
Abstract
Introduction
Coenzyme Q10 deficiency can be due to mutations in Coenzyme Q10-biosynthesis genes (primary) or genes unrelated to biosynthesis (secondary). Primary Coenzyme Q10 deficiency-4 (COQ10D4), also known as autosomal recessive spinocerebellar ataxia-9 (SCAR9), is an autosomal recessive disorder caused by mutations in the ADCK3 gene. This disorder is characterized by several clinical manifestations such as severe infantile multisystemic illness, encephalomyopathy, isolated myopathy, cerebellar ataxia, or nephrotic syndrome.
Methods
In this study, whole-exome sequencing was performed in order to identify disease-causing variants in an affected girl with developmental regression and Epilepsia Partialis Continua (EPC). Next, Sanger sequencing method was used to confirm the identified variant in the patient and segregation analysis in her parents.
Case Presentation
The proband is an affected 11-year-old girl with persistent seizures, EPC, and developmental regression including motor, cognition, and speech. Seizures were not controlled with various anticonvulsant drugs despite adequate dosing. Progressive cerebellar atrophy, stroke-like cortical involvement, multifocal hyperintense bright objects, and restriction in diffusion-weighted imaging (DWI) were seen in the brain magnetic resonance imaging (MRI).
Conclusions
A novel homozygous missense variant [NM_020247.5: c.814G>T; (p.Gly272Cys)] was identified within the ADCK3 gene, which is the first mutation in this gene in the Iranian population. Bioinformatics analysis showed this variant is damaging. Based on our patient, clinicians should consider genetic testing earlier to instant diagnosis and satisfactory treatment based on exact etiology to prevent further neurologic sequelae.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Epilepsia Partialis Continua (EPC) is a unique variant of prolonged focal motor status epilepticus with awareness, which is characterized by frequent myoclonic or clonic jerks usually arrhythmic. At a short distance, EPC is followed by a gradually progressive neurological disorder (Mameniškienė and Wolf 2017). The etiological agents, which cause EPC, are divided into two categories: focal and systemic (Khan et al. 2020). The Focal etiologic causes of EPC include Rasmussen encephalitis, tick-borne encephalitis (TBE), AIDS, tuberculoma, Creutzfeldt–Jakob disease (CJD), Cat-scratch disease (CSD), Herpes simplex encephalitis (HSE), and Japanese encephalitis (JE) (Valentin et al. 2015). In addition, stroke, focal cortical dysplasia, and neoplastic disease can cause EPC (Ribeiro et al. 2015). On the other hand, systemic factors are mitochondrial diseases, metabolic disorders, idiopathic diseases, and autoimmunity (Atmaca et al. 2018).
Mitochondrial encephalomyopathies include a group of complaints which have failure oxidative metabolism in the central nervous system and skeletal muscles (Li et al. 2020). Berbel-Garcia et al. (2004) declared that treatment of mitochondrial diseases with Coenzyme Q10 (CoQ10) is effective (Berbel-Garcia et al. 2004). CoQ10 (also known as Ubiquinone) is a lipid-soluble component of the mitochondrial inner membrane, which plays an essential role in the mitochondrial respiratory chain (electron transport chain: ETC) function. By this role, CoQ10 acts as electrons carrier from complexes I (NDSH: Ubiquinone reductase) and II (succinate: ubiquinone reductase) to complex III (ubiquinol cytochrome c oxidase). Thus, it participates in ATP production (Mancuso et al. 2010). The reduced form of CoQ10 (Ubiquinol) also has antioxidant activity, protecting membrane lipids, proteins, and mitochondrial DNA (mtDNA) against oxidative stress (Dallner and Sindelar 2000).
