
Abstract
Background
En bloc resection for treatment of sacral tumors is the approach of choice for patients with resectable tumors who are well enough to undergo surgery, and studies describe patient survival, postoperative complications, and recurrence rates associated with this treatment. However, most of these studies do not provide patient-reported functional outcomes other than binary metrics for bowel and bladder function postresection.
Questions/purposes
The purpose of this study was to use validated patient-reported outcomes tools to compare quality of life based on level of sacral resection in terms of (1) physical and mental health; (2) pain; (3) mobility; and (4) incontinence and sexual function.
Methods
Our analysis included 33 patients (19 men, 14 women) who had a mean age of 53 years (range, 22–72 years) with a quality-of-life survey administered at a mean postoperative followup of 41 months (range, 6–123 months). The majority of patient-reported quality-of-life outcome surveys for this study were taken from the National Institute of Health’s Patient Reported Outcome Measurement Information System (PROMIS) system. To assess physical and mental health, the PROMIS Global Items Survey with physical and mental subscores, Anxiety, and Depression scores were used. Pain outcomes were assessed using PROMIS Pain Intensity and Pain Interference surveys. Patient-reported lower extremity function was assessed using the PROMIS Mobility Survey. Patient-reported quality of life for sexual function was assessed using the PROMIS Sex Interest and Orgasm survey, whereas incontinence was measured using the International Continence Society Voiding and Incontinence scores and the Modified Obstruction and Defecation Score. Surveys were collected prospectively during clinic visits in the postoperative period. Patients were grouped by the level of osteotomy as determined by review of postoperative MRI or CT and half levels were grouped with the more cephalad level. This resulted in the inclusion of total sacrectomy (N = 6), S1 (N = 8), S2 (N = 10), S3 (N = 5), and S4 (N = 4). One-way analysis of variance tests on means or ranks were used to conduct statistical analysis between levels.
Results
Patients with more caudal resections had higher physical health (95% confidence interval [CI] total sacrectomy 36–42 versus S4 50–64, p < 0.001), less intense pain (95% CI total sacrectomy 47–60 versus S4 28–37, p < 0.001), less interference resulting from pain (95% CI total sacrectomy 58–69 versus S4 36–51, p = 0.004), higher mobility (95% CI total sacrectomy 24–46 versus S4 59–59, p = 0.002), and were more functionally able to achieve orgasm (95% CI S1 1–1 versus S4 2.2–5.3, p = 0.043). No difference was found for PROMIS Global Item Mental Health Subscore, Sex Interest, Sex Satisfaction, modified obstruction and defecation score, and International Continence Society Voiding and Incontinence although this could be the result of an inadequate sample size.
Conclusions
Our analysis on patient-reported quality of life based on the level of bony resection in patients who underwent resection for primary sacral tumor indicates that patients with higher resections have more pain and loss of physical function in comparison to patients with lower resections. Additionally, use of the PROMIS outcomes allows for comparisons to normative data.
Level of Evidence
Level III, therapeutic study.
Similar content being viewed by others


Introduction
Surgical resection for malignant bone tumors arising in the sacrum has been shown to be an important component of the therapeutic strategy to achieve local tumor control [1, 6, 20, 21]. However, the sacral nerves control anal sphincter, bladder, and sexual function and their removal can lead to functional loss and presumably a decreased quality of life. Previous studies have demonstrated the functional role of the sacral nerves from a physiologic perspective [7, 9–11, 19]. Other studies have described the symptoms of bowel and bladder dysfunction as reported to the treating clinician [12, 14, 21].
However, patient-reported quality of life and functional outcomes after sacral resection for malignancy are lacking and, to our knowledge, no such reports exist at this time. Surgical resection with negative margins has been shown to improve local control and disease-free survival in primary malignant tumors of the sacrum [1, 6, 20, 21]. Malignant tumors of the sacrum often invade the sacral nerve roots and they are therefore necessarily sacrificed during definitive resection. Several studies have documented the deleterious effects of sacral nerve root resection on the normal physiology of bowel, bladder, and sexual function [7, 9–11, 19]. Other studies have documented the clinical effects of sacral tumor resection as reported in patients’ medical records [3–5, 12, 14]. The level of sacral nerve root resection has been shown to be important and sparing of the S3 nerve root has been reported to allow some bowel, bladder, and sexual function [7, 9–12, 14]. Because the level of nerve root resection is dictated by the location of the tumor if one is attempting to achieve negative margins, patients and clinicians must weigh the improved local control and survival associated with a particular surgical approach against the loss of bowel, bladder, and sexual function also associated with that surgery. Patient-reported outcomes allow for a quantitative assessment of function that is unfiltered by treating clinicians and such normalized data allow for comparison not only between patients, but also with other disease and healthy states [17].
