
Abstract
Human Rhinoviruses (HRV) are the most common viral agents, being responsible for upper as well as lower respiratory tract infections. Evidence demonstrating that HRV disease is not exclusively limited to the upper airways and may cause lower respiratory complications, together with the frequency of HRV infections and the increasing number of immunocompromised patients underline the need for including HRV in virological diagnostics of acute lower respiratory tract illness. This article describes the development and optimization of a reverse transcription (RT) real-time PCR assay for quantification of HRV RNA in clinical samples. Efficiency, sensitivity, specificity, inter- and intra-assay variability, and dynamic range have been determined. Subsequently, the assay has been validated on bronchoalveolar lavage (BAL) specimens obtained from immunocompetent and immunocompromised patients.
Similar content being viewed by others

Introduction
PCR assays have markedly improved the diagnosis of Human Rhinoviruses (HRV) infections by increasing sensitivity in comparison to traditional cell culture [1]; however, many RT-PCR protocols still are time-consuming. Real-time PCR assays have resulted in improving virus detection and quantification [2]. Rapidity and quantitative results represent important advantages in the diagnostic workup of HRV infection and could be of relevance considering the future potential availability of antiviral agents. Human rhinoviruses are the most common viral agents in humans, being the over 110 serologic types responsible for about 30–50% of all the cases of common colds and associated upper respiratory tract complications in both adults and children. Although HRV are generally temperature restricted in replication with optimal growth at 33–35°C, the temperatures observed in the tracheobronchial tree are often lower than body core temperatures, also in relation to external temperature and frequency of ventilation, and so are permissive for HRV replication [3]. Moreover, it has been evidenced that many HRV serotypes can replicate efficiently at core body temperature with modest differences in terms of infectious titres (<0.5–1.0 log10 TCID50) [4]. Indeed, several studies have linked HRV infection to illnesses in the lower respiratory tract in immunocompetent patients, including exacerbations of pre-existing airways disease in those with asthma, chronic obstructive pulmonary disease (COPD) or cystic fibrosis, and pneumonia and bronchiolitis in children aged <5 years hospitalized for HRV infection [5]. However, a recent study on hospitalized adults with pulmonary disease found a prevalence of HRV in bronchoalveolar lavage (BAL) specimens of 31.2% without evidencing a significant difference of prevalence in relation to the presence of COPD, pneumonia or acute respiratory illness [6]. In contrast to immunocompetent subjects, HRV clearance in immunocompromised patients may be delayed with prolonged shedding leading to the onset of life-threatening conditions and chronic infections [7–9]. Evidence demonstrating that HRV disease is not exclusively limited to the upper airways and may cause lower respiratory complications, together with the frequency of HRV infections and the increasing number of immunocompromised patients, underline the need for including HRV in virological diagnostics of acute lower respiratory tract illness. However, not many laboratories and institutions have adopted HRV diagnostics in the routine clinical use, and limited informations are available on HRV clinical impact in comparison with that of other respiratory viruses.
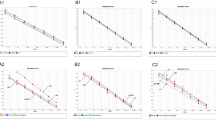
The aim of this study was to develop and validate a RT real-time PCR assay for quantification of HRV RNA in clinical samples. Efficiency, sensitivity, specificity, inter- and intra-assay variability and dynamic range have been determined (Fig. 1).

Standard curve (from 102 to 105 copies/reaction) and dynamic range (from 107 to 101 copies/reaction) of the real-time RT-PCR developed in this study
Materials and Methods
Virus and Clinical Specimens
Prototype rhinoviruses were obtained from the American Type Culture Collection (ATCC, Manassas, VA). Clinical specimens originated from the Virology Unit of the Azienda Ospedaliero-Universitaria San Giovanni Battista, Turin, and included 110 bronchoalveolar lavages (BAL) obtained from 84 patients (M/F, 57/27; mean age, 57.8 years; range, 16–84). Bronchoalveolar lavage procedure was performed as previously described [10] for investigating the cause of unexplained fever, and/or respiratory symptoms, and/or new infiltrates on chest X-ray or for checking up a previous positivity or as routine follow-up in lung transplant recipients. Before processing, specimens were thawed and liquefied with 1:1 N-acetylcisteine. Clinical specimens were divided in two groups: (I) 23 samples from 21 immunocompetent individuals, and (II) 87 from 63 immunocompromised patients (including 57 from transplant recipients, and 30 from patients with other conditions such as chemotherapy, HIV infection or long-term use of corticosteroids). Discharge diagnosis was made according to the International Classification of Diseases—Italian version 2002, based on the 9th revision Clinical Modification [ICD9CM].