CoQ10 deficiency includes several clinical manifestations such as severe infantile multisystemic illness, encephalomyopathy, isolated myopathy, cerebellar ataxia, or nephrotic syndrome (Lamperti et al. 2003). This deficiency can be caused by mutations in CoQ10-biosynthesis genes (primary) including PDSS1, PDSS2, ADCK3, ADCK4, COQ2, COQ4, COQ6, and COQ9 genes, or genes unrelated to biosynthesis (secondary) (Potgieter et al. 2013). ADCK3 (also known as COQ8A; OMIM: 606,980) is one of the numerous genes related to CoQ10 deficiency, which presents with epilepsy, progressive cerebellar ataxia, migraine, and psychiatric disorders (Hikmat et al. 2016). The secondary type occurs more frequently in patients with mtDNA depletion syndrome and/or mutations in APTX, ETFDH, BRAF, NPC, or ACADVL genes (Fragaki et al. 2016). In this study, we reported a case suffering from EPC with a mutation in the CoQ10-biosynthesis gene (ADCK3).
Materials and Methods
Ethical Standard Statement and Written Consent
Proband was selected during the ataxia project based on clinically interesting findings such as EPC. Written consent was obtained from parents as legal guardians of the proband. This study was approved by the local ethics committee of the National Institute for Medical Research Development (NIMAD) of Iran (Ethics ID: IR.NIMAD.REC.1397.508). Therefore, this research has been done in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Whole Exome Sequencing and Bioinformatics Analysis
At the first step, 10 ml of whole blood was collected from the patients and their parents, and extracting gDNA was performed based on the salting-out protocol (Gaaib et al. 2011). The concentration and quality of the extracted DNA were evaluated using agarose gel electrophoresis and spectrophotometry absorbance reading at 260 nm. Then, Whole Exome Sequencing was performed by the Agilent SureSelect Human All Exon V7 Kit from Illumina and using the NovaSeq 6000 platform with an average depth of about 100x. Based on similar studies (Mohammadi et al. 2021a, b, c; Tavasoli et al. 2022), an in-house bioinformatics pipeline was performed by the following bioinformatics tools:
-
(A)
FASTP tool was utilized to evaluate quality control (QC) of reading length and depth (GC content ~ 50%, Phred score > 20) (Chen et al. 2018).
-
(B)
BWA aligning tool was used to map the raw reads to the (GRCh38/hg38) human reference genome (Jo and Koh 2015).
-
(C)
SAM (Sequence Alignment/Map) file, obtained from the alignment step, was converted to BAM (Binary Alignment Map) file using Samtools software (Li et al. 2009).
-
(D)
SNVs and insertion/deletion (Indel) variant calling were performed by GATK Haplotypecaller, FREEBAYES, and DeepVariant callers. The VCF (variant call format) file was generated (Ren et al. 2018; Supernat et al. 2018).
-
(E)
The VCF file was annotated by the Ensemble VEP tool (Thormann et al. 2019). The annotated VCF contained 53,991 variants.
Segregation analysis and variant confirmation
Reverse and forward primers were designed by PrimerQuest tool and UCSC genome browser blat tools. Then, qualities and features of primers were checked by OligoAnalyzer Tool. At the next step, Sanger sequencing Applied Biosystems 3130 Genetic Analyzer was used to confirm the identified variant in the proband and to study segregation in the family. Finally, CodonCode aligner tool was utilized for the analysis of Sanger sequencing results.
Results
Case Presentation
An affected eleven-year-old girl, a known case of poorly controlled epilepsy and developmental regression, was admitted due to increasing seizure frequency and severity. As the first child of the consanguineous parents (first cousin), she was born via normal vaginal delivery (NVD) at 38 weeks of gestational age without perinatal insult. Birth weight was 3.180 g and birth head circumference (HC) was 33 cm. Family history was unremarkable for epilepsy and developmental regression.
The patient’s developmental milestones were normal until 24 months of age that her first seizure with fever occurred. The patient’s seizures repeated as upward gaze and left focal clonic seizures. Phenobarbital was administered but seizures continued at least once per month. Gradually, developmental regression appeared first in motor aspects, including gait instability and ataxia, and later cognition and speech regression added. Also, her seizures were uncontrolled. Eventually, phenobarbital was not able to seizures controlling and she was admitted to another hospital for this problem at the age of 3 years old. Focal seizures and developmental regression were continued. At the age of 3 years, phenobarbital was stopped and sodium valproate and topiramate were started. According to uncontrolled seizures, topiramate was replaced with clobazam in the drug regimen. Focal seizures and developmental regression were continued.