The purpose of this report is to document quality of life and functional outcomes after sacrectomy using validated patient-reported outcome measures for (1) physical and mental health; (2) pain; (3) mobility; and (4) incontinence and sexual function. This information can be used for patient education and allows providers to assess function on a quantitative scale instead of assessing a binary for signs or symptoms such as incontinence.
Patients and Methods
Under the Orthopaedic Oncology Database (institutional review board No. 2013P002411), our orthopaedic oncology department routinely collects patient-reported quality of life and functional outcome data at patient visits. These data are reviewed retrospectively for quality improvement purposes and for studies. The database was queried to identify all patients who underwent surgical resection for a sacral chordoma or sarcoma (primary tumor or recurrence) and had greater than 6 months of postoperative followup at the time of survey administration. If a patient had multiple quality-of-life surveys in the registry, then the most recently completed survey was used. Patients were excluded if their resection involved a sagittal cut through the sacrum rather than a transverse cut. Furthermore, patients were excluded if their tumor involved the ileum or other aspects of the bony pelvis requiring a hemipelvectomy. Patients with postoperative complications such as recurrence, infection, and hardware failure were not excluded from the study. All patients underwent preoperative radiation of 19.8 Gy or 50.4 Gy (based on perceived risk of wound healing complications and the planned wound closure) followed by resection and postoperative radiation boost radiation to bring the radiation dose to the tumor bed to approximately 70.2 Gy as previously described [3–5].
Patients were grouped by the level of osteotomy: total sacrectomy (osteotomy above S1 body), S1 (osteotomy through S1–S2 junction), S2 (osteotomy through S2–S3 junction), S3 (osteotomy through S3–S4 junction), and S4 (osteotomy through S4–S5 junction). Additionally, cuts that occurred between levels were grouped with the more cephalad level; for instance, a half S4 cut was grouped with S3, a half S3 cut was grouped with S2, a half S2 cut was grouped with S1, and a half S1 cut was grouped with total sacrectomy. We classified a high sacrectomy as one that involved S3 (implied loss of S3 nerve roots and above) and a low sacrectomy as one that involved a cut on S4 or below. We chose to classify our patients based on level of bony resection because this can be confirmed by postoperative surveillance imaging. The levels of nerve roots spared in half cuts were not available in all cases for this analysis (Fig. 1).

Illustration shows level of sacral resection by bony cut. Half cuts were grouped with the cephalad level in this analysis.
We identified 33 patients (19 men, 14 women) with a mean age at surgery of 53 years (range, 33–72 years) with a quality-of-life survey administered at a mean postoperative time of 41 months (range, 6–123 months) between February 2012 and February 2014. There were 31 cases of chordoma, one case of osteosarcoma, and one case of chondrosarcoma in the selected patients. Patients were grouped by level of resection to total sacrectomy (six), S1 (eight), S2 (10), S3 (five), and S4 (four; Table 1). We identified eight patients with a stoma, including four in the total sacrectomy group, three in the S1 group, and one in the S2 group.
The patient-reported outcome surveys we use are based on the recommendations of the Sacral Tumor Study Group (STSG). The STSG includes clinicians who have an active interest in sacral and pelvic tumors including orthopaedic oncologists, radiation oncologists, medical oncologists, urologists, gynecologists, and physiatrists. The STSG meets annually to discuss issues pertaining to the care of patients with sacral and pelvic tumors. At the annual meeting in 2011, held at the Mayo Clinic in Rochester, MN, USA, agreement was reached on a set of questionnaires. Our practice follows STSG guidelines and incorporates questionnaires primarily from the National Institutes of Health Patient Reported Outcome Measurement Information System (PROMIS). In this particular analysis we assessed physical and mental health using the PROMIS Global Items Survey with physical and mental subscores (33 of 33 participants), Anxiety (20 of 33 participants), and Depression (20 of 33 participants) scores. Pain outcomes were assessed using PROMIS Pain Intensity (32 of 33 participants) and Pain Interference (32 of 33 participants) surveys. Patient-reported lower extremity function was assessed using the PROMIS Mobility Survey (20 of 33 participants). Patient-reported quality of life for sexual function was assessed using the PROMIS Sex Interest (33 of 33 participants) and the PROMIS Orgasm (15 of 33 participants) survey, whereas incontinence was measured using the International Continence Society Voiding (18 of 33 participants) and Incontinence (30 of 33 participants) scores and the Modified Obstruction and Defecation Score (29 of 33 participants). Of these surveys, the International Continence Society and Modified Obstruction and Defecation Score are the only non-PROMIS questionnaires used. PROMIS surveys are scored using T-scores that are normalized and calibrated to both healthy and sick patients with a sample size of 21,133 respondents in a US patient population [17]. The normalized mean in the PROMIS surveys is set to 50 with a SD of 10 and higher scores indicate more of the metric being studied, ie, a higher anxiety score indicates more anxiety and a higher mobility score indicates more mobility.