RNA Extraction and RT-Reaction
Automated extraction of RNA was performed with the NucliSens easyMAG platform (bioMeriéux, Marcy l’Etoile, France). RNA was extracted from 500 μl volume of clinical specimens, according to manufacturer’s instructions, and eluted to a final volume of 110 μl. The RT reaction was done in a separate tube by a random cDNA syntesis from 10 μl of extracted RNA in two step: first a reaction mixture containing random primers (50 ng/ml)(Invitrogen) and 10 mM dNTPs (Invitrogen, Carlsbad, CA) was added and incubated at 65°C for 5 min using the 9800 Fast Thermal Cycler (Applied Biosystems, Monza, Italy); subsequently, a second reaction mixture containing 0.1 M DTT, 10× buffer (200 nM Tris–HCl [pH 8.4], 500 nM KCl), RNase OUTTM (40 unit/μl)(Invitrogen) and reverse transcriptase (50 unit/μl)(SuperScriptTM II RT, Invitrogen), giving a total volume 20 μl, was used. After incubation for 10 min at 25°C, 50 min at 42°C and 15 min at 70°C, the cDNA mixture was used as target cDNA.
Cloning of PCR Product
Primers were designed within the highly conserved 5′-UTR region of HRV genome (Table 1) using the Primer Express 3.0 Software (Applied Biosystems, Cheshire, UK). Briefly, 2 μl of cDNA was added to 28 μl of PCR solution containing buffer 1×, 6 mM MgCl2, 1 unit recombinant Subtherm DNA polymerase (Sic, Rome, Italy), 200 μM of each dNTP, 25 μM of each sense and antisense primer. After an initial denaturation step of 2 min at 94°C, the first-round PCR amplification was carried out under the following conditions: 95°C for 0 s, 62°C for 15 s, 72°C for 15 s for 35 cycles, then 1 cycle at 72°C for 7 min using the 9800 Fast Thermal Cycler (Applied Biosystems). About 20 μl of PCR product (235 bp) was loaded onto a 4% (W/V) agarose gel containing 0.3 μg/ml ethidium bromide. The gel was visualized on a UV board. The PCR product was cloned using pTOPO-TA cloning (Invitrogen). Recombinant plasmid was propagated in TOP10 high-efficiency chemically competent cells (Invitrogen) using the heat shock procedure. After overnight culture, selected transformed clones were amplified by culture in liquid LB medium (10 g BACTOTRYPTONE, 5 g yeast extract, 171 mM NaCl, 15 g/l agar, pH 7.5) containing 50 μg/ml of ampicillin. Plasmid DNA was extracted and purified using the Wizard Plus SV Miniprep DNA Purification System (Promega, Madison, WI). The plasmid concentration was estimated on spectrophotometric reading at OD260. The DNA copy number of the target plasmid was calculated from the molecular weight of the construct (2,722,500 MW) and Avogadro number (6.02 × 1023). About 1 μl of target plasmid contained 4.3 × 1010 DNA copy number. To determine the sensitivity of the PCR assays, stock preparations were diluted to 1 × 10−1 copies/μl by a series of 10-fold dilutions. The limit of detection is defined the lowest concentration of target quantified, whereas the efficiency of RT-PCR assay was also evaluated and is defined as 10(−1/slope) [11].
Negative controls with RNAse-free sterile water (Sigma) were included in each batch of test samples for checking up carry-over contamination.