We did not find any abnormality in the hematological and biochemical laboratory findings. Blood ammonia, blood lactate, ABG (PH) and bicarbonate (HCO3) concentrations were 58 micromol/L (normal range: 16–60 micromol/L), 17 mg/dL (normal range: 2–20 mg/dL), 7.4 (normal range: 7/35–7/45), and 21 mmol/L (normal range: 22–26 mmol/L) respectively. The concentration of serum amino acids was in normal ranges. Tandem mass spectrometry (MS/MS) and urine organic acids were normal. Covid-19 PCR was negative. A central hypothyroidism (TSH = 0.06 mIU/L [reference range 0.5–6.5mIU/L]) was reported in endocrinologist consult and Levothyroxine (50 mcg /day) was initiated. CSF analysis was normal, including glucose and protein were 65 mg/dL and 38 mg/dL, respectively. There were no white blood cell, red blood cell and bacteria in CSF. Echocardiography was performed at the age of 7 years and showed a mild to moderate mitral regurgitation and mitral valve prolapse. Ophthalmic examination and visual evoked potential were normal. Electroencephalography (EEG) revealed frequent lateralized epileptiform discharges and delta activities.
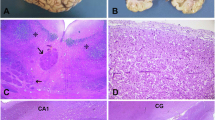
Brain MRI was performed at 2 and 3 years of age, revealing mild cerebellar atrophy and stroke-like signal changes. Also, multifocal cortical involvement and cerebellar atrophy (Fig. 1A, B) were observed at 5 and 7 years of age. At the age of 11 years, brain MRI (T1, T2, FLAIR, DWI, and ADC) was performed (Fig. 1C–H). The results showed progressive cerebellar atrophy, stroke-like cortical involvement, multifocal hyperintense bright objects, and restriction in DWI and ADC sequences.

Brain MRI. A and B Multifocal cortical involvement, a mild cerebellar atrophy at the age of 7 years and C, D, E, F, G, and H a progressive cerebellar atrophy, multifocal hyperintense bright objects, stroke like cortical involvement (restriction in DWI/ADC), and intact basal ganglia at the age of 11 years
At the beginning of hospitalization, the patient had persistent seizures which were not controlled with various anticonvulsant drugs despite adequate dosing. Due to mitochondropathy, use of sodium valproate was stopped. The patient was intubated and treated with high doses of medications such as Midazolam and Fentanyl. However, EPC seizures were still seen both at the patient’s bedside and in repeated EEGs. The patient was even treated with high-dose COQ10, after the preparation of WES result, but the seizures were not controlled.
Exome Results
Filtering the annotated VCF was performed by the R programming software to detect the most relevant variants in the proband by the following steps:
-
(A)
Removing variants with minor allele frequency (MAF) > 1%, based on GnomAD, ExAC, 1000Genome project, and Iranome. Remaining variants: 11,753.
-
(B)
Filtering synonymous, intronic, and noncoding variants based on consequence. Remaining variants: 1,109.
-
(C)
Removing variants which are not related to human phenotype ontology (HPO) terms. Remaining variants: 71.
According to the clinical and para-clinical findings, the genes related to the following HPO (The Human Phenotype Ontology) terms were considered in the analysis: Epilepsy HP:0,001,250, Developmental regression HP:0,002,376, Focal clonic seizure HP:0,002,266, Unsteady gait HP:0,002,317, Ataxia HP:0,001,251, Cognitive impairment HP:0,100,543, Cerebellar atrophy HP:0,001,272.
At the next step, 71 remaining variants were classified based on the American College of Medical Genetics and Genomics (ACMG) guideline (Nykamp et al. 2017). Finally, we checked the depth of reads of final variants using IGV (Integrative Genomics Viewer) software (Thorvaldsdóttir et al. 2013).
