
Abstract
Purpose of review
Gastric outlet obstruction is a syndrome that is caused by several benign and malignant diseases. Endoscopic ultrasonography-guided gastroenterostomy (EUS-GE) is a novel treatment that seems to combine the advantages of the two traditional treatments: enteral stent placement (ES) and surgical gastrojejunostomy (SGJ). This review aims to determine the current position of EUS-GE amidst the two traditional treatment options.
Recent findings
Different approaches can be adopted to facilitate EUS-GE. Direct gastroenterostomy seems to have the shortest procedure time. All methods possess high technical success rates. Several retrospective analyses have compared EUS-GE to ES and SGJ. EUS-GE seems to have better stent patency compared to ES and a lower adverse event rate compared to SGJ. Recently, randomized trials have been initiated which compare EUS-GE with ES or SGJ.
Summary
Although the currently published literature unequivocally shows the great promises of EUS-GE, properly powered and controlled studies are warranted to ascertain the definitive position of EUS-GE within the treatment repertoire of GOO. Until reliable data has been collected, EUS-GE can be considered a safe and effective alternative to ES and SGJ.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric outlet obstruction (GOO) is a phenomenon that is characterized by mechanical obstruction of the distal stomach, pylorus, or duodenum [1]. The condition is caused by several benign and malignant diseases. Peptic ulcer disease due to nonsteroidal anti-inflammatory drugs (NSAIDs) or Helicobacter pylori infection is the most frequent cause of benign GOO [2•]. Other etiologies include anastomotic strictures and (complications of) acute and chronic pancreatitis [3]. Common diseases that may result in malignant GOO are gastric, pancreatic, or duodenal carcinomas [4]. An estimated 10 to 25% of patients with pancreatic or biliary cancer will develop GOO at a certain point during the disease course [5]. Extraluminal compression of the gastric outlet by metastatic disease or lymphoma may also result in obstruction [2•].
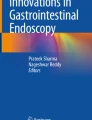
Symptoms of GOO typically encompass nausea, vomiting, inability to tolerate oral intake, and abdominal pain [6]. Owing to metastatic or irresectable disease, patients with malignant GOO generally have a poor prognosis with a median survival of 2 to 3 months [7, 8]. These symptoms may have a considerable impact on quality of life [9]. Therefore, treatment of malignant causes of GOO is often directed at palliation of obstructive symptoms and resumption of oral intake [10, 11]. Classically, malignant GOO is treated by means of two interventions: surgical gastrojejunostomy (SGJ) or placement of an enteral stent (ES) (Fig. 1).

Treatment options for gastric outlet obstruction. A Enteral stent placement. B Surgical gastrojejunostomy. C Endoscopic ultrasonography-guided gastroenterostomy.
SGJ can be performed through an open or laparoscopic procedure [12]. Technical success rates of SGJ are very high, ranging from 95 to 100% [9]. Nevertheless, postoperative course is often characterized by a high morbidity rate of up to 24% [13]. In addition to delayed gastric emptying, common complications after SGJ are anastomotic leakage, ileus, and bleeding [14, 15]. These disadvantages notwithstanding, a surgically created gastrointestinal anastomosis is known to be durable in terms of patency, resulting in low reintervention rates [13].
Comparable to SGJ, ES is distinguished by a high technical success rate [16]. Moreover, postprocedural initiation of oral intake is fast, especially compared to SGJ [17]. However, ES is at risk of migration and dysfunction, due to tissue ingrowth or food impaction. Hence, reintervention because of recurrent obstructive symptoms is required in approximately 25% of patients [18].
Based on the characteristics of both treatments, ES is mainly recommended in patients with a short life-expectancy of less than 6 months, whereas SGJ is advised in patients with an expected survival of longer than six months [2•].
Owing to the limitations of the above-mentioned treatments, endoscopic ultrasonography-guided gastroenterostomy (EUS-GE) has emerged as a potentially valuable alternative (Fig. 1) [19]. EUS-GE is characterized by placing a lumen-apposing metal stent (LAMS) between the stomach and jejunal loop distal to the obstruction, thereby creating an alternative route for food passage [20]. This minimally invasive treatment has the capacity to combine the benefits of ES and SGJ while avoiding the risks involved in both treatments [21].
This review aims to identify the current position of EUS-GE amidst SGJ and ES for the treatment of malignant GOO. Furthermore, objectives for future research will be identified. The discussion of these issues attempts to provide an answer to the question whether EUS-GE is ready for prime time.
Treatment
Interventional Procedures
EUS-Guided Gastroenterostomy (EUS-GE)
Due to the frequently occurring negative effects of both SGJ and ES, alternative treatment options for GOO were examined in the past two decades. The first experiences with the endoscopic ultrasonography-guided creation of a gastrointestinal anastomosis by means of a specially designed suturing device were already described in 2002 [22, 23]. Nevertheless, it took about a decade for the first dedicated LAMS to be introduced [24]. The aim of LAMS placement was to create an anastomosis between two gastrointestinal lumina [25]. Initial reports focused on the creation of a cholecystogastrostomy with a biflanged stent [24]. The LAMS was loaded in a delivery system which could be connected to an echoendoscope. Originally, a guidewire was used to facilitate tract dilation and advance the LAMS into the target lumen after which the two structures could be anastomosed [24]. Updated versions of the delivery system, however, contain a wired nose cone tip that enables electrocautery. This feature promotes advancement of the catheter — in which the LAMS is folded — into the structure of interest, rendering prior tract dilation redundant [26]. Currently, LAMS placement in the gastrointestinal tract is approved for drainage of pancreatic fluid collections, the gallbladder, and biliary tract [27]. Yet, in 2012, a porcine model showed its effectiveness for the creation of a gastroenterostomy using an anchor wire, access device, and LAMS [19]. Consequently, since the first studies on EUS-GE in humans were published, this off-label indication for LAMS use gained momentum [28, 29].