Real-Time PCR
Reaction mixture contained 1 × Master Mix (Platinum qPCR supermix—UDG with ROX, Invitrogen), 0.2 mM primers and 0.1 mM FAM probe for target; 0.06 mM primers for internal control and 0.09 mM VIC probe at the 3′-terminus. About 2 μl of cDNA were added to 18 μl of the reaction mix, giving a final volume of 20 μl. Uracil-DNA glycosylase was used to eliminate PCR ‘carry over’ contaminations from previous PCR reactions. Amplification profile was optimized for the 7300 Real Time PCR System (Applied Biosystems) as follows: one cycle of decontamination at 50°C for 2 min, one cycle of denaturation at 95°C for 10 min followed by 45 cycles of amplification at: 95°C for 15 s, 60°C for 60 s. The cycle number during which the fluorescence signal is above the background (Ct) is proportional to the initial log concentration of the target DNA. For each run a standard curve was created in a 4-log range by 1:10 serial dilutions of the HRV DNA plasmid standard. Quantification was determined by normalizing results on the basis of spectrophotometric analysis at 260 nm.
Amplification data were analyzed by the Sequence Detection System software (Applied Biosystems).
Specificity
A ‘nucleotide-nucleotide blast’ search for short nucleotide sequences performed at the National Center for Biotechnology Information and the National Library of Medicine web site (www.ncbi.nlm.nih.gov/blast/) confirmed that the primer pairs used amplify the following HRV sequences (accession numbers EU700002.1, EU699985.1, EU699972.1, EU699969.1, EU699948.1, EU699945.1, EU096058.1, EU096054.1, EU096010.1, EU095996.1, EU095988.1, EU126773.1, EU126734.1, EU126730.1, EU126686.1, EU126672.1, DQ473497.1, Z29656.1, DQ316298.1, AF108165.1, AF108153.1, D00239.1, EU699994.1, EU699944.1, EU096052.1, EU096019.1, EU096006.1, EU096000.1, EU095987.1, EU126728.1, EU126695.1, EU126682.1, EU126676.1, EU126663.1, EF582386.1, AF542442.1, DQ316279.1, AF108179.1, AF108177.1, EU700019.1, EU700016.1, EU700011.1, EU700005.1, EU700001.1, EU699986.1, EU699984.1, EU699981.1, EU699971.1, EU699970.1, EU699964.1, EU699963.1, EU699961.1, EU699943.1, EU096040.1, EU095999.1, EU126780.1, EU126769.1, EU126716.1, EU126675.1, EF173415.1, DQ473507.1, AF542443.1, AF542437.1, DQ316302.1, DQ316297.1, DQ316264.1, AF108176.1, AF108173.1, AF108169.1, AF108168.1) and do not amplify other viruses pathogenic to humans.
Controls
Negative controls: A number of precautions were undertaken to prevent the occurrence of false-positive results. Each run included control reactions lacking template (no-template controls) to test for the presence of contamination or the generation of nonspecific amplification products under the assay conditions used.
Positive controls: The presence of cellular GAPDH transcript was analysed as internal control and marker of sensitivity of the assay; primer sequences for GAPDH were designed using the software OligoPerfectTM Designer (Invitrogen) within exon 6 (forward primer) and exon 8 (reverse primer) and are reported in Table 1.
Statistical Analysis
The coefficient of variation for samples quantified in repeated measurements was calculated. Descriptive statistics were expressed as absolute value, percentage and median as appropriate. The Chi-squared test was applied to analyze results in clinical specimens. Statistical analysis was performed using a commercially available software (Med Calc version 9.2.1.0). A P-value <0.05 was considered statistically significant.
Results
Efficiency and Sensitivity
These parameters were assessed by repeated testing of serial logarithmic dilutions of the plasmid standard (covering a range of 4 logs from 102 to 105). The number of genome copies in the plasmid preparation used for dilutions was determined by spectrophotometry at 260 nm. After PCR amplification, the Ct value (crossing point of the amplification curve with the pre-set threshold of fluorescence detection) of individual dilution steps was plotted against the initial virus copy number, leading to a typical standard curve. The amplification efficiency, defined by the standard curve slope, was generally between three and four. The consistency of replicates was measured by the correlation coefficient (R 2), which indicates the linearity of the Ct values plotted in the standard curves. The R 2 index was higher than 0.990. The actual sensitivity of assay was determined by the lowest standard dilution consistently detectable in replicate reactions at a frequency of 100% and it was found to be of 100 copy/reaction and was linear (quantifiable) up to 101 copies. A standard dilution of 10−1 copy/reaction was detected at a frequency of 10%, while that of 10−2 copy/reaction at a frequency of 0%. The limit of detection was 10−1 copy/reaction. The efficiency of the reaction is considered acceptable if it falls between the range of 1.7 and 2.2 with 2 being ideal. The efficiency of our real-time RT-PCR assays was 2.08.