A novel homozygous missense variant in the ADCK3 gene [NM_020247.5: c.814G>T; (p.Gly272Cys)] was identified. ACMG classified this variant as likely pathogenic (class 2) (Table 1). Pathogenic variants in the ADCK3 gene are associated with primary Coenzyme Q10 deficiency-4 (COQ10D4), also known as autosomal recessive spinocerebellar ataxia-9 (SCAR9) (Lagier-Tourenne et al. 2008). We confirmed the homozygous state for this variant in the proband, as well as the heterozygote state in the parents by Sanger sequencing (Fig. 2). As a result, the c.814G>T variant in the ADCK3 gene segregated with the primary Coenzyme Q10 deficiency-4 in this family, and can be identified as the cause of disease in the proband. Therefore, based on the results of WES, the patient developed a Coenzyme Q deficiency, and she was treated with CoQ10; however, there were frequent increased seizures in the patient.

A Sanger sequencing chromatographs shows heterozygous missense variant in the parents. B Family pedigree of the 11-year-old affected girl offspring of first cousin parents. The affected proband is shown by arrow. The genotype of the parents for the c.814G>T variant is depicted on the pedigree
Discussion
Homozygous or compound heterozygous mutations in the ADCK3 gene cause COQ10D4, also known as SCAR9 (Lagier-Tourenne et al. 2008). In this study, WES identified a novel homozygous missense variant [NM_020247.5: c.814G>T; (p.Gly272Cys)] in an 11-year-old Iranian girl with EPC. The identified variant is in the Exon 6, which affects the atypical kinase chain, creates an amino acid change from Gly to Cys at position 272 (Fig. 3A). According to our knowledge, this is the first report from Iran.

A The ADCK3 gene contains 15 exons and spans ~ 90 kb. Graphical view of the COQ8A atypical kinase protein updated from UniProt (UniProtKB-Q8NI60). The canonical isoform length of the protein (Identifier: Q8NI60-1) has 647 amino acids and N-terminal transit peptide (residue 1–162), helical transmembrane region (residue: 214–230), protein kinase domain (residue 329–518), KxGQ motif (residue 276–279), and AAAS motif (residue 337–340). The [c.814G>T, (p.Gly272Cys)] variant is in the Exon 6, which affects the atypical kinase chain, creates an amino acid change from Gly to Cys at position 272. B 3D structure of the protein, which is provided by the PyMOL software. The difference between the side chain of Gly272 and Cys272 has been locally enlarged (PDB: 4ped). C 3D structure which is designed by ConSurf server database. According to this structure and conservation analysis of amino acids by ConSurf, Gly272 is a highly conserved amino acid with score 9 of 9. Also, this amino acid is evolutionary conserved in different species including rhesus, mouse, dog, elephant, chicken, and zebrafish based on UCSC genome browser
Alternative variants [NM_020247.5: c.815G>A; p.(Gly272Asp)] and [NM_020247.5: c.815G>T; p.(Gly272Val)] in the ADCK3 gene were reported by Mollet et al. (2008), and Chang et al. (2018) (Mollet et al. 2008; Chang et al. 2018). Mollet et al. (2008) studied a progressive neurological disorder with cerebellar atrophy and seizures in four ubiquinone-deficient patients in three distinct families. In agreement with our study, all the cases showed ubiquinone deficiency in the enzymological studies (Mollet et al. 2008).
Chang et al. (2018) describe two new cases of neurological syndromes due to ADCK3 mutations obtaining outstanding benefits from CoQ10. Despite the remarkable responses in some cases with ataxia and movement disorders (myoclonus, dystonia, tremor), these researchers were not, overall, able to identify variables to predict response to CoQ10 supplementation (Chang et al. 2018). These data are in contrast with our presented case.
In agreement with our data, Hikmat et al. (2016) showed that mutations in the ADCK3 gene can cause a complex ataxia-myoclonus syndrome and acute epileptic encephalopathy with stroke‐like episodes. This finding suggested that ADCK3 mutations can be responsible for differential diagnosis of mitochondrial encephalopathy with stroke‐like cortical involvement. Typically, cases present with a complex neurological phenotype, with cerebellar ataxia as the main manifestation (Hikmat et al. 2016). Liu et al. (2014) declared that mutations in the ADCK3 should be considered a potential cause of unexplained complex neurological syndromes even when cerebellar ataxia is not the major feature. Although the manifestations can start in early childhood or infancy, there are reports of juvenile-onset of CoQ10 deficiency, revealing that age of onset can vary (Liu et al. 2014). CoQ10 replacement therapy resulted in objective and subjective development in the case function and symptoms. Despite the fact that there were also improvements in ataxic symptoms as evaluated using the SARA scale, the most noticeable improvements were in a decrease of myoclonus and speech recovery. Our study declared that WES is a suitable method to detect mutations, mainly in unexplained complex syndromes with high genetic heterogeneity. This finding is in concordance with the study of Liu et al. (2014).