Currently, two electrocautery-enhanced delivery systems are available: the Hot AXIOS™ stent (Boston Scientific Corporation, Marlborough, MA, USA) and the Niti-S™ Hot SPAXUS™ stent (Taewoong Medical Co., Gyeonggi-do, South Korea) [27].
Standard Procedure
Several methods have been described to perform EUS-GE with a LAMS, such as EUS-guided balloon-occluded gastroenterostomy bypass (EPASS), balloon-assisted gastroenterostomy, and direct gastroenterostomy (synonyms: freehand technique or wireless EUS-guided gastroenterostomy simplified technique (WEST)) [30]. The balloon-assisted approach is characterized by the transgastric puncture of an inflated balloon that is positioned in the distal duodenum or proximal jejunum. Bursting of the balloon confirms that the correct target loop is punctured, after which a LAMS can be placed between the stomach and duodenum or jejunum [29]. During EPASS, a dedicated double balloon enteric tube is positioned in the distal duodenum or proximal jejunum. The balloons are inflated, and subsequently, the space between the balloons is distended by instillation of saline. Finally, this section is punctured transgastrically after which the LAMS is deployed [31, 32]. The direct gastroenterostomy approach is distinguished by directly infusing saline distal to the obstruction, without using a balloon catheter or guidewire [20]. Since our institute exclusively uses this technique, we will explain the different steps involved in performing a direct gastroenterostomy in more detail (Figs. 2 and 3).

EUS-GE procedural steps. A Fluid instillation of indigo-colored saline. B Transluminal puncture with electrocautery-enhanced delivery system. C Deployment of distal flange. D Deployment of proximal flange.

Ultrasonographic and endoscopic images of EUS-GE. A Bowel distension after instillation of saline. B Deployment of distal flange in duodenum/jejunum. C Backflow of indigo-colored saline in stomach after deployment of proximal flange. D Visibility of intestinal mucosa through the LAMS.
To perform EUS-GE as safe as possible, the stomach should be relieved of contents. Therefore, patients should fast for a minimum of 6 h prior to the procedure, also depending on the severity of obstruction. Preferably, a nasogastric tube is placed to minimize the risk of aspiration. Just before or after EUS-GE, prophylactic antibiotics are administered intravenously to mitigate the risk of intra-abdominal infections.
The direct gastroenterostomy is performed under deep conscious sedation or — if adequate airway management is warranted — under general anesthesia.
The first step of this approach consists in inserting a gastroscope to remove residual gastric contents. If not already in place, a jejunal feeding tube or nasobiliary drain is placed distal to the obstruction deep in the jejunum. Saline, colored with a small amount of dye (e.g., indigo carmine), is infused via the feeding tube or nasobiliary drain into the small bowel distal to the obstruction. The device we use to facilitate saline infusion is the Rapid Refill™ Continuous Injection System (Boston Scientific Corporation, Marlborough, MA, USA). At the same time as fluid is instilled, the endoscope is replaced by a therapeutic linear echoendoscope. We advise to position the echoendoscope in the gastric antrum and rotate the scope clockwise to identify a distended intestinal loop. In case of excessive intestinal motility, scopolamine butylbromide or glucagon can be used to inhibit peristalsis. Based on several endosonographic characteristics, the endoscopist is able to identify a target loop. A key feature of a saline-infused jejunal loop is what we call “the swirl sign.” This entails the rapid flow of air mixed with saline close to the distal end of the jejunal feeding tube or nasobiliary drain. Another characteristic that is used is the identification of circular folds (valves of Kerckring) in the small bowel.
A target loop is sufficiently dilated when the segment is distended to at least –4 cm. This prevents that the punctured intestinal loop is pushed away from the stomach wall during LAMS deployment. Ideally, the target loop runs axially from the position of the transducer, allowing enough space to insert and deploy the LAMS. When a sufficiently distended segment of the jejunum is found, the electrocautery-enhanced delivery system can be connected to the echoendoscope. If the endoscopist is unsure whether the target loop is in fact jejunum, it is recommended to puncture the lumen with a fine needle aspiration (FNA) needle and verify that the punctate is indeed blue dyed saline. This confirms that a correct loop is visualized.
After verification of the correct target lumen, the stomach wall and intestinal wall are punctured consecutively with the electrocautery-enhanced catheter. Preferentially, the stomach is punctured as distal as possible. The distal flange of the 20-mm LAMS is deployed in the jejunum followed by traction of the flange against the bowel wall. Subsequently, the proximal part of the stent is deployed in the stomach and pushed out the working channel during gentle retraction of the echoendoscope. Position and passage of the stent are confirmed by backflow of the indigo-colored saline from the jejunum back into the stomach. The saline will be suctioned to prevent aspiration pneumonia. We generally do not dilate the LAMS; instead, it will be left to expand naturally. In case EUS-GE is used to palliate symptoms of malignant GOO, the LAMS will not be removed. Directly after a technically successful procedure, all tubes will be removed.
Patients are allowed a clear liquid diet the same day as the procedure took place. The next morning, this can be expanded to an easily digestible diet if there are no signs of complications. When the patient tolerates this without vomiting, oral intake can be resumed without any restrictions. Generally, patients are discharged the day after the procedure, although limited data suggests that same-day discharge may be safe as well.