The reproducibility was expressed as the coefficient of variation (CV) in the log10 values of the concentration. Furthermore, intra- and inter-assay variability was evaluated over different concentrations ranging from 102 to 105 plasmid copies within a single run (n = 10) or different run experiments (n = 10) by CV value of the Ct and is reported in Table 2. Quantification of HRV was highly reproducible for as few as 102 copies.
Variability
The variability was studied by analysing 100 samples tested in duplicate in five experiments. The results of the quantification revealed that the median (5th, 95th) CV was 3.2% (0.15–13.5%).
Specificity
The analytical specificity of the RT-PCR assay was determined by testing coxsackievirus types B1 (ATCC VR-28), B2 (ATCC VR-29) and B3 (ATCC VR-30), echovirus types 1 (ATCC VR-31), 6 (ATCC VR-36) and 9 (ATCC VR-39), enterovirus type 68 (ATCC VR-561), 69 (ATCC VR-785), 70 (ATCC VR-836) and 71 (ATCC VR-1432), human parainfluenza viruses (PIV 1 [ATCC VR-94], PIV 2 [ATCC VR-92], PIV 3 [ATCC VR-93]), influenza viruses (influenza A virus H1N1 [ATCC VR-95], H3N2 [ATCC VR-547], influenza B virus [ATCC VR-101]), human respiratory syncytial virus (RSV-A [ATCC VR-26], human adenovirus 3 (ATCC VR-3), 5 (ATCC VR-5) and 7 (ATCC VR-7), herpes simplex virus 1 (ATCC VR-260), human cytomegalovirus (ATCC VR-538), Epstein-Barr virus (ATCC VR-602), human coronavirus types 229E (ATCC VR-740) and OC43 (ATCC VR-1558), Streptococcus pneumoniae (ATCC 6301), Legionella pneumophila (ATCC 33152), Mycoplasma pneumoniae (ATCC 15377), Chlamydia pneumoniae (ATCC 53592). None of them resulted positive, thus indicating that this method is specific for HRV.
Dynamic Range
To examine the dynamic range of HRV RNA quantification by RT-PCR, serial dilutions of the plasmid standard ranging from 107 to 10 copies/reaction were carried out. The RT-PCR assay was able to quantify HRV RNA from 1010 to 100 copies/reaction with a dynamic range of 107–101 copies/reaction (R 2 = 0.999) obtained from linear regression analysis, without having to dilute high load samples.
Quantification of HRV in Clinical Samples
Viral loads in clinical specimens were investigated in duplicate reactions with the appropriate external standard preparations. The efficiency of viral RNA detection from clinical samples and the possible presence of polymerase inhibitors were monitored by using internal control, as described in the section ‘Materials and Methods.’ These controls permitted appropriate correction in the calculation of viral copy numbers. For the quantification of viral load, the slope (s) and the y-axis intercept (Y) (the y-axis intercept is the point at which the standard curve intersects with the ordinate; it indicates the theoretical detection limit of the reaction by revealing the Ct expected in the presence of a single target molecule in the sample) of the corresponding standard curve and the Ct of the target virus amplification were used according to the following equation: Po = Inverse log(Ct − Y/s), where Po is the number of virus copy equivalents in the PCR prior to amplification. Results of HRV quantification are summarized in Table 3. Briefly, HRV was positive in 12/110 (10.9%) BAL specimens, obtained from as many patients (12/84, 14.3%): in particular 11/87 (12.6%) samples from immunocompromised patients and 1/23 (4.4%) samples from immunocompetent patients (P = n.s.). Viral load was <220 Genome equivalents (GEq)/ml in the immunocompetent patient and ranged from <220 to 3.14 × 106 GEq/ml (median, 994) in the immunocompromised patients. Considering discharge diagnosis of pneumonia, respiratory insufficiency, exacerbations of pre-existing bronchopneumopathies, other pneumopathies, there was no significant difference of prevalence between immunocompetent and immunocompromised patients. HRV was also detected in one sample obtained during routine follow-up in one lung allograft recipient and in three cases with transplant complications. Results in clinical samples and main features of patients positive to HRV are reported in Table 4.