In a similar study, Aure et al. (2004) studied a 7-year follow-up evaluation of a case with CoQ10 deficiency, revealing that CoQ10 defects may cause progressive neurologic disease despite Coenzyme supplementation. Early symptoms of exercise intolerance and hyperlactatemia improved noticeably with substitutive treatment. However, CoQ10 supplementation did not prevent the onset of cerebellar syndrome. A switch to idebenone treatment caused clinical and metabolic worsening, which disappeared with subsequent CoQ10 treatment (Aure et al. 2004). Central hypothyroidism arises from insufficient stimulation of the thyroid gland by TSH, for which secretion or activity can be impaired at the hypothalamic or pituitary levels. Central hypothyroidism should be evaluated in each patient with developmental delay (Konishi et al. 2021). Hypothyroidism is often seen in patients with mitochondrial disorders and ataxia-related phenotypes (Goldstein et al. 2013; Sun et al. 2019). To the best of our knowledge, hypothyroidism has not been reported in patients with disease-causing variants in the ADCK3 gene.
Calculating the ΔΔG values of variants, the I-Mutant2.0 server revealed that p.(Gly272Cys) variant decreases the stability of COQ8A protein (ΔΔG = − 0.89, ΔΔG < 0: decrease stability). 3D structure of the protein and difference between side chains shown in Fig. 3B. Evolutionary conservation analysis was performed using UCSC genome browser, showing that Gly at residue 272 of the COQ8A is conserved among different species including rhesus, mouse, zebrafish, elephant, and dog. Also, according to the ConSurf server, Gly272 is a highly conserved amino acid with a conservation scale of 9 out of 9 (Fig. 3C). Based on pathogenic mutation prediction (PMut) analysis, which predicts pathogenicity of all missense variants in the protein, all substitutions at the residue of 272 of COQ8A protein were pathogenic, including Gly to Cys. This substitution was predicted as “disease” with a score of 0.88 (92%) out of 1.00. Pathogenicity prediction was predicted by computational prediction tools. FATHMM-MKL, PROVEAN, and SIFT specified the p.(Gly272Cys) variant as “damaging.” Based on EIGEN and REVEL tools, this variant was “pathogenic.”
Conclusion
The disease-causing variants in the ADCK3 gene cause primary coenzyme Q10 deficiency-4, also known as autosomal recessive spinocerebellar ataxia-9. A small number of variants in the ADCK3 gene may cause EPC. However, there are still several unknown variants, which cause EPC. These variants need to be determined in suspicious patients by genetic studies. There was a significant delay in diagnosis of this patient because of focusing on seizure control rather than prompt genetic testing for refractory seizures with underlying regression and ataxia. Therefore, clinicians should consider genetic testing earlier to instant diagnosis and satisfactory treatment based on exact etiology to prevent further neurologic sequelae.
Availability of Data and Materials
Human variant and pertinent phenotypes have been reported to ClinVar (Submission ID: SUB8911007, Accession ID: SCV001477284).