No prospective comparisons of the different EUS-GE techniques have been conducted. Chen et al. retrospectively compared the direct and balloon-assisted techniques. They concluded that the direct method could be performed in less time than the balloon-assisted approach. However, no differences in technical success, clinical success, and adverse events (AEs) were found [33]. A recently published meta-analysis, on the other hand, did find a lower AE rate in the direct EUS-GE group as compared to balloon-assisted techniques. The same applies to the length of hospital stay [30].
Primarily based on the suggestion that the direct approach consumes less time, many endoscopists prefer this method [20].
General Outcomes of EUS-GE
To date, more than 20 single-arm studies have been published that specifically focused on EUS-GE performance and outcomes in malignant GOO. Most have a sample size between 10 and approximately 50 patients, with few exceeding 100 patients. Based on these studies, technical and clinical success ranges between 80–100% and 73–95%, respectively [21, 34, 35, 36•].
A meta-analysis from Iqbal et al. reported an AE rate of 12% after EUS-GE [37]. Serious AEs occur in approximately 3–6% of EUS-GE procedures, consisting of peritonitis, perforation, hemorrhage, and abdominal pain [38, 39]. A notorious periprocedural complication of EUS-GE is LAMS misdeployment. This occurs when the distal or proximal flange of the LAMS is deployed outside of the gastrointestinal tract. When the target lumen is already punctured, this might have serious consequences, such as peritonitis, surgical intervention, or death [40•]. Although misdeployment is not uncommon — occurring in up to 10% of LAMS placements — most of these complications can be managed endoscopically and have only mild consequences [40•]. The rate of LAMS misdeployments might be related to the technical complexity of EUS-GE and the learning curve associated with the procedure [40•, 41•, 42•]. It is estimated that proficiency is achieved after 7 to 25 procedures. Notably, the studies that have assessed learning curve of EUS-GE included endoscopists experienced in therapeutic EUS, emphasizing the complexities associated with the procedure [41•, 42•].
Currently, LAMSs are registered for implantation up to a maximum of 60 days in case of drainage of pancreatic fluid collections [43]. However, in case of palliative treatment of GOO, the LAMS generally remains in situ until death or until removal is warranted for medical reasons. A long-term evaluation of patients who underwent EUS-GE observed LAMS dysfunction in 2 of 53 patients (3.7%) because of stent occlusion. The other patients experienced no LAMS-related problems, after a median follow-up of 196 days in malignant GOO and 319.5 days in benign GOO [44]. These results are corroborated by Kastelijn et al., who observed a LAMS dysfunction rate of 6.1% [21].
In addition to LAMS dysfunction as a long-term complication of EUS-GE, some case reports have described jejunal ulceration at the site opposite to the distal flange, even resulting in perforation and consequent peritonitis. Yet, this complication is perhaps more common in benign GOO, since indwelling time tends to be longer compared to malignant causes of GOO [45].
Comparison with ES
With regard to the effectiveness of EUS-GE, several retrospective cohort studies have compared LAMS placement with ES (Tables 1 and 3) [46••, 47••, 48••, 49••, 50••, 51••]. None of these studies observed any differences in technical success. However, three studies concluded that EUS-GE resulted in higher clinical success rates compared to ES. These studies observed clinical success in more than 90% of EUS-GE patients, whereas ES was clinically successful in approximately 75% of patients [46••, 48••, 51••].
Only the study of Jaruvongvanich et al. reported statistically significant differences in the occurrence of AEs, in favor of EUS-GE (8.6% vs. 38.9%) [51••]. With regard to the patency of both treatments, four studies observed a significantly lower reintervention rate for recurrent obstructive symptoms in patients who underwent EUS-GE [46••, 47••, 48••, 51••]. This discrepancy is primarily explained by the high rate of stent dysfunction due to tumor in- or overgrowth, food impaction, or migration after ES. Moreover, time to stent failure also seems to be shorter after ES, compared to EUS-GE [48••, 49••, 51••]. With regard to EUS-GE, the pooled rate of LAMS misdeployment of these cohorts combined was 3.3%. Partly based on these comparative studies, the Endoscopic Society of Gastrointestinal Endoscopy (ESGE) currently perceives the use of EUS-GE in an expert setting as a valid alternative to ES [52•]. Nevertheless, the results of these retrospective studies should be interpreted cautiously since they might be affected by selection bias.
Comparison with SGJ
EUS-GE has been compared to SGJ in seven retrospective studies (Tables 2 and 3) [50••, 51••, 53••, 54••, 55••, 56••, 57••]. In all studies, technical success of SGJ was 100%. Most studies did not find differences in technical success between the two approaches. However, Khashab et al. observed a higher technical success rate when SGJ was performed (100% vs. 87%), although this did not translate into a higher proportion of clinical success [57••]. This is comparable to most other studies [50••, 53••, 54••, 55••, 56••, 57••]. The largest study of Jaruvongvanich et al. did find differences in clinical success — defined as tolerance of at least a liquid diet within 2 weeks — favoring EUS-GE (98.3% vs. 91.6%). Moreover, this study found a significantly lower reintervention rate in the EUS-GE group (0.9% vs. 13.7%) [51••].
Four studies noted a lower AE rate after EUS-GE, compared to SGJ. AEs in patients who underwent SGJ mainly consisted of postoperative delayed gastric emptying or ileus, anastomotic leakage, bleeding, or infection [51••, 53••, 54••, 56••]. Remarkably, Abbas et al. observed a lower AE rate after EUS-GE compared to SGJ in patients with peritoneal carcinomatosis, even though the former group was in a clinically worse condition than patients who underwent SGJ [56••].
What should be noted is that some studies compared EUS-GE with an open surgical approach, in contrast to a laparoscopic approach, which could have influenced the results [55••, 56••, 57••]. A laparoscopic gastrojejunostomy is considered to be the better option, since it results in a lower rate of postoperative gastroparesis, faster clinical success, and shorter length of hospital stay [58].
