
Abstract
Background
The Surgical Trial in Intracerebral Hemorrhage (STICH) showed no overall benefit from early surgery compared with initial conservative treatment for intracerebral hemorrhage (ICH). We hypothesized that the STICH trial findings would lead to a reduction in the rates of surgery for ICH in the United States. Using a national hospital database, we determined trends in surgery for ICH before and after publication of STICH. We also determined trends in ICH mortality during the study period.
Methods
We queried the Premier database for all ICH-related admissions (denominator) using the ICD-9 codes 431 and 432.9, and craniotomy (numerator) with CPT procedure codes 01.2, 01.24, 01.25, 01.31, 01.39, or 01.59, for fiscal years (FY) 2000—FY2008. Trends in craniotomy and ICH mortality were determined. Change over time was tested using logistic regression.
Results
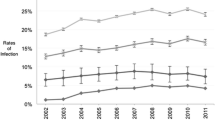
During the study period, 107,590 ICH discharges were identified. A craniotomy procedure code was identified in 7,518 instances (7.0%). Surgical cases were younger and had lower mortality than non-surgical cases. Publication of the STICH trial did not significantly impact the rate of craniotomy for ICH in the United States (P = 0.15). Age-, race-, and gender-adjusted in-hospital ICH mortality decreased steadily during the study period (P < 0.001).
Conclusions
The rate of surgery among ICH discharges in the United States has remained stable in the past decade. While in-hospital ICH mortality decreased, controlled clinical trials are needed to determine which ICH patients would benefit from surgery, and if decreasing in-hospital mortality is associated with decreased longer term mortality and improved functional outcomes.


Similar content being viewed by others


References
Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Circulation. 2007;116(16):e391–413.
Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics—2009 update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008.
Mendelow AD, Gregson BA, Fernandes HM, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. 2005;365(9457):387–97.
Kirkman MA, Mahattanakul W, Gregson BA, Mendelow AD. The effect of the results of the STICH trial on the management of spontaneous supratentorial intracerebral haemorrhage in Newcastle. Br J Neurosurg. 2008;22(6):739–46. Discussion 47.
Gregson BA, Mendelow AD. International variations in surgical practice for spontaneous intracerebral hemorrhage. Stroke. 2003;34(11):2593–7.
Andaluz N, Zuccarello M. Recent trends in the treatment of spontaneous intracerebral hemorrhage: analysis of a nationwide inpatient database. J Neurosurg. 2009;110(3):403–10.
Adeoye O, Woo D, Haverbusch M, et al. Surgical management and case-fatality rates of intracerebral hemorrhage in 1988 and 2005. Neurosurgery. 2008;63(6):1113–7. Discussion 7–8.
Staffa JAGB. Outcome-based evaluation of a method for obtaining U.S. National estimates of inpatient drug utilization. Pharmacoepidemiol Drug Saf. 2003;12:S173.
Broderick J, Brott T, Tomsick T, Tew J, Duldner J, Huster G. Management of intracerebral hemorrhage in a large metropolitan population. Neurosurgery. 1994;34(5):882–7. Discussion 7.
Inagawa T, Ohbayashi N, Takechi A, Shibukawa M, Yahara K. Primary intracerebral hemorrhage in Izumo City, Japan: incidence rates and outcome in relation to the site of hemorrhage. Neurosurgery. 2003;53(6):1283–97. Discussion 97–98.
Morioka J, Fujii M, Kato S, et al. Surgery for spontaneous intracerebral hemorrhage has greater remedial value than conservative therapy. Surg Neurol. 2006;65(1):67–72. Discussion 3.
Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortality after intracerebral hemorrhage. Neurology. 2006;66(8):1182–6.
Diringer MN, Edwards DF. Admission to a neurologic/neurosurgical intensive care unit is associated with reduced mortality rate after intracerebral hemorrhage. Crit Care Med. 2001;29(3):635–40.
Suarez JI, Zaidat OO, Suri MF, et al. Length of stay and mortality in neurocritically ill patients: impact of a specialized neurocritical care team. Crit Care Med. 2004;32(11):2311–7.
Alberts MJ, Latchaw RE, Selman WR, et al. Recommendations for comprehensive stroke centers: a consensus statement from the Brain Attack Coalition. Stroke. 2005;36(7):1597–616.
Acknowledgment
This work was supported by AAMC Grant MM-0971-07/07.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Adeoye, O., Ringer, A., Hornung, R. et al. Trends in Surgical Management and Mortality of Intracerebral Hemorrhage in the United States Before and After the STICH Trial. Neurocrit Care 13, 82–86 (2010). https://doi.org/10.1007/s12028-010-9351-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9351-4