References
Atmaca MM, Bebek N, Kocasoy-Orhan E, Gürses C (2018) Epilepsia partialis continua: correlation of semiology, outcome and electrophysiologic features 171:143–150
Aure K, Benoist JF, De Baulny HO, Romero NB, Rigal O, Lombes A (2004) Progression despite replacement of a myopathic form of coenzyme Q10 defect 63:727–729
Berbel-Garcia A, Barbera-Farre JR, Etessam JP, Salio AM, Cabello A, Gutierrez-Rivas E, Campos Y (2004) Coenzyme Q 10 improves lactic acidosis, strokelike episodes, and epilepsy in a patient with MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes). 27:187–191
Chang A, Ruiz‐Lopez M, Slow E, Tarnopolsky M, Lang AE, Munhoz RP (2018) ADCK3‐related coenzyme Q10 deficiency: a potentially treatable genetic disease 5:635–639
Chen S, Zhou Y, Chen Y, Gu J (2018) fastp: an ultra-fast all-in-one FASTQ preprocessor 34:i884–i890
Dallner G, Sindelar PJ (2000) Regulation of Ubiquinone Metabolism. Free Rad Biol Med 29:285–294
Fragaki K, Chaussenot A, Benoist JF, Ait-El-Mkadem S, Bannwarth S, Rouzier C, Cochaud C, Paquis-Flucklinger V (2016) Coenzyme Q10 defects may be associated with a deficiency of Q10-independent mitochondrial respiratory chain complexes 49:1–9
Gaaib JN, Nassief AF, Al-Assi A (2011) Simple Salting-out Method for Genomic DNA Extraction from Whole Blood 16:1813–2662
Goldstein AC, Bhatia P, Vento JM (2013) Mitochondrial Disease in Childhood: Nuclear Encoded 10:212–226
Hikmat O, Tzoulis C, Knappskog PM, Johansson S, Boman H, Sztromwasser P, Lien E, Brodtkorb E, Ghezzi D, Bindoff LA (2016) ADCK 3 mutations with epilepsy, stroke‐like episodes and ataxia: a POLG mimic? 23:1188–1194
Jo H, Koh G (2015) & ENGINEERING. Faster single-end alignment generation utilizing multi-thread for BWA 26:S1791–S1796
Khan Z, Arya K, Bollu PCJS (2020) Epilepsia partialis continua
Konishi A, Ida S, Shoji Y, Etani Y, Kawai M (2021) Central hypothyroidism improves with age in very young children with prader-willi syndrome 94:384–391
Lagier-Tourenne C, Tazir M, López LC, Quinzii CM, Assoum M, Drouot N, Busso C, Makri S, Ali-Pacha L, Benhassine T, Anheim M (2008) ADCK3, an ancestral kinase, is mutated in a form of recessive ataxia associated with coenzyme Q10 deficiency 82:661–672
Lamperti C, Naini A, Hirano M, De Vivo DC, Bertini E, Servidei S, Valeriani M, Lynch D, Banwell B, Berg M, Dubrovsky T (2003) Cerebellar ataxia and coenzyme Q10 deficiency 60:1206–1208
Li H, Handsaker B, Wysoker A, Fennell T, Ruan J, Homer N, Marth G, Abecasis G, Durbin RJB (2009) The sequence alignment/map format and samtools 25:2078–2079
Li MC, Symmonds M, Pretorius PM, Sheerin F, Nithi K, Hofer M, Poulton J, Sen A (2020) Very late-onset mitochondrial cytopathy featuring epilepsia partialis continua and bilateral deafness: a case report 76:153–155
Liu YT, Hersheson J, Plagnol V, Fawcett K, Duberley KE, Preza E, Hargreaves IP, Chalasani A, Laurá M, Wood NW, Reilly MM (2014) Autosomal-recessive cerebellar ataxia caused by a novel ADCK3 mutation that elongates the protein: clinical, genetic and biochemical characterisation 85:493–498
Mameniškienė R, Wolf P (2017) Epilepsia partialis continua: a review 44:74–80
Mancuso M, Orsucci D, Volpi L, Calsolaro V, Siciliano G (2010) Coenzyme Q10 in neuromuscular and neurodegenerative disorders 11:111–121
Mohammadi P, Heidari M, Ashrafi MR, Mahdieh N, Garshasbi M (2021b) A novel homozygous missense variant in the NAXE gene in an Iranian family with progressive encephalopathy with brain edema and leukoencephalopathy pp. 1–10
Mohammadi P, Salehi Siavashani E, Mohammadi MF, Bahramy A, Almadani N, Garshasbi M (2021c) Whole‐exome sequencing identified first homozygous frameshift variant in the COLEC10 gene in an Iranian patient causing 3MC syndrome type 3 9:e1834