Bronswijk et al. and Kouanda et al. observed a shorter time to oral intake after EUS-GE (median 1 vs. 3 days and mean 1.3 vs. 4.7 days, respectively) [54••, 55••]. Moreover, time to initiation or resumption of chemotherapy tends to be shorter after EUS-GE compared to SGJ [55••, 56••].
Largely based on the above-mentioned publications, the ESGE concludes that EUS-GE is a valid alternative to SGJ within an expert setting [52•]. However, similarly to the comparison of EUS-GE with ES, the results of these studies might be affected by selection bias.
Practical Considerations
Based on our personal experience with EUS-GE and supported by evidence from the literature, we have formulated the following practical considerations which can be taken into account when considering EUS-GE:
We recommend the use of a LAMS with the largest luminal diameter, as to ensure an as wide as possible gastrointestinal anastomosis. Currently, the AXIOS™ stent has a maximum available diameter of 20 mm, whereas the SPAXUS™ stent has a largest available diameter of 16 mm [59, 60]. A recently published retrospective analysis compared the use of the 15 mm AXIOS™ stent with the 20 mm stent. Although the authors did not observe differences in clinical success and the rate of AEs, significantly more patients with a 20-mm LAMS tolerated a soft solid or complete diet at the end of study follow-up [36•]. These results suggest that a LAMS with the largest diameter is preferred.
The current literature did not specifically focus on the relation between etiology of the obstruction and technical and clinical success. Based on experience in our institute, we speculate that gastric cancer as cause of GOO might negatively influence EUS-GE performance and efficacy. The presence of a malignancy at the region of the antrum or pylorus could result in an increased distance between the gastric wall and the jejunal target loop, thereby creating difficulties for safe puncture and deployment of the LAMS. Moreover, malignancies located in the distal stomach might decrease gastric motility, which could lead to disappointing clinical effectiveness of EUS-GE. Currently, our research group is assessing the influence of etiology on EUS-GE outcomes. Hence, a more definitive conclusion is expected in time.
Malignant GOO may occur in conjunction with biliary obstruction [61]. Limited evidence is available with regard to the preferred treatment options in these specific situations. The CABRIOLET-study evaluated the relationship between various treatment combinations (EUS-guided interventions, transpapillary and/or duodenal SEMS placement) and dysfunction rates [62•]. Although highly underpowered, the results suggest a preference of EUS-GE with EUS-guided hepaticogastrostomy over other combinations, such as EUS-GE with transpapillary stent placement, EUS-guided cholecystoduodenostomy (EUS-CDS), or ES combined with either one of the above-mentioned procedures. The former treatment combination may lead to the lowest recurrence rate. The use of EUS-CDS, on the other hand, seems to be related to worse outcomes since it may be prone to food impaction due to a “sump” that is created when the obstructed duodenal bulb becomes clogged with food remains [62•]. Despite the drawbacks of this retrospective analysis, these outcomes suggest that certain treatment combinations might be better suited for concomitant biliary and gastric outlet obstruction than others.
Peritoneal involvement is predictive of morbidity and mortality in patients undergoing SGJ for malignant GOO [63•]. One retrospective study assessed whether this was also the case for EUS-GE compared to SGJ [56••]. Albeit EUS-GE patients were older and had more advanced disease, there was no difference in technical success. Furthermore, EUS-GE was associated with a lower AE rate. What should be noted is that patients in the SGJ group underwent an open procedure, what may have influenced the results. Nevertheless, in our experience, EUS-GE in patients with peritoneal carcinomatosis is generally safe and effective. However, it is advisable to confirm adequate intestinal passage by placing a nasojejunal feeding tube in order to exclude distal obstruction and paralytic ileus. Moreover, if abdominal radiology shows diffuse dilation of the small bowel with air-fluid levels, we do not recommend EUS-GE since risk of clinical failure tends to be high.
The presence of ascites is considered a contraindication for save execution of EUS-GE [52•]. This has various reasons. First, diagnosing ascites often implies the presence of peritoneal metastases and hence an advanced disease stage, rendering the clinical benefit of EUS-GE less likely [52•, 64•]. Second, ascites might suggest the existence of distal obstruction sites due to peritoneal metastases [52•]. Third, ascites might pose technical challenges during LAMS placement since it could push the target loop away from the gastric wall [64•]. Lastly, the electrocautery-enhanced tip of the delivery system may function less optimally. Based on these potential problems, we advise prudence when patients with GOO and ascites are considered for EUS-GE. Nevertheless, a retrospective analysis from Basha et al. compared patients with and without ascites that underwent EUS-GE, and they did not find differences in technical and clinical success or in the rate of adverse events [64•]. Hence, if the space between the gastric wall and the target loop is not increased by the presence of ascites, we argue that one can proceed with EUS-GE.
Despite LAMS misdeployment being a relatively uncommon complication of EUS-GE, consequences might be dreadful [40•]. In many cases, however, serious consequences can be prevented by merely placing through-the-scope or over-the-scope clips or perform endoscopic suturing [40•]. Nevertheless, a systematic review identified several methods to endoscopically salvage a misdeployed LAMS, such as bridging the initially placed LAMS with a second LAMS or SEMS [65]. An alternative approach is natural orifice transluminal endoscopic surgery (NOTES), in which the peritoneal cavity is traversed through the original gastric puncture site, a jejunal loop is grasped and penetrated with a needle-knife, allowing a second stent to be placed in the target jejunal lumen [66]. The above-mentioned salvage methods require considerable endoscopic expertise. Therefore, it might be desirable to be in close contact with the surgeon on call when performing EUS-GE, facilitating rapid discussion regarding the preferred way to treat the complication.