Discussion
This raticle describes the development of an in-house RT real-time PCR assay for quantification of HRV RNA in clinical samples.
Real-time PCR assays are described as ‘closed’ systems, as no post-amplification manipulation of the amplicon is required. The advantages of these systems include a reduced turnaround time, minimisation of the potential for carry-over contamination and ability to closely scrutinise the assay performance, thus representing a suitable tool for routine diagnostics in virology. The use of an external standard curve for quantification relies upon titration of an identically amplified template, in a related sample matrix, within the same experimental run. However, this approach may suffer from uncontrolled and unmonitored inter-tube variations and thus such experiments should be described as semi-quantitative. Despite this sub-optimal approach, fluorescence data are generally collected from PCR cycles that span the linear amplification portion of the reaction where the fluorescent signal and the accumulating DNA are proportional. Because the emissions from fluorescent chemistries are temperature dependent, data are generally acquired only once per cycle at the same temperature in order to monitor amplicon yield [12]. Then, the Ct of the sample at a specific fluorescence value can be compared with similar data collected from a series of standards by the calculation of a standard curve. The determination of the Ct depends upon the sensitivity and ability of the instrument to discriminate specific fluorescence from background noise, concentration and nature of the fluorescence-generating component and amount of template initially present. Real-time PCR offers significant improvements to viral load quantification because of its wide dynamic range that can accommodate at least eight log10 copies of nucleic acid template [13–15]. This is made possible because data are chosen from the linear phase of amplification where conditions are optimal, rather than the end-point where the final amount of amplicon could be affected by inhibitors, poorly optimised reaction conditions or saturation by inhibitory PCR by-products and double-stranded amplicon. The result of taking data from the end-point is that there may exist no relationship between the initial template and final amplicon concentrations. Real-time PCR for the study of viral load presents a lower inter- and intra-assay variability in comparison to conventional PCR [13, 14] and an equivalent or higher analytical sensitivity in comparison to traditional viral culture, or conventional single-round, and nested PCR [16]. Indeed, PCR methods have significantly improved the diagnosis of HRV infection. However, these reports could be an over-estimate due to the choice of smaller targets, which amplify more efficiently, or due to the use of different or improved primers for the real-time assays as the use of software to design optimised primers and oligoprobes is more common. When increased sensitivity and broad dynamic range are combined, it is possible to quantify template from samples containing a wide range of concentrations, as in clinical specimens. This avoids the need for dilution of the amplicon prior to conventional detection or repetition of the assay using a diluted sample because the first result falls outside the detection limits.
The performance of the RT real-time PCR developed in this study was examined over different concentrations of HRV RNA and it was found to be very sensitive with a minimum cut-off for detection of 100 copy/reaction and was linear up to 101 copies. The sensitivity, defined as the lowest concentration of HRV RNA quantified at a frequency of 100%, was found to be 100 copies/reaction. The assay reproducibility was high with a median inter-assay variability and intra-assay variability of 1.116% (range 0.785–1.699%) and 0.553% (range 0.088–0.671%), respectively, thus being superior to that obtained in other studies [17].
