
Abstract
Background
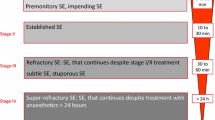
There were nearly 700,000 patients in the United States in 2010 living with brain tumor diagnoses. The incidence of seizures in this population is as high as 70% and is historically difficult to control. Approximately 30–40% of brain tumors patients who present with status epilepticus (SE) will not respond to typical therapy consisting of benzodiazepines and phenytoin (PHT), resulting in patients with refractory status epilepticus (RSE). RSE is usually treated with anesthetic doses of propofol or midazolam infusions. This therapy can have significant risk, particularly in patients with cancer.
Methods
A retrospective chart review was performed on 23 patients with primary or metastatic brain tumors whose SE was treated with intravenous PHT, levetiracetam (LEV), and oral pregabalin (PGB).
Results
In all the patients under study, PHT or LEV was used as first-line therapy. PGB was typically used as third-line treatment. The median daily dose of PGB was 375 mg (usually divided BID or TID), and the median daily dose of LEV 3000 mg (usually divided BID). Cessation of SE was seen in 16/23 (70%) after administration of PHT, LEV, and PGB. SE was aborted, on average, 24 h after addition of the third antiepileptic drug. Only one patient in the responder group required intubation. Mortality rate was zero in the responder group. No adverse reactions to this medication regimen were observed.
Conclusion
Our study suggests that the administration of PHT, LEV, and PGB in brain tumor patients with RSE is safe and highly effective.

Similar content being viewed by others

References
Porter KR, et al. Prevalence estimates for primary brain tumors in the United States by age, gender, behavior, and histology. Neuro Oncol. 2010;12(6):520–7.
Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935–1984. Epilepsia. 1993;34(3):453–68.
Morris HH, et al. Chronic intractable epilepsy as the only symptom of primary brain tumor. Epilepsia. 1993;34(6):1038–43.
Hildebrand J, et al. Epileptic seizures during follow-up of patients treated for primary brain tumors. Neurology. 2005;65(2):212–5.
Moots PL, et al. The course of seizure disorders in patients with malignant gliomas. Arch Neurol. 1995;52(7):717–24.
Aminoff MJ, Simon RP. Status epilepticus. Causes, clinical features and consequences in 98 patients. Am J Med. 1980;69(5):657–66.
DeLorenzo RJ, et al. A prospective, population-based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology. 1996;46(4):1029–35.
Knake S, et al. Incidence of status epilepticus in adults in Germany: a prospective, population-based study. Epilepsia. 2001;42(6):714–8.
Sagduyu A, Tarlaci S, Sirin H. Generalized tonic-clonic status epilepticus: causes, treatment, complications and predictors of case fatality. J Neurol. 1998;245(10):640–6.
Claassen J, et al. Predictors of functional disability and mortality after status epilepticus. Neurology. 2002;58(1):139–42.
Towne AR, et al. Determinants of mortality in status epilepticus. Epilepsia. 1994;35(1):27–34.
Fountain NB. Status epilepticus: risk factors and complications. Epilepsia. 2000;41(Suppl 2):S23–30.
Claassen J, Hirsch LJ, Mayer SA. Treatment of status epilepticus: a survey of neurologists. J Neurol Sci. 2003;211(1–2):37–41.
Lowenstein DH, Alldredge BK. Status epilepticus. N Engl J Med. 1998;338(14):970–6.
Knake S, et al. Intravenous levetiracetam in the treatment of benzodiazepine refractory status epilepticus. J Neurol Neurosurg Psychiatry. 2008;79(5):588–9.
Moddel G, et al. Intravenous levetiracetam: a new treatment alternative for refractory status epilepticus. J Neurol Neurosurg Psychiatry. 2009;80(6):689–92.
Rossetti AO, Bromfield EB. Levetiracetam in the treatment of status epilepticus in adults: a study of 13 episodes. Eur Neurol. 2005;54(1):34–8.
Gaitanis JN, Drislane FW. Status epilepticus: a review of different syndromes, their current evaluation, and treatment. Neurologist. 2003;9(2):61–76.
Novy J, Rossetti AO. Oral pregabalin as an add-on treatment for status epilepticus. Epilepsia. 2010;51(10):2207–10.
Ben-Menachem E. Pregabalin pharmacology and its relevance to clinical practice. Epilepsia. 2004;45(Suppl 6):13–8.
Cranford RE, et al. Intravenous phenytoin: clinical and pharmacokinetic aspects. Neurology. 1978;28(9 Pt 1):874–80.
Lynch BA, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci USA. 2004;101(26):9861–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Swisher, C.B., Doreswamy, M., Gingrich, K.J. et al. Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain Tumors. Neurocrit Care 16, 109–113 (2012). https://doi.org/10.1007/s12028-011-9626-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-011-9626-4