Accidental creation of a gastrocolic anastomosis is rare, occurring in less than 5% of EUS-GE misdeployments [40•]. In our institute, we have experienced this complication in one patient. She was admitted with post-prandial diarrhea, which led to the radiologic confirmation of the misplaced LAMS about a month after initial placement. We believe the risk of creating a gastrocolostomy increases when the interval between saline infusion and actual LAMS placement is prolonged, since the instilled fluid will not only dilate the jejunum but eventually the colon as well. Endoscopic ultrasound may not always be feasible to adequately differentiate a large bowel loop from a small bowel loop. Hence, caution is advised when identification of a target loop appears to be complicated and risk of saline infusion in the colon increases.
EUS-GE is primarily described in light of malignant GOO. However, a limited number of retrospective studies specifically assessed EUS-GE as treatment for benign GOO, demonstrating excellent results in terms of technical success [3, 67]. However, in contrast to patients in a palliative setting, the LAMS is expected to be indwelling for a longer duration. This poses additional concerns, such as bleeding or a buried LAMS [3]. James et al., however, observed a relatively low rate of surgical reinterventions (16.6%) in the period prior to resolution of the obstruction, suggesting that the LAMS can safely remain in situ until the cause of GOO is definitively solved. These results are based on small sample sizes, and therefore, we recommend leaving the LAMS indwelling for a minimum amount of time, thus decreasing the risks of long-term complications.
Future Directions
A steadily growing collection of evidence already has EUS-GE firmly embedded in the treatment arsenal of GOO. Numerous hospitals worldwide have already adopted EUS-GE as the primary treatment of choice of this debilitating syndrome [62•]. Nevertheless, up until today, LAMSs are not CE-marked or FDA-approved for creating a gastrointestinal anastomosis [27]. Therefore, future research should concentrate on outcomes that are sincerely meaningful from a patient perspective. In our opinion, two aspects are of special interest. First, short-term outcomes of EUS-GE, such as time to resumption of oral intake and length of hospital stay, should be assessed prospectively. Second, studies ought to focus on long-term LAMS patency, e.g., the rate of recurrent symptoms or reinterventions. Preferably, these studies should have a comparative design. Currently, several randomized controlled trials (RCTs) are planned or have recently started patient accrual. These results are eagerly awaited. Two studies compare EUS-GE with ES and are powered on the rate of GOO recurrence and reinterventions [68, 69]. Four other studies randomize patients between EUS-GE and SGJ and focus on either functional recovery, time to oral intake, or adverse events [70,71,72,73]. Moreover, our institute initiated the Dutch ENDURO-study. This RCT is unique in the sense that it is powered on two coprimary endpoints, focusing on short-term efficacy (time to oral intake of at least soft solids) and longer-term durability (persistent or recurrent symptoms of GOO requiring reintervention) [74]. In the end, the evidence gathered by these trials might be sufficient to definitively determine the place of EUS-GE for the treatment of GOO.
Conclusions
EUS-GE is an exciting and promising new approach for the treatment of GOO. It may combine the advantages of ES and SGJ, without adopting the negative effects. However, it should be emphasized that the currently published retrospective literature is prone to selection bias, rendering appropriate comparison between EUS-GE and the other existing treatments of GOO difficult. ES might still be the treatment of choice for patients with an expected short survival due to the small interval between treatment and clinical success. When comparing SGJ to EUS-GE, the latter might have a more beneficial risk profile. Nevertheless, EUS-GE remains a high-risk procedure which requires considerable expertise. Moreover, long-term patency of the LAMS has not been sufficiently compared with the patency of a surgical bypass. Therefore, well-designed trials are necessary to definitively determine the place of EUS-GE amongst ES and SGJ. Steadily, more and more hospitals with expertise in advanced endoscopy have adopted the treatment. Until reliable data has been collected, EUS-GE can be considered a safe and effective alternative to ES and SGJ.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Papanikolaou IS, Siersema PD. Gastric outlet obstruction: current status and future directions. Gut Liver. 2022;16:667–75. https://doi.org/10.5009/gnl210327.
Jue TL, Storm AC, Naveed M, Fishman DS, Qumseya BJ, McRee AJ, et al. ASGE guideline on the role of endoscopy in the management of benign and malignant gastroduodenal obstruction. Gastrointest Endosc. 2021;93:309–322.e4. https://doi.org/10.1016/j.gie.2020.07.063. ASGE guideline on the management of benign and malignant gastroduodenal obstruction.
James TW, Greenberg S, Grimm IS, Baron TH. EUS-guided gastroenteric anastomosis as a bridge to definitive treatment in benign gastric outlet obstruction. Gastrointest Endosc. 2020;91:537–42. https://doi.org/10.1016/j.gie.2019.11.017.
Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. Am J Gastroenterol. 2002;97:72–8. https://doi.org/10.1111/j.1572-0241.2002.05423.x.
House MG, Choti MA. Palliative therapy for pancreatic/biliary cancer. Surg Clin North Am. 2005;85:359–71. https://doi.org/10.1016/j.suc.2005.01.022.
Schmidt C, Gerdes H, Hawkins W, Zucker E, Zhou Q, Riedel E, et al. A prospective observational study examining quality of life in patients with malignant gastric outlet obstruction. Am J Surg. 2009;198:92–9. https://doi.org/10.1016/j.amjsurg.2008.09.030.
Lillemoe KD, Cameron JL, Hardacre JM, Sohn TA, Sauter PK, Coleman JA, et al. Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? - A prospective randomized trial. Ann Surg. 1999;230:322–30. https://doi.org/10.1097/00000658-199909000-00005.
van Hooft JE, Dijkgraaf MGW, Timmer R, Siersema PD, Fockens P. Independent predictors of survival in patients with incurable malignant gastric outlet obstruction: a multicenter prospective observational study. Scand J Gastroenterol. 2010;45:1217–22. https://doi.org/10.3109/00365521.2010.487916.