Survey data were scored using PROMIS Scoring Manuals and were converted to T-scores where appropriate. Raw scores or percent of the maximum score were used to display the results of the survey in the absence of a scoring manual. Missing data within a specific domain were interpolated using a weighted mean if participants completed half a survey or four questions, whichever was greater, as per PROMIS guidelines. The survey was not scored if these criteria were not met. Data were analyzed using Stata 13.0 (StataCorp LP, College Station, TX, USA) using the Holm-Sidak analysis of variance test to determine if a significant difference (alpha < 0.05) existed between outcomes based on the level of bony cut.
In a post hoc power analysis, adequate power (> 0.8) for the analysis of variance test was met with alpha set at 0.05 for the global items physical subscore (power: 0.99, delta: 1.1), pain intensity (power: 0.95, delta: 0.96), pain interference (power: 0.91, delta: 0.91), mobility (power: 0.97, delta: 1.4), and orgasm (power: 0.94, delta: 1.4) surveys. For reference, a delta of 0.1 is considered small, 0.3 is considered modest, and 0.5 is considered large. The other analyses were underpowered where either the sample size was not large enough to capture a small effect size or no difference exists.
In the Global Items Mental subscore, we observed a delta at 0.58 with a power of 0.68 where a delta of 0.65 or sample size of 45 would have been required to detect an effect. For the Anxiety survey, we observed a delta of 0.65 at a power of 0.49, which would have required a delta of 0.91 or sample size of 35 to detect an effect. For the depression survey, we observed a delta of 0.45 with a power of 0.24, where a delta of 0.9 or a sample size of 65 would have been required to detect an effect. For the International Continence Society (ICS) voiding survey, we observed a delta of 0.55 with a power of 0.31, where a delta of 0.97 or a sample size of 45 would have been required to detect an effect. For the ICS incontinence survey, we observed a delta of 0.57 with a power of 0.6, where a delta of 0.69 or sample size of 45 would have been required to detect an effect. For the Modified Obstruction and Defecation Score (MODS) survey, we observed a delta of 0.45 with a power of 0.38, where a delta of 0.71 or a sample size of 65 would have been required to detect an effect. For the Sex Interest survey, we detected a delta of 0.50 with a power of 0.54, where a delta of 0.65 or a sample size of 55 would have been required to show an effect.
Cohort Details and Eligible Patients
To determine the total number of eligible patients, we queried a clinical database that tracks patient visits. During the 2-year period for data collection, we found 50 potential patients. Of these 50 patients, we had 10 ineligible patients: two patients were nonnative English speakers, two patients had ineligible surgical resection (hemisacrectomy and curettage), five patients were ineligible because their available quality-of-life survey was taken less than 6 months after surgery, and one patient had surgery at an outside hospital. The remaining seven patients were eligible for the study but either opted out of the survey or were missed during screening. As such, we captured 82.5% of patients eligible for our study during the data collection period. None of the patients eligible for the study were lost to clinical followup.
Of the 45 patients who were potentially eligible, 34 had a primary surgery at an outside hospital and 11 had their primary surgery at our institution. After surgery, three patients who had primary surgery at an outside facility and one patient with a primary surgery at our facility had a recurrence with a mean recurrence free survival of 320 months (95% confidence interval [CI], 283–358 months; Fig. 2). In total, there were 11 patients who developed metastases. The three patients who died had a mean survival of 332 months (95% CI, 301–363 months; Fig. 3). One patient treated at our institution developed a radiation-induced sarcoma. The median clinical followup for the eligible group was 103 months (range, 20–355 months).

