
Abstract
Background
The postoperative analgesic potential of periarticular anesthetic infiltration (PAI) after TKA is unclear as are the complications of continuous femoral nerve block on quadriceps function.
Questions/purposes
We asked (1) whether PAI provides equal or improved postoperative pain control in comparison to a femoral nerve block in patients who have undergone TKA; and (2) if so, whether PAI improves early postoperative quadriceps control and facilitates rehabilitation.
Methods
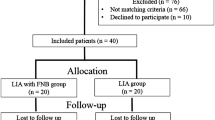
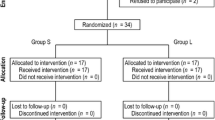
We randomized 60 patients to receive either PAI or femoral nerve block. During the first 5 days after TKA, we compared narcotic consumption, pain control, quadriceps function, walking distance, knee ROM, capacity to perform a straight leg raise, and active knee extension. Medication-related side effects, complications, operating room time, and hospitalization duration were compared.
Results
Opioid consumption was lower in the PAI group during the first 8 postoperative hours (12.5 mg versus 18.7 mg morphine), as was reported pain at rest (1.7 versus 3.5 on a 10-point VAS). Thereafter, narcotic consumption and reported pain were similar up to 120 hours. More subjects in the femoral nerve block group experienced quadriceps motor block (37% versus 0% in the PAI group). On Days 1 to 3, subjects in the PAI group experienced better capacity to perform the straight leg raise, active knee extension, and had longer walking distances.
Conclusions
PAI provided pain control equivalent to that of a femoral nerve block while avoiding a motor block and its negative functional impacts. The data suggest it should be considered an alternative to a femoral nerve block.
Level of Evidence
Level I, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.





Similar content being viewed by others

References
Albert TJ, Cohn JC, Rothman JS, Springstead J, Rothman RH, Booth RE Jr. Patient-controlled analgesia in a postoperative total joint arthroplasty population. J Arthroplasty. 1991;6(suppl):S23–S28.
Allen HW, Liu SS, Ware PD, Nairn CS, Owens BD. Peripheral nerve blocks improve analgesia after total knee replacement surgery. Anesth Analg. 1998;87:93–97.
Badner NH, Bourne RB, Rorabeck CH, MacDonald SJ, Doyle JA. Intra-articular injection of bupivacaine in knee-replacement operations: results of use for analgesia and for preemptive blockade. J Bone Joint Surg Am. 1996;78:734–738.
Ben-David B, Schmalenberger K, Chelly JE. Analgesia after total knee arthroplasty: is continuous sciatic blockade needed in addition to continuous femoral blockade? Anesth Analg. 2004;98:747–749.
Browne C, Copp S, Reden L, Pulido P, Colwell C Jr. Bupivacaine bolus injection versus placebo for pain management following total knee arthroplasty. J Arthroplasty. 2004;19:377–380.
Busch CA, Shore BJ, Bhandari R, Ganapathy S, MacDonald SJ, Bourne RB, Rorabeck CH, McCalden RW. Efficacy of periarticular multimodal drug injection in total knee arthroplasty: a randomized trial. J Bone Joint Surg Am. 2006;88:959–963.
Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. 1999;91:8–15.
Carli F, Clemente A, Asenjo JF, Kim DJ, Mistraletti G, Gomarasca M, Morabito A, Tanzer M. Analgesia and functional outcome after total knee arthroplasty: periarticular infiltration vs continuous FB. Br J Anaesth. 2010;105:185–195.
Chelly JE, Greger J, Gebhard R, Coupe K, Clyburn TA, Buckle R, Criswell A. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty. 2001;16:436–445.
Cuvillon P, Ripart J, Lalourcey L, Veyrat E, L’Hermite J, Boisson C, Thouabtia E, Eledjam JJ. The continuous FB catheter for postoperative analgesia: bacterial colonization, infectious rate and adverse effects. Anesth Analg. 2001;93:1045–1049.
DeWeese FT, Akbari Z, Carline E. Pain control after knee arthroplasty: intraarticular versus epidural anesthesia. Clin Orthop Relat Res. 2001;392:226–231.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213.
Forst J, Wolff S, Thamm P, Forst R. Pain therapy following joint replacement: a randomized study of patient-controlled analgesia versus conventional pain therapy. Arch Orthop Trauma Surg. 1999;119:267–270.
Horlocker TT, Cabanela ME, Wedel DJ. Does postoperative epidural analgesia increase the risk of peroneal nerve palsy after total knee arthroplasty? Anesth Analg. 1994;79:495–500.