Boghossian MB, Funari MP, de Moura DTH, McCarty TR, Sagae VMT, Chen Y, et al. EUS-guided gastroenterostomy versus duodenal stent placement and surgical gastrojejunostomy for the palliation of malignant gastric outlet obstruction: a systematic review and meta-analysis. Langenbecks Arch Surg. 2021;406:1803–17. https://doi.org/10.1007/s00423-021-02215-8.
Ramai D, Facciorusso A, Crinò S, Adler D. EUS-guided gastroenteric anastomosis: a first-line approach for gastric outlet obstruction? Endosc Ultrasound. 2021;10:404. https://doi.org/10.4103/EUS-D-21-00238.
Ly J, O’Grady G, Mittal A, Plank L, Windsor JA. A systematic review of methods to palliate malignant gastric outlet obstruction. Surg Endosc. 2010;24:290–7. https://doi.org/10.1007/s00464-009-0577-1.
Wilson RG, Varma JS. Laparoscopic gastroenterostomy for malignant duodenal obstruction. Br J Surg. 2005;79:1348–1348. https://doi.org/10.1002/bjs.1800791235.
Krishnamoorthi R, Bomman S, Benias P, Kozarek RA, Peetermans JA, McMullen E, et al. Efficacy and safety of endoscopic duodenal stent versus endoscopic or surgical gastrojejunostomy to treat malignant gastric outlet obstruction: systematic review and meta-analysis. Endosc Int Open. 2022;10:E874–97. https://doi.org/10.1055/a-1794-0635.
Zhang LP, Tabrizian P, Nguyen S, Telem D, Divino C. Laparoscopic gastrojejunostomy for the treatment of gastric outlet obstruction. JSLS. 2011;15:169–73. https://doi.org/10.4293/108680811X13022985132074.
Cheung SLH, Teoh AYB. Optimal management of gastric outlet obstruction in unresectable malignancies. Gut Liver. 2022;16:190–7. https://doi.org/10.5009/gnl210010.
van Halsema EE, Rauws EAJ, Fockens P, van Hooft JE. Self-expandable metal stents for malignant gastric outlet obstruction: a pooled analysis of prospective literature. World J Gastroenterol. 2015;21:12468–81. https://doi.org/10.3748/wjg.v21.i43.12468.
Jeurnink SM, Steyerberg EW, van Hooft JE, van Eijck CH, Schwartz MP, Vleggaar FP, et al. Surgical gastrojejunostomy or endoscopic stent placement for the palliation of malignant gastric outlet obstruction (SUSTENT study): a multicenter randomized trial. Gastrointest Endosc. 2010;71:490–9. https://doi.org/10.1016/j.gie.2009.09.042.
Mintziras I, Miligkos M, Wachter S, Manoharan J, Bartsch DK. Palliative surgical bypass is superior to palliative endoscopic stenting in patients with malignant gastric outlet obstruction: systematic review and meta-analysis. Surg Endosc. 2019;33:3153–64. https://doi.org/10.1007/s00464-019-06955-z.
Binmoeller KF, Shah JN. Endoscopic ultrasound-guided gastroenterostomy using novel tools designed for transluminal therapy: a porcine study. Endoscopy. 2012;44:499–503. https://doi.org/10.1055/s-0032-1309382.
Bronswijk M, Vanella G, Petrone MC, van Malenstein H, Laleman W, Arcidiacono PG, et al. EUS-guided gastroenterostomy: less is more! The wireless EUS-guided gastroenterostomy simplified technique. VideoGIE. 2020;5:442. https://doi.org/10.1016/j.vgie.2020.06.012.
Kastelijn JB, Moons LMG, Garcia-Alonso FJ, Pérez-Miranda M, Masaryk V, Will U, et al. Patency of endoscopic ultrasound-guided gastroenterostomy in the treatment of malignant gastric outlet obstruction. Endosc Int Open. 2020;8:E1194–201. https://doi.org/10.1055/a-1214-5659.
Fritscher-Ravens A, Mosse CA, Mills TN, Mukherjee D, Park P-O, Swain P. A through-the-scope device for suturing and tissue approximation under EUS control. Gastrointest Endosc. 2002;56:a129084. https://doi.org/10.1067/mge.2002.129084.
Fritscher-Ravens A, Mosse CA, Mukherjee D, Mills T, Park P-O, Swain CP. Transluminal endosurgery: single lumen access anastomotic device for flexible endoscopy. Gastrointest Endosc. 2003;58:585–91. https://doi.org/10.1016/s0016-5107(03)02006-6.
Binmoeller KF, Shah J. A novel lumen-apposing stent for transluminal drainage of nonadherent extraintestinal fluid collections. Endoscopy. 2011;43:337–42. https://doi.org/10.1055/s-0030-1256127.
Choi J-H, Kozarek RA, Larsen MC, Ross AS, Law JK, Krishnamoorthi R, et al. Effectiveness and safety of lumen-apposing metal stents in endoscopic interventions for off-label indications. Dig Dis Sci. 2022;67:2327–36. https://doi.org/10.1007/s10620-021-07270-1.
Binmoeller KF, DeSimio T, Donovan R. Design considerations of the AXIOS stent and electrocautery enhanced delivery system. Tech Innov Gastrointest Endosc. 2020;22:3–8. https://doi.org/10.1016/j.tgie.2019.150653.