In our cohort of 45 patients, we observed a mean recurrence-free survival time of 320 months (95% CI, 283–358 months).

In our cohort of 45 patients, we observed a mean survival time of 332 months (95% CI, 301–363 months).
The patients in the included group had an mean age at surgery of 52 years (range, 22–72 years), tumor size of 8.03 cm (SD 4.9 cm), and three of the 33 patients had positive margins, whereas the patients who were missed had an mean age of 58 years (range, 38–72 years), tumor size of 11.9 cm (SD 7.4 cm), and four patients had positive margins. There were seven males and five females in the eligible group missing quality-of-life data. A rank-sum test was not statistically significant when comparing the included quality-of-life cohort and the missed cohort for age (p = 0.162), sex (p = 0.976), margin status (p = 0.052), or tumor size (p = 0.078).
Results
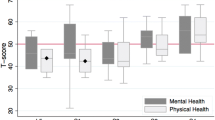
For our primary endpoint of physical and mental function, the Global Item Physical subscore indicated that patients with a high sacral resection had lower function relative to patients with a low resection (delta: 1.1, power: 0.99, p < 0.001; Table 2). A subgroup analysis detected an effect between total sacrectomy (mean, 39; SD, 2.9; 95% CI, 36–42) versus S2 (mean, 49; SD, 5.9; 95% CI, 45–53; p = 0.0013) as well as S1 (mean, 41; SD, 5.8; 95% CI, 36 -46) versus S4 (mean, 57; SD, 4.6; 95% CI, 50–64; p < 0.001) and total sacrectomy (mean, 39; SD, 2.98; 95% CI, 36–42) versus S4 (mean, 57; SD, 4.6; 95% CI, 50–64; p < 0.001) where this difference was greater than 1 SD with respect to a difference in T-scores. The S4 group also had higher physical health than the general population. However, no effect was detected between groups in the Global Mental health (delta: 0.58, power: 0.68, p = 0.078) (Fig. 4), Anxiety (delta: 0.65, power: 0.49, p = 0.225) (Fig. 5), or Depression (delta: 0.45, power: 0.24, p = 0.572) (Fig. 6) surveys (Table 2).

The PROMIS Global Items Survey showed a significant difference between physical health by level of resection (p < 0.001) where lower sacrectomies had better outcomes, but there was no significant difference in mental health outcomes. A T-score of 50 (SD 10) represents the PROMIS population mean for the United States and a higher score indicates more physical or mental health.

The PROMIS Anxiety Survey showed no significant difference between groups based on level of resection. A T-score of 50 (SD 10) represents the PROMIS population mean for the United States and a higher score indicates more anxiety.

The PROMIS Depression Survey showed no significant difference between groups based on level of resection. A T-score of 50 (SD 10) represents the PROMIS population mean for the United States and a higher score indicates more depression.
Analysis of patient-reported pain outcomes revealed that higher sacral cuts led to more intense pain (delta: 0.96, power: 0.99, p = 0.001) and more interference from pain (delta: 0.91, power: 0.98, p = 0.002) than lower sacral cuts (Table 2). In the Pain Intensity survey, subgroup analysis revealed differences between S3 (mean, 46; SD, 6.3; 95% CI, 38–53) versus S4 (mean, 32; SD, 2.8; 95% CI, 28–37; p = 0.043), S2 (mean, 44; SD, 6.8; 95% CI, 40–49) versus S4 (mean, 32; SD, 2.8; 95% CI, 28–37; p = 0.039), S1 (mean, 49; SD, 8.9; 95% CI, 41–57) versus S4 (mean, 32; SD, 2.8; 95% CI, 28–37; p = 0.005), and total sacrectomy (mean, 53; SD, 6.1; 95% CI, 47–60) versus S4 (mean, 32; SD, 2.8; 95% CI, 28–37; p < 0.001). The mean difference between these groups was greater than 1 SD, and the difference between total sacrectomy and S4 was greater than 2 SDs (Fig. 7). Pain Interference also revealed that higher sacral cuts led to more interference from pain than a lower cut (delta: 0.91, power: 0.98, p = 0.002); however, subgroup analysis only revealed an effect in the total sacrectomy (mean, 63; SD, 5.5; 95% CI, 48–69) versus S4 (mean, 44; SD, 4.8; 95% CI, 36–51; p = 0.004) and S1 (mean, 61; SD, 6.8; 95% CI, 55–67) versus S4 (mean, 44; SD, 4.8; 95% CI, 36–51; p = 0.01) groups, where both comparisons approached 2 SDs of difference (SD, 19.9 and 17.4, respectively) (Fig. 7). Patients who had resections at S4 and below had a mean pain score that was lower than that of the general population (Table 2).

