
Abstract
This classic article is a translation and reprint (Appendix 1. Supplemental material is available with the online version of CORR.) from the French of the original article by M. Robert, entitled La radiographie de l’articulation trapézo-métacarpienne. Les arthroses de cette jointure. The original article was published in Société de Radiologie Méd de France, Bulletins.1936;24:687-689. (Reproduced with kind permission of the SFR.)
Similar content being viewed by others


Avoid common mistakes on your manuscript.
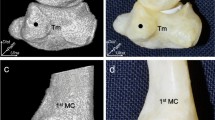
Lying flat on a horizontal surface, isolated from all its anatomic connections, the appearance of the trapeziometacarpal joint is as follows:
-
a)
On the side of the trapezium, there is a quadrilateral facet that is concave in the transverse plane, and convex in the anteroposterior direction.
-
b)
On the side of the first metacarpal, the facet is configured inversely to the facing side of the joint facet, meaning convex from side to side, and concave from front to back.
If one considers only the bony anatomy, the radiography of this joint in the horizontal plane would not be particularly difficult. But, obtaining good radiographic images in the living human hand is more complicated. For example, the palmar surface of the trapezium and of the first metacarpal are not exactly in the frontal plane. Rather, they are oblique relative to principal axis of the hand. Moreover, the trapezium is anterior to the other carpal bones, and represents the lateral border of the carpal row. The fact that the trapeziometacarpal joint is not perpendicular to the anteroposterior plane of the wrist explains why it is not well visualized on the typical AP views of the wrist taken in that plane.
For a radiograph to provide a good view of this joint, one needs to see the full length of the joint space. To get that view, the dorsal or palmar surface of first metacarpal and the trapezium must lie flat on the radiographic plate. However, because of the shape of the joint as described above, it is impossible to make the palmar side of the trapeziometacarpal joint lie flat on the radiographic plate. So necessarily, the radiograph of the joint needs to be done with the dorsal face on the plate. To achieve this position, one must either force the wrist into supination (Fig. 1) or pronation (Fig. 2).

Position of the hand and wrist in forced supination for radiography of the CMC joint

Position of the hand and wrist in forced pronation for radiography of the CMC joint
Forced supination has two drawbacks. The first drawback, which is the more serious of the two, is that in a position of forced supination, it is very difficult to get the trapezometacarpal joint into the same plane as the radiographic plate itself. The overhanging of the head of the first metacarpal partly prevents getting the wrist into this position. Also, maintaining this position is fatiguing and difficult for the patient, resulting in patient movement affecting the quality of the image.
By contrast, forced pronation is easier to achieve and more comfortable for the patient. Importantly, it also is more likely to position the joint exactly in the plane of the radiographic plate. For these reasons, forced pronation with the dorsal face of the joint on the plate is the approach of choice for trapeziometacarpal joint radiography. The beam should be centered on the joint, which can be identified by palpating and moving the first metarcarpal.
The trapeziometacarpal joint is a common site of degenerative changes. Most often, when a patient complains of vague, diffuse pain of the thumb, arthritis of the trapeziometacarpal joint is the cause. Disease progression in this location is similar to the evolution of degenerative arthrosis in other anatomic sites, beginning with narrowing of the joint space. Most often in this joint, the narrowing occurs asymmetrically, and is much more pronounced on the lateral side of the joint.
As the cartilage thins, the subchondral bone becomes more dense. Then, osteophytes appear on the trapezial side of the joint. Because this joint plays such a large functional role in thumb opposition, the arthritis progresses, and the base of the first metacarpal erodes the trapezium. That bone may become progressively more hollowed, and, in severe cases, it may take on a scaphoid shape.
Interestingly, although the trapeziometacarpal joint frequently shows degenerative changes, only uncommonly is it the cause of inflammatory arthritis. This joint is involved by the inflammatory disease in the late and subacute stage; this is in contrast to the smaller joints of the carpus, which are involved early in the disease.
From the practical point of view, radiologists typically will see only more advanced cases, since it would be unusual for a doctor to order a radiograph of the trapeziometacarpal joint early in the disease process. This is regrettable, because therapeutic interventions here—like in all arthritic joints—are more likely to succeed earlier in the natural history of the condition. By the time bony changes are visible, they will persist regardless of treatment, and the damaged articulation will cause mechanical symptoms, diminishing the likelihood of achieving a good functional result.
By contrast, early treatment arrests the progression of degenerative arthritis, and limits the damage.
In Aix-les-Bains, we get very good results with a combination of local heat treatments employing thermal baths using the Berthollet method, along with cautious radiotherapy of the joint.
Author information
Authors and Affiliations
Additional information
Editor’s Note: This translation was performed by Rémy S. Nizard MD and Seth S. Leopold MD. We took substantial license in condensing some of the sentence structure and using more contemporary terms and syntax. Some statements appeared ambiguous and we necessarily interpreted the meanings, hopefully capturing Dr. Robert’s intent.
Seth S. Leopold MD (✉) Clinical Orthopaedics and Related Research, 1600 Spruce Street, Philadelphia, PA 19103, USA e-mail: sleopold@clinorthop.org
Seth S. Leopold MD (✉) Clinical Orthopaedics and Related Research, 1600 Spruce Street, Philadelphia, PA 19103, USA e-mail: sleopold@clinorthop.org
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article
Cite this article
Robert, M. The Classic: Radiography of the Trapeziometacarpal Joint. Degenerative Changes of This Joint. Clin Orthop Relat Res 472, 1095–1096 (2014). https://doi.org/10.1007/s11999-013-2930-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-2930-x