Horlocker TT, Hebl JR, Kinney MA, Cabanela ME. Opioid-free analgesia following total knee arthroplasty: a multimodal approach using continuous lumbar plexus (psoas compartment) block, acetaminophen, and ketorolac. Reg Anesth Pain Med. 2002;27:105–108.
Klasen JA, Opitz SA, Melzer C, Thiel A, Hempelmann G. Intraarticular, epidural, and intravenous analgesia after total knee arthroplasty. Acta Anaesthesiol Scand. 1999;43:1021–1026.
Lombardi AV Jr, Berend KR, Mallory TH, Dodds KL, Adams JB. Soft tissue and intra-articular injection of bupivacaine, epinephrine, and morphine has a beneficial effect after total knee arthroplasty. Clin Orthop Relat Res. 2004;428:125–130.
Luber MJ, Greengrass R, Vail TP. Patient satisfaction and effectiveness of lumbar plexus and sciatic nerve block for total knee arthroplasty. J Arthroplasty. 2001;16:17–21.
Mauerhan DR, Campbell M, Miller JS, Mokris JG, Gregory A, Kiebzak GM. Intra-articular morphine and/or bupivacaine in the management of pain after total knee arthroplasty. J Arthroplasty. 1997;12:546–552.
McNamee DA, Parks L, Milligan KR. Post-operative analgesia following total knee replacement: an evaluation of the addition of an obturator nerve block to combined femoral and sciatic nerve block. Acta Anaesthesiol Scand. 2002;46:95–99.
Mullaji A, Kanna R, Shetty GM, Chavda V, Singh DP. Efficacy of periarticular injection of bupivacaine, fentanyl, and methylprednisolone in total knee arthroplasty: a prospective, randomized trial. J Arthroplasty. 2010;25:851–857.
Ritter MA, Koehler M, Keating EM, Faris PM, Meding JB. Intra-articular morphine and/or bupivacaine after total knee replacement. J Bone Joint Surg Br. 1999;81:301–303.
Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. 1998;87:88–92.
Singelyn FJ, Gouverneur JM. Postoperative analgesia after total hip arthroplasty: i.v. PCA with morphine, patient-controlled epidural analgesia, or continuous “3-in-1” block? A prospective evaluation by our acute pain service in more than 1,300 patients. J Clin Anesth. 1999;11:550–554.
Strassels SA, Chen C, Carr DB. Postoperative analgesia: economics, resource use, and patient satisfaction in an urban teaching hospital. Anesth Analg. 2002;94:130–137.
Toftdahl K, Nikolajsen L, Haraldsted V, Madsen F, Tonnesen EK, Soballe K. Comparison of peri- and intraarticular analgesia with FB after total knee arthroplasty: a randomized clinical trial. Acta Orthop. 2007;78:172–179.
Vendittoli PA, Makinen P, Drolet P, Lavigne M, Fallaha M, Guertin MC, Varin F. A multimodal analgesia protocol for total knee arthroplasty: a randomized, controlled study. J Bone Joint Surg Am. 2006;88:282–289.
Wang H, Boctor B, Verner J. The effect of single-injection FB on rehabilitation and length of hospital stay after total knee replacement. Reg Anesth Pain Med. 2002;27:139–144.
Acknowledgments
We thank Marie-Êve Lacasse and Charles Rivière, both research students; Lucie Grondin, physiotherapist, who helped gather the data; and Michel Fallaha, MD, FRCS (C) and Alain Roy, MD, FRCS (C) who performed some of the TKAs.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (ML) has received payments or benefits not related to this work, during the study period, an amount of USD 10,000–USD 100,000 from Wright Medical Technology (Memphis, TN, USA) and Zimmer (Warsaw, IN, USA). One of the authors (P-AV) has received payments or benefits not related to this work, during the study period, an amount of USD 10,000–USD 100,000 from Wright Medical, Biomet (Warsaw, IN, USA), and Stryker Orthopaedics (Mahwah, NJ, USA). The institution of one or more of the authors (PAV, ML, DA, PD) has received, during the study period, unrestricted research funding not related to this work from Biomet, Zimmer, Stryker, Smith and Nephew (Memphis, TN, USA), and DePuy Orthopaedics (Warsaw, IN, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Randomization, surgical procedures, and followup of the subjects were performed at Maisonneuve-Rosemont Hospital, Montreal, Quebec, Canada.
About this article
Cite this article
Chaumeron, A., Audy, D., Drolet, P. et al. Periarticular Injection in Knee Arthroplasty Improves Quadriceps Function. Clin Orthop Relat Res 471, 2284–2295 (2013). https://doi.org/10.1007/s11999-013-2928-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-2928-4