The PROMIS Pain Intensity and Interference surveys showed a significant difference between groups based on level of resection at p = 0.001 and p = 0.002, respectively, where patients with lower resections reported less pain. A T-score of 50 (SD 10) represents the PROMIS population mean for the United States and a higher score indicates more pain. Here, we observe that patients with cuts at S4 and below have lower average pain than the PROMIS national average.
With regard to patient mobility, patients retained increasing mobility function with more caudal bony cuts (delta: 1.4, power: 0.99, p = 0.001; Table 2). Subgroup analysis revealed a mean difference of over 2 SDs on the PROMIS scale between total sacrectomy (mean, 35; SD, 4.5; 95% CI, 24–46) and S4 (mean, 59; SD, 0; 95% CI, 59–59; p = 0.002) and a mean difference of over 1.5 SDs for total sacrectomy (mean, 35; SD, 4.5; 95% CI, 24–46) versus S2 (mean, 42; SD, 7.4; 95% CI, 31–54; p = 0.01) and for S1 (mean, 42; SD, 7.1; 95% CI, 31–54) versus S4 (mean, 59; SD, 0; 95% CI, 59–59; p = 0.02) (Fig. 8).

The PROMIS Mobility Survey showed a significant difference between groups based on level of resection (p = 0.001), where patients with lower sacrectomies had more mobility. A T-score of 50 (SD 10) represents the PROMIS population mean for the United States and a higher score indicates more mobility. Here, we observe that patients with cuts at S4 and below have lower average mobility than the PROMIS national average.
With regard to sexual function, patients reported increased ability to have a satisfying orgasm with a more caudal resection (delta: 1.4, power: 0.93, p = 0.012; Table 2) (Fig. 9). There was no observed difference in groups for the sex interest survey (delta: 0.50, power: 0.53, p = 0.168) (Fig. 10). The S4 group here had a similar level of sexual interest as the general population (mean, 59.2; SD, 5.72; 95% CI, 50–68) (Table 2). No differences were observed linking caudal bony cuts to increased function for ICS Voiding (delta: 0.55, power: 0.31, p = 0.454), ICS Incontinence (delta: 0.56, power: 0.24, p = 0.125) (Fig. 11), and the MODS (delta: 0.45, power: 0.38, p = 0.332) (Fig. 12).

The PROMIS Orgasm Survey showed a significant difference between groups based on level of resection (p = 0.012), where patients with lower sacrectomies were more able to have a functional orgasm. Raw scores were used for this survey; thus, no comparison to the PROMIS national average can be made.

The PROMIS Sex interest Survey showed no significant difference between groups based on level of resection. A T-score of 50 (SD 10) represents the PROMIS population mean for the United States and a higher score indicates more interest in sex. Here we observe that patient interest in sex for all groups remains within 1 SD of the PROMIS national average of 50 after sacral resection.

The ICS Voiding and Incontinence surveys show no statistical difference between groups. This can be attributed to our small sample size.

The MODS survey shows no significant difference between groups. This can be attributed to our small sample size.
Discussion
Previous reports of function after sacral resection have focused on whether bowel, bladder, and sexual function are lost owing to the vital role the sacral nerves play in their normal physiology and describe ambulatory status by the use of assistive devices [7, 9–12]. Although these metrics provide some means for comparisons between patients, their utility is limited in contrast to patient-reported outcomes, especially for educating patients on expectations of postoperative function. The purpose of this study is to use validated patient-reported outcomes to describe postoperative function from the patient’s perspective and make comparisons to PROMIS normative data comprised of 21,233 patients from the United States [17]. This study demonstrates that patients undergoing caudal sacral resection have better quality of life, function, and pain levels than those undergoing more cephalad sacral resection, where distal sacral resection, at or below S4, was noted to have quality-of-life and functional levels at or above PROMIS normative data. This information will be useful for patients and their healthcare providers when considering treatment options and for patient education on expectations for postoperative function.