Mollet J, Delahodde A, Serre V, Chretien D, Schlemmer D, Lombes A, Boddaert N, Desguerre I, De Lonlay P, De Baulny HO, Munnich A (2008) CABC1 gene mutations cause ubiquinone deficiency with cerebellar ataxia and seizures 82:623–630
Nykamp K, Anderson M, Powers M, Garcia J, Herrera B, Yuan-Yuan H, Kobayashi Y, Patil N, Thusberg J, Westbrook M, Aguilar S (2017) Sherloc: a comprehensive refinement of the ACMG–AMP variant classification criteria 19:1105–1117
Potgieter M, Pretorius E, Pepper MS (2013) Primary and secondary coenzyme Q10 deficiency: the role of therapeutic supplementation 71:180–188
Ren S, Bertels K, Al-Ars Z (2018) Efficient Acceleration of the Pair-Hmms Forward Algorithm for Gatk Haplotypecaller on Graphics Processing Units 14:1176934318760543
Ribeiro JJ, Sousa M, Teotónio R, Bento C, Sales F (2015) Epilepsia Partialis Continua of the Abdominal Muscles Due to Cerebrovascular Disease 17:72–76
Sun M, Johnson AK, Nelakuditi V, Guidugli L, Fischer D, Arndt K, Ma L, Sandford E, Shakkottai V, Boycott K, Chardon JW (2019) Targeted exome analysis identifies the genetic basis of disease in over 50% of patients with a wide range of ataxia-related phenotypes 21:195–206
Supernat A, Vidarsson OV, Steen VM, Stokowy T (2018) Comparison of three variant callers for human whole genome sequencing 8:1–6
Tavasoli AR, Memar EH, Ashrafi MR, Hosseini SM, Haghighi R, Ghabeli H, Pourbakhtyaran E, Rasoulinezhad M, Mohammadi P, Heidari M (2022) Primary and secondary microcephaly, global developmental delay, and seizure in two siblings caused by a novel missense variant in the ZNF335 gene pp. 1–11
Thormann A, Halachev M, McLaren W, Moore DJ, Svinti V, Campbell A, Kerr SM, Tischkowitz M, Hunt SE, Dunlop MG, Hurles ME (2019) Flexible and scalable diagnostic filtering of genomic variants using G2P with Ensembl VEP 10:1–10
Thorvaldsdóttir H, Robinson JT, Mesirov JP (2013) Integrative Genomics Viewer (IGV): high-performance genomics data visualization and exploration 14:178–192
Valentin A, Ughratdar I, Cheserem B, Morris R, Selway R, Alarcon G (2015) Epilepsia partialis continua responsive to neocortical electrical stimulation 56:e104–e109
Acknowledgements
We thank all participants in this research. The authors are especially thankful to the patient and his parents who took part in this study and also the personnel of the Children’s Medical Center for supporting us through the research. The grant of this study was from NIMAD proposal No 971846.
Funding
This study was funded by NIMAD proposal No 971846 received by Professor. Mahmoud Reza Ashrafi.
Author information
Authors and Affiliations
Contributions
PM and MH conceived and designed the experiments. RSB, MRA, RH, AT, EP, and HGH conducted the experiments. PM, MH, ZR, RH, and NM analyzed and interpreted the data. RH and MRA contributed reagents/ materials/analysis tools. PM, RH, and MH wrote the paper. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics Approval and Consent to Participate
Written consent was obtained from parents as legal guardians of the proband. This study was approved by the local ethics committee of the National Institute for Medical Research Development (NIMAD) of Iran (Ethics ID: IR.NIMAD.REC.1397.508). Therefore, this research has been done in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ashrafi, M.R., Haghighi, R., Badv, R.S. et al. Epilepsia Partialis Continua a Clinical Feature of a Missense Variant in the ADCK3 Gene and Poor Response to Therapy. J Mol Neurosci 72, 1125–1132 (2022). https://doi.org/10.1007/s12031-022-01993-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12031-022-01993-0