The assay developed in this study was based on primers amplifying the 5′-UTR of the viral genome, that is highly conserved among entero- and rhinoviruses, and therefore, many PCR protocols amplify also enteroviruses. Our assay resulted able to amplify 70 HRV sequences, as confirmed by BLAST search, and should not amplify other viruses pathogenic to humans, in particular enteroviruses. Other studies developed RT real-time PCR assays for detection of HRV [2, 18] in respiratory specimens; however, our assay has been developed and optimized on the basis of the standard amplification profile for the Applied Biosystems Real Time PCR System, thus allowing the simultaneous processing of the same clinical specimens for different viruses potentially involved in respiratory tract infections. Evaluation on clinical specimens confirmed the occurrence of HRV infection in the lower respiratory tract, as 10.9% of BAL specimens resulted positive. Although prevalence of infection tended to be higher in specimens obtained from immunocompromised patients, the difference did not reach the statistical significance, as well as no significant association with a discharge diagnosis was found. Regarding this, it has to be taken into account that all of our specimens, but one, presented a coinfection with at least another respiratory virus (including herpesviruses HSV, EBV, CMV, HHV-6 and -7, human metapneumovirus, human coronavirus, human bocavirus, parainfluenza viruses, influenza viruses, adenoviruses, RSV)(data not shown). HRV shedding in the immunocompromised host could be prolonged in comparison to the immunocompetent one, thus leading to the onset of severe complications, as well as it has been suggested an association with acute rejection in lung transplant recipients [7]. In our study, multiple sampling was available in particular for lung transplant recipients, however no repeated positivity was found, thus preventing the possibility to evaluate this issue and suggesting the need for further studies. Similarly, no significant association was found with the occurrence of exacerbation of pre-existing bronchopneumopaties. As the association between acute exacerbations of asthma and chronic obstructive pulmonary disease and respiratory viral pathogens, particularly HRV, is well recognized [19–21], the lack of association found in our study could be due to the small number, thus preventing us to evaluate this issue.
In conclusion, the RT real-time PCR assay developed in this study could represent a useful tool for diagnosing HRV infections, quantifying the viral load and could be applicable for routine diagnostic workup of upper as well as lower respiratory tract diseases. The availability of a quantitative approach for detection of HRV RNA could represent a useful tool to investigate the epidemiological and clinical role on HRV in clinical contexts involving the immunocompromised hosts, in particular lung transplant recipients, or the association with exacerbations of pre-existing bronchopneumopathies, in particular the relation between viral load and severity or duration of asthma exacerbations.
References
Hyypiä, T., Puhakka, T., Ruuskanen, O., Makela, M., Arola, A., & Arstila, P. (1998). Molecular diagnosis of human rhinovirus infections: comparison with virus isolation. Journal of Clinical Microbiology, 36, 2081–2083.
Kares, S., Lönnrot, M., Vuorinen, P., Oikarinen, S., Taurianen, S., & Hyöty, H. (2004). Real-time PCR for rapid diagnosis of entero- and rhinovirus infections using LightCycler. Journal of Clinical Virology, 29, 99–104. doi:10.1016/S1386-6532(03)00093-3.
McFadden, E. R., Jr., Pichurko, B. M., Bowman, H. F., et al. (1985). Thermal mapping of the airways in humans. Journal of Applied Physiology, 58, 564–570.
Papadopoulos, N. G., Sanderson, G., Hunter, J., & Johnston, S. L. (1999). Rhinoviruses replicate effectively at lower airway temperatures. Journal of Medical Virology, 58, 100–104. doi:10.1002/(SICI)1096-9071(199905)58:1<100::AID-JMV16>3.0.CO;2-D.
Hayden, F. G. (2004). Rhinovirus and the lower respiratory tract. Reviews in Medical Virology, 14, 17–31. doi:10.1002/rmv.406.
Minosse, C., Selleri, M., Zaniratti, M. S., et al. (2008). Frequency of detection of respiratory viruses in the lower respiratory tract of hospitalized adults. Journal of Clinical Virology, 42, 215–220. doi:10.1016/j.jcv.2008.01.012.
Kaiser, L., Aubert, J.-D., Pache, J.-C., et al. (2006). Chronic rhinoviral infection in lung transplant recipient. American Journal of Respiratory and Critical Care Medicine, 174, 1392–1399. doi:10.1164/rccm.200604-489OC.