There are several methodological limitations with this report. The first is that we have no presurgical outcome measures because the study was started after most of these patients underwent surgery. It is possible that some of our patients had poor quality of life and function before surgery owing to the impact of the tumor on their quality of life, pain levels, and bowel, bladder, and sexual function. We are currently collecting these outcomes preoperatively for future studies. Second, although we discovered many major findings, we did not have enough power to determine whether many of our no-difference findings were related to insufficient statistical power or sample size. For instance, in the Global Items Mental subscore, we observed a delta at 0.58 with a power of 0.68 where a delta of 0.65 or sample size of 45 would have been required to detect an effect. Thus, a large effect size was present in this and other outcomes, but no effect was detected in the analysis as a result of our small sample size. A larger study is currently underway to help answer this question. Third, the patients did not answer the patient-reported outcomes at a uniform time period after surgery. Although the average time of survey administration was 41 months after surgery, the difference may impact the answers provided by the patients and potentially confound results. Moving forward, we are collecting data at standardized preoperative and multiple postoperative visits to make more uniform comparisons.
With regard to our primary outcome for patient-reported mental health outcomes, overall mental health as well as anxiety and depression were not significantly different between groups. However, these data are spread within a SD of the PROMIS-normalized patient mean of 50 indicating that patients in our sample are not faring much worse than the general public. Better physical function and mobility are both strongly correlated with low sacrectomy as opposed to high sacrectomy. Patients undergoing high sacrectomy may have sciatic nerve dysfunction, which would impact function and mobility. In particular, sacrectomy above the S1-S2 junction renders the sacrum unable to withstand physiologic forces, which often necessitates lumbar-pelvic instrumentation, which may also impact function and mobility [2, 6, 8, 13, 15, 16, 20]. Previous studies have characterized patient loss of sensory and motor deficiencies by describing use of assistive devices required for mobility or by using provider-reported outcomes detailing the degree of function [7, 9–12, 14, 18, 22]. Although these methods provide a means for comparison and the results also showed more loss of function with higher sacrectomies, our use of patient-reported outcomes allows for comparison between groups from the patient’s perspective. Additionally, comparing our outcomes in this population with PROMIS normalized data shows that patients with lower sacrectomy have general physical health and mobility that is within a SD or on par with the general population. Before the use of PROMIS data, this comparison would have been unfeasible.
In our secondary outcome describing patient-reported pain levels, analysis revealed a striking difference between higher and lower sacrectomy, where the comparison between patients with high and low sacrectomy versus normative PROMIS data offers the most insight. Patients with high sacrectomy experience chronic pain that likely influences other aspects of their lives. Most patients who consent to undergo high sacrectomy do so with the understanding that bowel, bladder, and sexual function will be affected. However, one must add chronic pain to the side effects of high sacrectomy to fully inform a patient of potential surgical outcomes. This finding is in contrast to the patients with lower sacrectomy, who reported pain levels lower than normative PROMIS data involving 21,233 patients [17]. It is unclear why patients with lower sacrectomy reported better pain scores than the national average, but the scores may reflect the fact that the tumor had caused the patients’ pain and postoperatively they are relatively pain-free with close to normal function.
Previous reports have emphasized the importance of the S3 nerve root in maintaining bowel, bladder, and sexual function [7–9, 12, 14]. We classified our patients based on level of bony resection because this can be confirmed by postoperative surveillance imaging as opposed to level of nerve root resection, which was not consistently reported in the operative notes. Although we cannot characterize the specific role of the S3 nerve root on patient-reported outcomes in this study, it is important to note that disruption of the normal neurophysiology of bowel, bladder, and sexual function can occur by interruption of the hypogastric plexus during mobilization of the great vessels of the pelvis during anterior sacral approaches. Bowel, bladder, and sexual dysfunction can also occur after ligation of the pudendal nerve or its branches even if the S3 nerve root is spared during sacrectomy. The S3 nerve root likely plays a crucial role in normal function, although loss of bowel, bladder, and sexual function can occur through mechanisms other than sacral root ligation as well. Our study shows that lower sacral resection is less likely to lead to neurologic dysfunction. Lower sacral resection often does not require an anterior approach, which decreases the likelihood of interrupting the hypogastric plexus. In addition, lower sacral resection often allows sparing of the S3 nerve root. Therefore, we theorize that when the S3 nerve roots and the pudendal nerve are left intact, good functional outcomes can be expected.