Hindryckx P, Degroote H. Lumen-apposing metal stents for approved and off-label indications: a single-centre experience. Surg Endosc. 2021;35:6013–20. https://doi.org/10.1007/s00464-020-08090-6.
Barthet M, Binmoeller KF, Vanbiervliet G, Gonzalez JM, Baron TH, Berdah S. Natural orifice transluminal endoscopic surgery gastroenterostomy with a biflanged lumen-apposing stent: first clinical experience (with videos). Gastrointest Endosc. 2015;81:215–8. https://doi.org/10.1016/j.gie.2014.09.039.
Khashab MA, Kumbhari V, Grimm IS, Ngamruengphong S, Aguila G, el Zein M, et al. EUS-guided gastroenterostomy: the first U.S. clinical experience (with video). Gastrointest Endosc. 2015;82:932–8. https://doi.org/10.1016/j.gie.2015.06.017.
Ribas PHBV, de Moura DTH, Proença IM, do Monte Júnior ES, Yvamoto EY, Hemerly MC, et al. Endoscopic ultrasound-guided gastroenterostomy for the palliation of gastric outlet obstruction (GOO): a systematic review and meta-analysis of the different techniques. Cureus. 2022;14:e31526. https://doi.org/10.7759/cureus.31526.
Irani S, Itoi T, Baron TH, Khashab M. EUS-guided gastroenterostomy: techniques from east to west. VideoGIE. 2020;5:48–50. https://doi.org/10.1016/j.vgie.2019.10.007.
Itoi T, Itokawa F, Uraoka T, Gotoda T, Horii J, Goto O, et al. Novel EUS-guided gastrojejunostomy technique using a new double-balloon enteric tube and lumen-apposing metal stent (with videos). Gastrointest Endosc. 2013;78:934–9. https://doi.org/10.1016/j.gie.2013.09.025.
Chen Y-I, Kunda R, Storm AC, Aridi HD, Thompson CC, Nieto J, et al. EUS-guided gastroenterostomy: a multicenter study comparing the direct and balloon-assisted techniques. Gastrointest Endosc. 2018;87:1215–21. https://doi.org/10.1016/j.gie.2017.07.030.
Wannhoff A, Ruh N, Meier B, Riecken B, Caca K. Endoscopic gastrointestinal anastomoses with lumen-apposing metal stents: predictors of technical success. Surg Endosc. 2021;35:1997–2004. https://doi.org/10.1007/s00464-020-07594-5.
Xu G, Shen Y, Lv Y, Zhou X, Li W, Wang Y, et al. Safety and efficacy of endoscopic ultrasound-guided gastroenterostomy using double balloon occlusion methods: a clinical retrospective study in 36 patients with malignant gastric outlet obstruction. Endosc Int Open. 2020;8:E1690–7. https://doi.org/10.1055/a-1221-9656.
Bejjani M, Ghandour B, Subtil JC, Martínez-Moreno B, Sharaiha RZ, Watson RR, et al. Clinical and technical outcomes of patients undergoing endoscopic ultrasound-guided gastroenterostomy using 20-mm vs. 15-mm lumen-apposing metal stents. Endoscopy. 2022;54:680–7. https://doi.org/10.1055/a-1654-6914. Retrospective study comparing 20 mm with 15 mm LAMS.
Iqbal U, Khara HS, Hu Y, Kumar V, Tufail K, Confer B, et al. EUS-guided gastroenterostomy for the management of gastric outlet obstruction: a systematic review and meta-analysis. Endosc Ultrasound. 2020;9:16–23. https://doi.org/10.4103/eus.eus_70_19.
Kumar A, Chandan S, Mohan BP, Atla PR, McCabe EJ, Robbins DH, et al. EUS-guided gastroenterostomy versus surgical gastroenterostomy for the management of gastric outlet obstruction: a systematic review and meta-analysis. Endosc Int Open. 2022;10:E448–58. https://doi.org/10.1055/a-1765-4035.
McCarty TR, Garg R, Thompson CC, Rustagi T. Efficacy and safety of EUS-guided gastroenterostomy for benign and malignant gastric outlet obstruction: a systematic review and meta-analysis. Endosc Int Open. 2019;7:E1474–82. https://doi.org/10.1055/a-0996-8178.
Ghandour B, Bejjani M, Irani SS, Sharaiha RZ, Kowalski TE, Pleskow DK, et al. Classification, outcomes, and management of misdeployed stents during EUS-guided gastroenterostomy. Gastrointest Endosc. 2022;95:80–9. https://doi.org/10.1016/j.gie.2021.07.023. Retrospective study describing outcomes and management of EUS-GE misdeployment.
Jovani M, Ichkhanian Y, Parsa N, Singh S, Brewer Gutierrez OI, Keane MG, et al. Assessment of the learning curve for EUS-guided gastroenterostomy for a single operator. Gastrointest Endosc. 2021;93:1088–93. https://doi.org/10.1016/j.gie.2020.09.041.(Learning-curveassessmentofEUS-GE).
Tyberg A, Kats D, Choi A, Gaidhane M, Nieto J, Kahaleh M. Endoscopic ultrasound guided gastroenterostomy: what is the learning curve? J Clin Gastroenterol. 2021;55:691–3. https://doi.org/10.1097/MCG.0000000000001400.(Learning-curveassessmentofEUS-GE).
Boston Scientific Corporation. AXIOS Stent and Electrocautery Enhanced Delivery System. Prescriptive Information 2015. https://www.bostonscientific.com/content/dam/bostonscientific/endo/portfolio-group/AXIOS/dfu_AXIOS-Stent-and-Electrocautery-Enhanced-system.pdf. Accessed 23 Jan 2023.