Parody, R., Rabella, N., Martino, R., et al. (2007). Upper and lower respiratory tract infections by human enterovirus and rhinovirus in adult patients with hematological malignancies. American Journal of Hematology, 82, 807–811. doi:10.1002/ajh.20974.
Costa, C., Bergallo, M., Sidoti, F., et al. (2009). What role for human Rhinoviruses in the lower respiratory tract? New Microbiologica, 32, 115–117.
Costa, C., Elia, M., Astegiano, S., et al. (2008). Quantitative detection of Epstein-Barr virus in bronchoalveolar lavage from transplant and non-transplant patients. Transplantation, 86, 1389–1394. doi:10.1097/TP.0b013e3181890415.
Rasmussen, R., Meuer, S., Wittwer, C., & Nakagawara, K. (2001). Rapid cycle real-time PCR methods and application. Heidelberg: Springer Press.
Wittwer, C. T., Herrmann, M. G., Moss, A. A., & Rasmussen, R. P. (1997). Continuous fluorescence monitoring of rapid cycle DNA amplification. BioTechniques, 22, 130–138.
Paraskevis, D., Haida, C., Tassopoulos, N., et al. (2002). Development and assessment of a novel real-time PCR assay for quantitation of HBV DNA. Journal of Virological Methods, 103, 201–212. doi:10.1016/S0166-0934(02)00033-2.
Logan, C., O’Leary, J. J., & O’Sullivan, N. (2006). Real-time reverse transcription-PCR for detection of rotavirus and adenovirus as causative agents of acute viral gastroenteritis in children. Journal of Clinical Microbiology, 44, 3189–3195. doi:10.1128/JCM.00915-06.
Laurent, P., Le Roux, K., Grivard, P., et al. (2007). Development of a sensitive real-time reverse transcriptase PCR Assay with an internal control to detect and quantify chikungunya virus. Clinical Chemistry, 53, 1408–1414. doi:10.1373/clinchem.2007.086595.
van Elden, L. J. R., Nijhuis, M., Schipper, P., Schuurman, R., & van Loon, A. M. (2001). Simultaneous detection of influenza viruses A and B using real-time PCR. Journal of Clinical Microbiology, 39, 196–200. doi:10.1128/JCM.39.1.196-200.2001.
Lu, X., Holloway, B., Dare, R. K., et al. (2008). Real-time reverse transcription-PCR assay for comprehensive detection of human rhinoviruses. Journal of Clinical Microbiology, 46, 533–539. doi:10.1128/JCM.01739-07.
Deffernez, C., Wunderli, W., Thomas, Y., Yerly, S., Perrin, L., & Kaiser, L. (2004). Amplicon sequencing and improved detection of human rhinovirus in respiratory samples. Journal of Clinical Microbiology, 42, 3212–3218. doi:10.1128/JCM.42.7.3212-3218.2004.
Proud, D., & Chow, C.-H. (2006). Role of viral infections in asthma and chronic obstructive pulmonary disease. American Journal of Respiratory Cell and Molecular Biology, 35, 513–518. doi:10.1165/rcmb.2006-0199TR.
Camargo, C. A., Ginde, A. A., Clark, S., et al. (2008). Viral pathogens in acute exacerbations of chrnoic obstructive pulmonary disease. Internal and Emergency Medicine, 3, 355–359. doi:10.1007/s11739-008-0197-0.
Djukanovic, R., & Gadola, S. D. (2008). Virus infection, asthma, and chronic obstructive pulmonary disease. The New England Journal of Medicine, 359, 2062–2064. doi:10.1056/NEJMcibr0806978.
Acknowledgements
We thank Dr. Paolo Solidoro and Dr. Daniela Libertucci, Pneumology Division of San Giovanni Battista Hospital, Turin, for their assistance in clinical sample analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
Stefano Gambarino and Cristina Costa have equally contributed to this work and share first authorship.
Rights and permissions
About this article
Cite this article
Gambarino, S., Costa, C., Elia, M. et al. Development of a RT Real-Time PCR for the Detection and Quantification of Human Rhinoviruses. Mol Biotechnol 42, 350–357 (2009). https://doi.org/10.1007/s12033-009-9164-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12033-009-9164-x