Patients remained interested in sex, particularly after middle and lower sacrectomy, and sexual satisfaction exceeded normative data for patients undergoing low sacrectomy. Furthermore, the ability to achieve an orgasm was better in patients who had lower sacrectomy. Patients with middle and lower sacrectomy maintained sexual function, whereas patients undergoing higher sacrectomy did not have the same interest or satisfaction with sexual activity. Gunterberg and Petersen reported that the S2 nerve root was implicated in erectile function in men and that bilateral S3-S5 nerve root sacrifice in a subset of women did not affect sexual function [11]. In addition Wuisman et al reported that all patients in their study had saddle-like anesthesia and were left with no sexual function after total sacrectomy [22]. Although these data were based on smaller sample sizes than our data, it is difficult to advise a patient on their prognosis using this information. Although our data are also limited at this time, we believe that there is much higher utility in educating patients on postoperative expectations based on the PROMIS responses of previous respondents as well as a comparison of this information to normalized data.
The importance of patient-reported outcomes is revealed in this pilot study when comparing groups of patients and also comparing patients with normalized PROMIS data [17]. Although the results of this study are not meant to be conclusive, this method of reporting may help frame a discussion of expected outcomes after sacrectomy, which could help patients prepare mentally and physically before surgery. Furthermore, understanding expected functional outcomes may help patients be better informed when discussing treatment options. Our study helps to frame the conversation about expected functional outcomes after sacral resection. Patients with distal sacral resection can expect to have dramatically different functional outcomes when compared with patients undergoing proximal sacrectomy and patients with proximal sacrectomy often have a much higher level of pain months or even years after surgery. This pilot study analyzing patient-reported outcomes after sacrectomy reports improved physical function, mobility, pain levels, and sexual function in patients undergoing distal sacrectomy versus patients undergoing higher sacrectomy. Patients undergoing distal sacrectomy scored better than the national average in several functional measures. The data reported here can be used by clinicians and patients to help better understand and prepare for the impact of sacrectomy when treating sacral chordomas.
Although these data represent the experiences of patients at one center, we are currently working with the other members of the sacral tumor study group to pool our patient population to be able to add power to several underpowered analyses. In addition, this work also serves as the basis for our work on an analysis of the survey responses in this patient population to develop a more robust and reliable assessment tool for both patients and clinicians.
References
Bergh P, Gunterberg B, Meis-Kindblom JM, Kindblom LG. Prognostic factors and outcome of pelvic, sacral, and spinal chondrosarcomas: a center-based study of 69 cases. Cancer. 2001;91:1201–1212.
Bergh P, Lars-Gunnar K, Gunterberg B, Remotti F, Ryd W, Meis-Kindblom JM. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer. 2000;88:2122–2134.
Chen YL, Liebsch N, Kobayashi W, Goldberg S, Kirsch D, Calkins G, Childs S, Schwab J, Hornicek F, DeLaney T. Definitive high-dose photon/proton radiotherapy for unresected mobile spine and sacral chordomas. Spine (Phila Pa 1976). 2013;38:E930–936.
DeLaney TF, Liebsch NJ, Pedlow FX, Adams J, Dean S, Yeap BY, McManus P, Rosenberg AE, Nielsen GP, Harmon DC, Spiro IJ, Raskin KA, Suit HD, Yoon SS, Hornicek FJ. Phase II study of high-dose photon/proton radiotherapy in the management of spine sarcomas. Int J Radiat Oncol Biol Phys. 2009;74:732–739.
Delaney TF, Liebsch NJ, Pedlow FX, Adams J, Weyman EA, Yeap BY, Depauw N, Nielsen GP, Harmon DC, Yoon SS, Chen YL, Schwab JH, Hornicek FJ. Long-term results of Phase II study of high dose photon/proton radiotherapy in the management of spine chordomas, chondrosarcomas, and other sarcomas. J Surg Oncol. 2014;110:115–122.
Fuchs B, Dickey ID, Yaszemski MJ, Inwards CY, Sim FH. Operative management of sacral chordoma. J Bone Joint Surg Am. 2005;87:2211–2216.
Fujimura Y, Maruiwa H, Takahata T, Toyama Y. Neurological evaluation after radical resection of sacral neoplasms. Paraplegia. 1994;32:396–406.
Gunterberg B. Effects of major resection of the sacrum. Clinical studies on urogenital and anorectal function and a biomechanical study on pelvic strength. Acta Orthop Scand Suppl. 1976;162:1–38.
