
Abstract
Introduction
Patients on neurological intensive care units (NICU) who require ventilatory support often suffer from co-existing bulbar dysfunction, either because of their underlying disease or because of their decreased level of consciousness. For this reason, most patients are ventilated through a cuffed tracheostomy tube, which allows a degree of protection from tracheal aspiration of saliva and gastric contents. Patients who are awake often complain of thirst, but traditionally are only offered oral fluids when the cuff of the tracheostomy tube has been deflated. Given that many patients in NICU cannot tolerate cuff deflation, a reliable technique is needed to assess the adequacy of the patient’s swallow and therefore the risk of aspiration when the tracheostomy cuff is inflated.
Methods
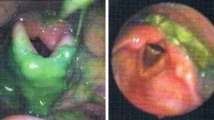
The aim of this feasibility study was to examine the viability of Fibreoptic Endoscopic Evaluation of Swallowing (FEES) as a diagnostic tool to assess the effectiveness of swallowing in four NICU patients with cuffed tracheostomies.
Results
The technique was successful in all of the four patients. One patient was found to have a normal swallow. Two patients were seen to have laryngeal penetration of fluids and one patient aspirated the fluid challenge.
Conclusion
This pilot study has demonstrated the feasibility of using the FEES technique for assessment of swallowing in patients with cuffed tracheostomy tubes; it therefore presents the prospect of allowing earlier drinking in such patients whilst helping confirm the safety of such a strategy.
Article PDF
Similar content being viewed by others


References
Ding R, Logemann J. Swallow physiology in patients with trach cuff inflated or deflated: a retrospective study. Head Neck 2005;27:809–813.
Ajemian M, Nirmul G, Anderson M, Zirlen D, Kwasnik E. Routine fiberoptic endoscopic evaluation of swallowing following prolonged intubation. Arch Surg 2001;136:434–7.
Leder S. Incidence and type of aspiration in acute care patients requiring mechanical ventilation via a new tracheotomy. Chest 2002;122:1721–6.
O’Neil-Pirozzi T, Lisiecki D, Momose K, Connors J, Milliner M. Simultaneous modified barium swallow and blue dye tests: a determination of the accuracy of blue dye test aspiration findings. Dysphagia 2003;18:32–8.
Langmore S. Evaluation of oropharyngeal dysphagia: which diagnostic tool is superior? Curr Opin Otolaryngol Head Neck Surg 2003;11:485–9.
Barquist E, Brown M, Cohn S, Lundy D, Jackowski J. Postextubation fiberoptic endoscopic evaluation of swallowing after prolonged orotracheal intubation: a randomized, prospective trial. Crit Care Med 2001;29:1710–13.
Rosenbek J, Robbins J, Roecker E, Coyle J, Wood J. A penetration-aspiration scale. Dysphagia 1996;11:93–8.
DeVita M, Spierer-Rundback L. Swallowing disorders in patients with prolonged orotracheal intubation or tracheostomy tubes. Crit Care Med 1990;18:1328–30.
Elpern D, Scott M, Petro L, Ries M. Pulmonary aspiration in mechanically ventilated patients with tracheostomies. Chest 1994;105:563–6.
Tolep K, Getch C, Criner G. Swallowing dysfunction in patients receiving prolonged mechanical ventilation. Chest 1996;109:167–72.
Murray J, Langmore S, Ginsberg S, Dostie A. The significance of accumulated oropharyngeal secretions and swallowing frequency in predicting aspiration. Dysphagia 1996;11:99–103.
Acknowledgements
We thank the patients and staff who took part in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McGowan, S.L., Gleeson, M., Smith, M. et al. A pilot study of fibreoptic endoscopic evaluation of swallowing in patients with cuffed tracheostomies in neurological intensive care. Neurocrit Care 6, 90–93 (2007). https://doi.org/10.1007/s12028-007-0024-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-007-0024-x