residual disease detection in leukemic patients using 'real-time' quantitative reverse-transcriptase polymerase chain reaction (RQ-PCR) - a Europe against cancer program. Leukemia 12:2474–2486
Benini S, Perbal B, Zambelli D, Colombo MP, Manara MC, Serra M, Parenza M, Martinez V, Picci P, Scotlandi K (2005) In Ewing's sarcoma CCN3(NOV) inhibits proliferation while promoting migration and invasion of the same cell type. Oncogene 27:4349–4361
Chevalier G, Yeger H, Martinerie C, Laurent M, Alami J, Schofield PN, Perbal B (1998) novH: differential expression in developing kidney and Wilm's tumors. Am J Pathol 6:1563–1575
Clarkson BD, Strife A, Wisniewski D, Lambek C, Carpino N (1997) New understanding of the pathogenesis of CML: a prototype of early neoplasia. Leukemia 9:1404–1428
Deininger MW, Goldman JM, Melo JV (2000) The molecular biology of chronic myeloid leukemia. Blood 10:3343–3356
Deininger MW, Holyoake TL (2005) Can we afford to let sleeping dogs lie? Blood 5:1840–1841
English D, Andersen BR (1974) Single-step separation of red blood cells. Granulocytes and mononuclear leukocytes on discontinuous density gradients of Ficoll-Hypaque. J Immunol Methods 3:249–252
Fu CT, Bechberger JF, Ozog MA, Perbal B, Naus CC (2004) CCN3 (NOV) interacts with connexin43 in C6 glioma cells: possible mechanism of connexin-mediated growth suppression. J Biol Chem 35:36943–36950
Fukunaga-Kalabis M, Martinez G, Telson SM, Liu ZJ, Balint K, Juhasz I, Elder DE, Perbal B, Herlyn M (2007) Downregulation of CCN3 expression as a potential mechanism for melanoma progression. Oncogene 27:2552–60
Gabert J, Beillard E, van der Velden VH, Bi W, Grimwade D, Pallisgaard N, Barbany G, Cazzaniga G, Cayuela JM, Cave H et al (2003) Standardization and quality control studies of 'real-time' quantitative reverse transcriptase polymerase chain reaction of fusion gene transcripts for residual disease detection in leukemia - a Europe Against Cancer program. Leukemia 12:2318–2357
Gellhaus A, Propson S, Gabriel HD, Gruemmer R, Duerig J, Klein-Hitpass BL, Maass K, Perbal B, Winterhager E (2003) NOV is associated with CX3 but not with CX0 and TRCX43 in human choriocarcinoma transfectants: evidence for potential growth-regulatory functions. Mol Pathol 56:75
Jorgensen HG, Holyoake TL (2001) A comparison of normal and leukemic stem cell biology in Chronic Myeloid Leukemia. Hematol Oncol 3:89–106
Kumar L (2006) Chronic myelogenous leukaemia (CML): an update. Natl Med J India 5:255–263
Li WX, Martinerie C, Zumkeller W, Westphal M, Perbal B (1996) Differential expression of novH and CTGF in human glioma cell lines. Mol Pathol 91-97.
Maillard M, Cadot B, Ball RY, Sethia K, Edwards DR, Perbal B, Tatoud R (2001) Differential expression of the ccn3 (nov) proto-oncogene in human prostate cell lines and tissues. Mol Pathol 4:275–280
Manara MC, Perbal B, Benini S, Strammiello R, Cerisano V, Perdichizzi S, Serra M, Astolfi A, Bertoni F, Alami J et al (2002) The expression of ccn3(nov) gene in musculoskeletal tumors. Am J Pathol 3:849–859
McCallum L, Irvine AE (2009) CCN3–a key regulator of the hematopoietic compartment. Blood Rev 2:79–85
McCallum L, Price S, Planque N, Perbal B, Pierce A, Whetton AD, Irvine AE (2006) A novel mechanism for BCR-ABL action: stimulated secretion of CCN3 is involved in growth and differentiation regulation. Blood 5:1716–1723
Nowell PC, Hungerford D (1960) A minute chromosome in human chronic granulocytic leukaemia. Science 132:1497
Perbal B (2001) NOV (nephroblastoma overexpressed) and the CCN family of genes: structural and functional issues. Mol Pathol 2:57–79
Perbal B, Zuntini M, Zambelli D, Serra M, Sciandra M, Cantiani L, Lucarelli E, Picci P, Scotlandi K (2008) Prognostic value of CCN3 in osteosarcoma. Clin Cancer Res 3:701–709
Planque N, Perbal B (2003) A structural approach to the role of CCN (CYR61/CTGF/NOV) proteins in tumourigenesis. Cancer Cell Int 1:15
Rowley ID. (1973). A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature 290-3.
Scotlandi K, Benini S, Manara MC, Cerisano V, Perdichizzi S, Strammiello R, Perbal B (2003). Biological role of NOVH in Ewings sarcoma cells. Mol Pathol 73
Sin WC, Bechberger JF, Rushlow WJ, Naus CC (2008) Dose-dependent differential upregulation of CCN1/Cyr61 and CCN3/NOV by the gap junction protein Connexin43 in glioma cells. J Cell Biochem 103:1772–1782
Wong S, Witte ON (2001) Modelling Philadelphia chromosome positive leukemias. Oncogene 20:5644–5659
Acknowledgements
This work has been supported by the Leukaemia Research Fund (LRF, UK), Northern Ireland Leukaemia Research Fund (NILRF, UK) and the Elimination of Leukaemia Fund (ELF, UK).
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
McCallum, L., Lu, W., Price, S. et al. CCN3: a key growth regulator in Chronic Myeloid Leukaemia. J. Cell Commun. Signal. 3, 115–124 (2009). https://doi.org/10.1007/s12079-009-0058-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12079-009-0058-2