Gunterberg B, Kewenter J, Petersen I, Stener B. Anorectal function after major resections of the sacrum with bilateral or unilateral sacrifice of sacral nerves. Br J Surg. 1976;63:546–554.
Gunterberg B, Norlen L, Stener B, Sundin T. Neurourologic evaluation after resection of the sacrum. Invest Urol. 1975;13:183–188.
Gunterberg B, Petersen I. Sexual function after major resections of the sacrum with bilateral or unilateral sacrifice of sacral nerves. Fertil Steril. 1976;27:1146–1153.
Hsieh P C, Xu R, Sciubba D M,McGirt MJ, Nelson C, Witham TF, Wolinsky JP, Goskalan ZL. Long-term clinical outcomes following en bloc resections for sacral chordomas and chondrosarcomas: a series of twenty consecutive patients Spine (Phila Pa 1976). 2009;34:2233–2239.
Hugate RR, Dickey ID, Phimolsarnti R, Yaszemski MJ, Sim FJ. Mechanical effects of partial sacrectomy: when is reconstruction necessary? Clin Orthop Relat Res. 2006;450:82–88.
Hulen CA, Temple HT, Fox WP, Sama AA, Green BA, Eismont FJ. Oncologic and functional outcome following sacrectomy for sacral chordoma. J Bone Joint Surg Am. 2006;88:1532–1539.
Ikushima H, Osaki K, Furutani S, Yamashita K, Kishida Y, Kudoh T, Nishitani H. Pelvic bone complications following radiation therapy of gynecologic malignancies: clinical evaluation of radiation-induced pelvic insufficiency fractures. Gynecol Oncol. 2006;103:1100–1104.
Kim HJ, Boland PJ, Meredith DS, Lis E, Zhang Z, Shi W, Yamada YJ, Goodman KA. Fractures of the sacrum after chemoradiation for rectal carcinoma: incidence, risk factors, and radiographic evaluation. Int J Radiat Oncol Biol Phys. 2012;84:694–699.
Liu HH, Cella D, Gershon R, Shen J, Morales LS, Riley W, Hays RD. Representativeness of the PROMIS Internet panel. J Clin Epidemiol. 2010;63:1169–1178.
Moran D, Zadnik PL, Taylor T, Groves ML, Yurter A, Wolinsky J, Witham TF, Bydon A, Gokaslan ZL, Sciubba DM. Maintenance of bowel, bladder, and motor functions after sacrectomy. Spine J. 2015;15:222–229.
Nakai S, Yoshizawa H, Kobayashi S, Maeda K, Okumura Y. Anorectal and bladder function after sacrifice of the sacral nerves. Spine (Phila Pa 1976). 2000;25:2234–2239.
Ruggieri P, Angelini A, Ussia G, Montalti M, Mercuri M. Surgical margins and local control in resection of sacral chordomas. Clin Orthop Relat Res. 2010;468:2939–2947.
Schwab JH, Healey JH, Rose P, Casas-Ganem J, Boland PJ. The surgical management of sacral chordomas. Spine (Phila Pa 1976). 2009;34:2700–2704.
Wuisman P, Lieshout O, Sugihara S, Van Dijk M. Total sacrectomy and reconstruction: oncologic and functional outcome. Clin Orthop Relat Res. 2000;381:192–203.
Acknowledgments
We thank Al Ferreira RN, and Anne Fiore NP, for their assistance in working with patients during data collection for this project. We also thank the Harris Center for Chordoma Care at Massachusetts General Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (JS) has received consulting fees from Stryker Corp (Kalamazoo, MI, USA) and Biom’Up (Saint-Priest, France) outside the submitted work. One of the authors (JH) is Deputy Editor, Editorial Board, Clinical Orthopaedics and Related Research ®. One of the authors (TFD) received a grant from the National Cancer Institute (Principal Investigator, 5P01 CA21239-33, Optimizing Proton Radiation Therapy); receives royalties from UpToDate and Wolters Kluwer Health (Baltimore, MD, USA); and received payment for an audio lecture on proton radiation therapy from Oakstone Publishing (Birmingham, AL, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article

Cite this article
Phukan, R., Herzog, T., Boland, P.J. et al. How Does the Level of Sacral Resection for Primary Malignant Bone Tumors Affect Physical and Mental Health, Pain, Mobility, Incontinence, and Sexual Function?. Clin Orthop Relat Res 474, 687–696 (2016). https://doi.org/10.1007/s11999-015-4361-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4361-3