
Abstract
Background
The crossover sign is a radiographic finding associated with cranial acetabular retroversion and has been associated with pincer-type femoroacetabular impingement (FAI) in patients with hip pain. Variable morphology, location, and size of the anterior inferior iliac spine (AIIS) may contribute to the crossover sign even in the absence of retroversion. Thus, the sign may overestimate the incidence of acetabular retroversion.
Questions/purposes
We asked: Can the crossover sign appear on standardized, well-positioned AP pelvis radiographs despite the absence of acetabular retroversion? And what is the contribution of variable size and morphology of the AIIS to a crossover sign?
Methods
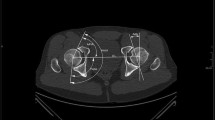
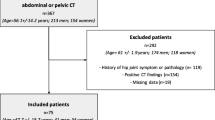
We evaluated radiographs of 53 patients with symptomatic FAI in the absence of substantial chondral degenerative changes (< Tönnis Grade 2). Forty-one radiographs met the appropriate criteria of neutral tilt and obliquity. Three independent reviewers determined presence and location of the crossover sign. Acetabular version was defined using high-resolution three-dimensional CT. CT reconstructions were used to define three AIIS types addressing AIIS morphology.
Results
Nineteen of 38 radiographs with a crossover sign on AP radiographs had focal or global acetabular retroversion on three-dimensional CT (positive and negative predictive values = 50%). In contrast, the AIIS extended to or below the level of the anterior superior acetabular rim and was partially or completely responsible for the appearance of a radiographic crossover sign in all 19 hips with an anteverted acetabulum. High interobserver reliability (kappa > 0.8) was found for AIIS types.
Conclusions
A crossover sign is frequently present on well-positioned AP pelvis radiographs in the absence of acetabular retroversion. Variable AIIS morphology may explain the appearance of this sign in the presence or absence of acetabular retroversion.
Level of Evidence
Level III, diagnostic study. See Instructions for Authors for a complete description of levels of evidence.






Similar content being viewed by others

References
Beaule PE, Allen DJ, Clohisy JC, Schoenecker PL, Leunig M. The young adult with hip impingement: deciding on the optimal intervention. Instr Course Lect. 2009;58:213–222.
Dandachli W, Islam SU, Liu M, Richards R, Hall-Craggs M, Witt J. Three-dimensional CT analysis to determine acetabular retroversion and the implications for the management of femoro-acetabular impingement. J Bone Joint Surg Br. 2009;91:1031–1036.
Dandachli W, Ul Islam S, Tippett R, Hall-Craggs MA, Witt JD. Analysis of acetabular version in the native hip: comparison between 2D axial CT and 3D CT measurements. Skeletal Radiol. 2011;40:877–883.
Dora C, Leunig M, Beck M, Simovitch R, Ganz R. Acetabular dome retroversion: radiological appearance, incidence and relevance. Hip Int. 2006;16:215–222.
Eckman K, Hafez MA, Ed F, Jaramaz B, Levison TJ, Digioia AM 3rd. Accuracy of pelvic flexion measurements from lateral radiographs. Clin Orthop Relat Res. 2006;451:154–160.
Ferguson SJ, Bryant JT, Ganz R, Ito K. An in vitro investigation of the acetabular labral seal in hip joint mechanics. J Biomech. 2003;36:171–178.
Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120.
Jamali AA, Mladenov K, Meyer DC, Martinez A, Beck M, Ganz R, Leunig M. Anteroposterior pelvic radiographs to assess acetabular retroversion: high validity of the “cross-over-sign.” J Orthop Res. 2007;25:758–765.
Kakaty DK, Fischer AF, Hosalkar HS, Siebenrock KA, Tannast M. The ischial spine sign: does pelvic tilt and rotation matter? Clin Orthop Relat Res. 2010;468:769–774.
Kalberer F, Sierra RJ, Madan SS, Ganz R, Leunig M. Ischial spine projection into the pelvis: a new sign for acetabular retroversion. Clin Orthop Relat Res. 2008;466:677–683.
Larson CM, Kelly BT, Stone RM. Making a case for anterior inferior iliac spine/subspine hip impingement: three representative case reports and proposed concept. Arthroscopy. 2011;27:1732–1737.
Pan HL, Kawanabe K, Akiyama H, Goto K, Onishi E, Nakamura T. Operative treatment of hip impingement caused by hypertrophy of the anterior inferior iliac spine. J Bone Joint Surg Br. 2008;90:677–679.
Siebenrock KA, Kalbermatten DF, Ganz R. Effect of pelvic tilt on acetabular retroversion: a study of pelves from cadavers. Clin Orthop Relat Res. 2003;407:241–248.
Tannast M, Kubiak-Langer M, Langlotz F, Puls M, Murphy SB, Siebenrock KA. Noninvasive three-dimensional assessment of femoroacetabular impingement. J Orthop Res. 2007;25:122–131.
Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis—what the radiologist should know. AJR Am J Roentgenol. 2007;188:1540–1552.
Tönnis D. [Letter: Congenital hip dysplasia: clinical and radiological diagnosis (author’s transl)] [in German]. Z Orthop Ihre Grenzgeb. 1976;114:98–99.
Acknowledgments
The authors thank Gavin Duke, MD, musculoskeletal radiologist, East River Medical Imaging, New York, NY, USA, for his help in performing the agreement study to validate AIIS type classification.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at the Hospital for Special Surgery, New York, NY, USA.
About this article
Cite this article
Zaltz, I., Kelly, B.T., Hetsroni, I. et al. The Crossover Sign Overestimates Acetabular Retroversion. Clin Orthop Relat Res 471, 2463–2470 (2013). https://doi.org/10.1007/s11999-012-2689-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2689-5