
Abstract
Background
Thromboembolic events and anticoagulation-associated bleeding events represent frequent complications following cardiac mechanical valve replacement. Management guidelines regarding the timing for resuming anticoagulation therapy following a surgically treated subdural hematoma (SDH) in patients with mechanical valves remains to be determined.
Objective
To determine optimal anticoagulation management in patients with mechanical heart valves following treatment of SDH.
Methods
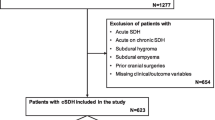
Outcomes were retrospectively reviewed for 12 patients on anticoagulation therapy for thromboembolic prophylaxis for mechanical cardiac valves who underwent surgical intervention for a SDH at the Johns Hopkins Hospital between 1995 and 2010.
Results
The mean age at admission was 71 years. All patients had St. Jude’s mechanical heart valves and were receiving anticoagulation therapy. All patients had their anticoagulation reversed with vitamin K and fresh frozen plasma and underwent surgical evacuation. Anticoagulation was withheld for a mean of 14 days upon admission and a mean of 9 days postoperatively. The average length of stay was 19 days. No deaths or thromboembolic events occurred during the hospitalization. Average follow-up time was 50 months, during which two patients had a recurrent SDH. No other associated morbidities occurred during follow-up.
Conclusion
Interruptions in anticoagulation therapy for up to 3 weeks pose minimal thromboembolic risk in patients with mechanical heart valves. Close follow-up after discharge is highly recommended, as recurrent hemorrhages can occur several weeks after the resumption of anticoagulation.
Similar content being viewed by others


References
Salem DN, O’Gara PT, Madias C, et al. Valvular and structural heart disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):593S–629S.
Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52(13):e1–142.
Fang MC, Go AS, Chang Y, et al. Death and disability from warfarin-associated intracranial and extracranial hemorrhages. Am J Med. 2007;120(8):700–5.
Rosand J, Eckman MH, Knudsen KA, et al. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med. 2004;164(8):880–4.
Flaherty ML, Kissela B, Woo D, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. 2007;68(2):116–21.
Freeman WD, Aguilar MI. Management of warfarin-related intracerebral hemorrhage. Expert Rev Neurother. 2008;8(2):271–90.
Eckman MH, Rosand J, Knudsen KA, et al. Can patients be anticoagulated after intracerebral hemorrhage? A decision analysis. Stroke. 2003;34(7):1710–6.
Claassen DO, Kazemi N, Zubkov AY, et al. Restarting anticoagulation therapy after warfarin-associated intracerebral hemorrhage. Arch Neurol. 2008;65(10):1313–8.
Cannegieter SC, Rosendaal FR, Wintzen AR, et al. Optimal oral anticoagulant therapy in patients with mechanical heart valves. N Engl J Med. 1995;333(1):11–7.
Ananthasubramaniam K, Beattie JN, Rosman HS, et al. How safely and for how long can warfarin therapy be withheld in prosthetic heart valve patients hospitalized with a major hemorrhage? Chest. 2001;119(2):478–84.
Jeffree RL, Gordon DH, Sivasubramaniam R, et al. Warfarin related intracranial haemorrhage: a case-controlled study of anticoagulation monitoring prior to spontaneous subdural or intracerebral haemorrhage. J Clin Neurosci. 2009;16(7):882–5.
Kawamata T, Takeshita M, Kubo O, et al. Management of intracranial hemorrhage associated with anticoagulant therapy. Surg Neurol. 1995;44(5):438–42. discussion 443.
Phan TG, Koh M, Wijdicks EF. Safety of discontinuation of anticoagulation in patients with intracranial hemorrhage at high thromboembolic risk. Arch Neurol. 2000;57(12):1710–3.
Wijdicks EF, Schievink WI, Brown RD, et al. The dilemma of discontinuation of anticoagulation therapy for patients with intracranial hemorrhage and mechanical heart valves. Neurosurgery. 1998;42(4):769–73.
Disclosure
The authors received no financial support in conjunction with the generation of this submission.
Author information
Authors and Affiliations
Corresponding author
Additional information
Anubhav G. Amin and Julie Ng contributed equally to this study.
Rights and permissions
About this article
Cite this article
Amin, A.G., Ng, J., Hsu, W. et al. Postoperative Anticoagulation in Patients with Mechanical Heart Valves Following Surgical Treatment of Subdural Hematomas. Neurocrit Care 19, 90–94 (2013). https://doi.org/10.1007/s12028-012-9704-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9704-2