
Abstract
Background
Cholangiocarcinoma is a relatively rare invasive carcinoma that arises from the lining of the gallbladder and bile ducts and carries a very poor prognosis (Chabner BA et al. Harrison’s manual of oncology. New York: McGraw-Hill; 2008). Its incidence in the US is on average one case per 100,000 persons per year and may be increasing in frequency (Darwin PE. Cholangiocarcinoma [Web page]. emedicine from WebMD, http://www.emedicine.com/med/TOPIC343.HTM, accessed July 22, 2008). Currently, the only treatment option that offers a potential for cure is radical surgical resection. Typically, only 30% of patients qualify for this, while, for the remainder, treatment is only palliative (Chabner BA et al. Harrison’s manual of oncology. New York: McGraw-Hill; 2008). Sorafenib is an oral-targeted agent that acts as a multikinase inhibitor and competitively inhibits the Raf, vascular endothelial growth factor receptor 2 (VEGFR2), VEGFR3, platelet-derived growth factor receptor beta, Flt3, and C-KIT receptors (Chabner BA et al. Harrison’s manual of oncology. New York: McGraw-Hill; 2008). It has demonstrated effective clinical antitumor activity in both renal cell and inoperable hepatocellular carcinoma gaining Food and Drug Administration approval for the latter carcinoma in November 2007. Its role in advanced cholangiocarcinoma is yet to be defined.
Methods
Two female patients with biopsy-proven multifocal moderately differentiated cholangiocarcinoma received single-agent sorafenib at standard doses.
Results
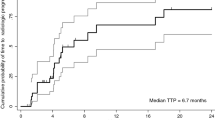
Both patients derived benefit in the form of disease stabilization with negligible cancer-related side effects lasting 4+ months. Sorafenib side effects were relatively modest aside for rash in one patient.
Conclusions
Sorafenib use resulted in effective palliation in two patients with advanced cholangiocarcinoma. Larger phase 2 trials, will be necessary to confirm this initial observation.
Similar content being viewed by others


References
Thongprasert S. The role of chemotherapy in cholangiocarcinoma, 2005. Ann Oncol 2005;16(supplement2):ii93–6. doi:10.1093/annonc/mdi712.
Myung AL, In SW, Jin-Hyoung K, Young SH, Kyung SL. Gemcitabine and cisplatin combination chemotherapy in intrahepatic cholangiocarcinoma as second-line treatment: report of four cases. Jpn J Clin Oncol 2004;34(9):547–50. doi:10.1093/jjco/hyh099.
Nehls HO, Hartmann JT, Hofheinz R-D, et al. Capecitabine plus oxaliplatin as first-line treatment in patients with advanced biliary system adenocarcinoma: a prospective multicentre phase II trial. Br J Cancer 2008;98:309–15. doi:10.1038/sj.bjc.6604178.
Huether A, Höpfner M, Baradari V, Schuppan D, Scherübl H. Sorafenib alone or as combination therapy for growth control of cholangiocarcinoma, 2007. Biochem Pharmacol 2007;73(9):1308–17, 1 May.
Chabner BA, Lynch TJ Jr, Longo DL. Harrison’s manual of oncology. New York: McGraw-Hill; 2008.
Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. NEJM 2008;359:378–90. doi:10.1056/NEJMoa0708857.
Abou-Alfa GK, Schwartz L, Ricci S, et al. Phase II study of sorafenib in patients with advanced hepatocellular carcinoma, 2006. J Clin Oncol 2006;24(26):4293–300, ©(September 10) 2006 American Society of Clinical Oncology.
Yu C, Bruzek LM, Meng XW, Gores GJ, et al. The role of Mcl-1 downregulation in the proapoptotic activity of the multikinase inhibitor BAY 43-9006. Oncogene 2005;24(46):6861–9. ISSN 0950-9232 [9 page(s) (article)] (37 ref).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
LaRocca, R.V., Hicks, M.D., Mull, L. et al. Effective Palliation of Advanced Cholangiocarcinoma with Sorafenib: a Two-Patient Case Report. J Gastrointest Canc 38, 154–156 (2007). https://doi.org/10.1007/s12029-008-9028-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-008-9028-9