
Abstract
Introduction
Conclusive evidence of cerebral ischemia following head injury has been elusive. We aimed to use 15O and 18Fluorodeoxyglucose positron emission tomography (PET) to investigate pathophysiological derangements following head injury.
Results
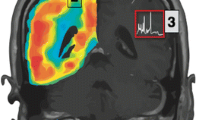
Eight patients underwent PET within 24 h of injury to map cerebral blood flow (CBF), cerebral oxygen metabolism (CMRO2), oxygen extraction fraction (OEF), and cerebral glucose metabolism (CMRglc). Physiological regions of interest (ROI) were generated for each subject using a range of OEF values from very low (<10), low (10–30), normal range (30–50), high (50–70), and critically high (≥70%). We applied these ROIs to each subject to generate data that would examine the balance between blood flow and metabolism across the injured brain independent of structural injury.
Discussion
Compared to the normal range, brain regions with higher OEF demonstrate a progressive CBF reduction (P < 0.01), CMRO2 increase (P < 0.05), and no change in CMRglc, while regions with lower OEF are associated with reductions in CBF, CMRO2, and CMRglc (P < 0.01). Although all subjects demonstrate a decrease in CBF with increases in OEF > 70%, CMRO2 and CMRglc were generally unchanged. One subject demonstrated a reduction in CBF and small fall in CMRO2 within the high OEF region (>70%), combined with a progressive increase in CMRglc.
Conclusions
The low CBF and maintained CMRO2 in the high OEF ROIs is consistent with classical cerebral ischemia and the presence of an ‘ischemic penumbra’ following early head injury, while the metabolic heterogeneity that we observed suggests significant pathophysiological complexity. Other mechanisms of energy failure are clearly important and further study is required to delineate the processes involved.





Similar content being viewed by others


References
Coles JP, Fryer TD, Smielewski P, et al. Incidence and mechanisms of cerebral ischemia in early clinical head injury. J Cereb Blood Flow Metab. 2004;24:202–11.
Coles JP, Fryer TD, Smielewski P, et al. Defining ischemic burden after traumatic brain injury using 15O PET imaging of cerebral physiology. J Cereb Blood Flow Metab. 2004;24:191–201.
Marshall LF, Marshall SB, Klauber MR, et al. A new classification of head injury based on computerized tomography. J Neurosurg. 1991;75:S14–S27.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–4.
Jennett B, Bond M. Assessment of outcome after severe brain damage. A practical scale. Lancet. 1975;1:480–4.
Coles JP, Fryer TD, Coleman MR, et al. Hyperventilation following head injury: effect on ischemic burden and cerebral oxidative metabolism. Crit Care Med. 2007;35:568–78.
Kinahan PE, Rogers JG. Analytic 3D image reconstruction using all detected events. IEEE Trans Nucl Sci. 1989;36:964–8.
Frackowiak RS, Lenzi GL, Jones T, et al. Quantitative measurement of regional cerebral blood flow and oxygen metabolism in man using 15O and positron emission tomography: theory, procedure, and normal values. J Comput Assist Tomogr. 1980;4:727–36.
Lammertsma AA, Baron JC, Jones T. Correction for intravascular activity in the oxygen-15 steady-state technique is independent of the regional hematocrit. J Cereb Blood Flow Metab. 1987;7:372–4.
Herscovitch P, Raichle ME. What is the correct value for the brain-blood partition coefficient for water? J Cereb Blood Flow Metab. 1985;5:65–9.
Phelps ME, Huang SC, Hoffman EJ, et al. Validation of tomographic measurement of cerebral blood volume with C-11-labeled carboxyhemoglobin. J Nucl Med. 1979;20:328–34.
Huang SC, Phelps ME, Hoffman EJ, et al. Noninvasive determination of local cerebral metabolic rate of glucose in man. Am J Physiol. 1980;238:E69–82.
Smielewski P, Coles JP, Fryer TD, et al. Integrated image analysis solutions for pet datasets in damaged brain. J Clin Monit Comput. 2002;17:427–40.
Miller JD. Head injury and brain ischaemia – implications for therapy. Br J Anaesth. 1985;57:120–30.
Becker DP, Miller JD, Ward JD, et al. The outcome from severe head injury with early diagnosis and intensive management. J Neurosurg 1977;47:491–502.
Rosner MJ, Rosner SD, Johnson AH. Cerebral perfusion pressure: management protocol and clinical results. J Neurosurg. 1995;83:949–62.
Patel HC, Menon DK, Tebbs S, et al. Specialist neurocritical care and outcome from head injury. Intensive Care Med. 2002;28:547–53.
Yundt KD, Diringer MN. The use of hyperventilation and its impact on cerebral ischemia in the treatment of traumatic brain injury. Crit Care Clin. 1997;13:163–84.
Coles JP, Fryer TD, Bradley PG, et al. Intersubject variability and reproducibility of (15)O PET studies. J Cereb Blood Flow Metab. 2006;26:48–57.
McLaughlin MR, Marion DW. Cerebral blood flow and vasoresponsivity within and around cerebral contusions. J Neurosurg. 1996;85:871–6.
Diringer MN, Yundt K, Videen TO, et al. No reduction in cerebral metabolism as a result of early moderate hyperventilation following severe traumatic brain injury. J Neurosurg. 2000;92:7–13.
Diringer MN, Videen TO, Yundt K, et al. Regional cerebrovascular and metabolic effects of hyperventilation after severe traumatic brain injury. J Neurosurg. 2002;96:103–8.
Vespa P, Bergsneider M, Hattori N, et al. Metabolic crisis without brain ischemia is common after traumatic brain injury: a combined microdialysis and positron emission tomography study. J Cereb Blood Flow Metab. 2005;25:763–74.
Stein SC, Graham DI, Chen XH, et al. Association between intravascular microthrombosis and cerebral ischemia in traumatic brain injury. Neurosurgery. 2004;54:687–91; discussion 691.
Rodriguez-Baeza A, Reina-de la Torre F, Poca A, et al. Morphological features in human cortical brain microvessels after head injury: a three-dimensional and immunocytochemical study. Anat Rec A Discov Mol Cell Evol Biol. 2003;273:583–93.
Schwarzmaier S, Kim SW, Trabold R, et al. Microcirculatory alterations following experimental TBI. J Neurotrauma. 2006;23:P4.7, p. 769.
Menon DK, Coles JP, Gupta AK, et al. Diffusion limited oxygen delivery following head injury. Crit Care Med. 2004;32:1384–90.
Johnston AJ, Steiner LA, Coles JP, et al. Effect of cerebral perfusion pressure augmentation on regional oxygenation and metabolism after head injury. Crit Care Med. 2005;33:189–95; discussion 255–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abate, M.G., Trivedi, M., Fryer, T.D. et al. Early Derangements in Oxygen and Glucose Metabolism Following Head Injury: The Ischemic Penumbra and Pathophysiological Heterogeneity. Neurocrit Care 9, 319–325 (2008). https://doi.org/10.1007/s12028-008-9119-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-008-9119-2