Kerdsirichairat T, Irani S, Yang J, Brewer Gutierrez OI, Moran R, Sanaei O, et al. Durability and long-term outcomes of direct EUS-guided gastroenterostomy using lumen-apposing metal stents for gastric outlet obstruction. Endosc Int Open. 2019;7:E144–50. https://doi.org/10.1055/a-0799-9939.
Taibi A, Durand Fontanier S, Derbal S, Lepetit H, Christou N, Fredon F, et al. What is the ideal indwelling time for metal stents after endoscopic ultrasound-guided gastrojejunostomy? Case report of delayed iatrogenic perforation with a review of the literature. Dig Endosc. 2020;32:816–22. https://doi.org/10.1111/den.13645.
Ge PS, Young JY, Dong W, Thompson CC. EUS-guided gastroenterostomy versus enteral stent placement for palliation of malignant gastric outlet obstruction. Surg Endosc. 2019;33:3404–11. https://doi.org/10.1007/s00464-018-06636-3. Retrospective comparison of EUS-GE and ES.
Chen YI, Itoi T, Baron TH, Nieto J, Haito-Chavez Y, Grimm IS, et al. EUS-guided gastroenterostomy is comparable to enteral stenting with fewer re-interventions in malignant gastric outlet obstruction. Surg Endosc. 2017;31:2946–52. https://doi.org/10.1007/s00464-016-5311-1. Retrospective comparison of EUS-GE and ES.
van Wanrooij RLJ, Vanella G, Bronswijk M, de Gooyer P, Laleman W, van Malenstein H, et al. Endoscopic ultrasound-guided gastroenterostomy versus duodenal stenting for malignant gastric outlet obstruction: an international, multicenter, propensity score-matched comparison. Endoscopy. 2022;54:1023–31. https://doi.org/10.1055/a-1782-7568. Retrospective comparison of EUS-GE and ES.
Sánchez-Aldehuelo R, Subtil Iñigo JC, Martínez Moreno B, Gornals J, Guarner-Argente C, Repiso Ortega A, et al. EUS-guided gastroenterostomy versus duodenal self-expandable metal stent for malignant gastric outlet obstruction: results from a nationwide multicenter retrospective study (with video). Gastrointest Endosc. 2022;96:1012–1020.e3. https://doi.org/10.1016/j.gie.2022.07.018. Retrospective comparison of EUS-GE and ES.
Chan SM, Dhir V, Chan YYY, Cheung CHN, Chow JCS, Wong IWM, et al. Endoscopic ultrasound-guided balloon-occluded gastrojejunostomy bypass, duodenal stent or laparoscopic gastrojejunostomy for unresectable malignant gastric outlet obstruction. Dig Endosc. 2022. https://doi.org/10.1111/den.14472. Retrospective comparison of EUS-GE, ES, and SGJ.
Jaruvongvanich V, Mahmoud T, Abu Dayyeh BK, Chandrasekhara V, Law R, Storm AC, et al. Endoscopic ultrasound-guided gastroenterostomy for the management of gastric outlet obstruction: a large comparative study with long-term follow-up. Endosc Int Open. 2022;11:E60–E66. https://doi.org/10.1055/a-1976-2279. Retrospective comparison of EUS-GE, ES, and SGJ.
van der Merwe SW, van Wanrooij RLJ, Bronswijk M, Everett S, Lakhtakia S, Rimbas M, et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2022;54:185–205. https://doi.org/10.1055/a-1717-1391.ESGE guideline regarding EUS-guided interventions.
Perez-Miranda M, Tyberg A, Poletto D, Toscano E, Gaidhane M, Desai AP, et al. EUS-guided gastrojejunostomy versus laparoscopic gastrojejunostomy: an international collaborative study. J Clin Gastroenterol. 2017;51:896–9. https://doi.org/10.1097/MCG.0000000000000887. Retrospective comparison of EUS-GE and SGJ.
Bronswijk M, Vanella G, van Malenstein H, Laleman W, Jaekers J, Topal B, et al. Laparoscopic versus EUS-guided gastroenterostomy for gastric outlet obstruction: an international multicenter propensity score-matched comparison (with video). Gastrointest Endosc. 2021;94:526–536.e2. https://doi.org/10.1016/j.gie.2021.04.006. Retrospective comparison of EUS-GE and SGJ.
Kouanda A, Binmoeller K, Hamerski C, Nett A, Bernabe J, Watson R. Endoscopic ultrasound-guided gastroenterostomy versus open surgical gastrojejunostomy: clinical outcomes and cost effectiveness analysis. Surg Endosc. 2021;35:7058–67. https://doi.org/10.1007/s00464-020-08221-z. Retrospective comparison of EUS-GE and SGJ.
Abbas A, Dolan RD, Bazarbashi AN, Thompson CC. Endoscopic ultrasound-guided gastroenterostomy versus surgical gastrojejunostomy for the palliation of gastric outlet obstruction in patients with peritoneal carcinomatosis. Endoscopy. 2022;54:671–9. https://doi.org/10.1055/a-1708-0037. Retrospective comparison of EUS-GE and SGJ in patients with peritoneal carcinomatosis.
Khashab MA, Bukhari M, Baron TH, Nieto J, el Zein M, Chen Y-I, et al. International multicenter comparative trial of endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for the treatment of malignant gastric outlet obstruction. Endosc Int Open. 2017;5:E275–81. https://doi.org/10.1055/s-0043-101695. Retrospective comparison of EUS-GE and SGJ.
Navarra G, Musolino C, Venneri A, de Marco ML, Bartolotta M. Palliative antecolic isoperistaltic gastrojejunostomy: a randomized controlled trial comparing open and laparoscopic approaches. Surg Endosc. 2006;20:1831–4. https://doi.org/10.1007/s00464-005-0454-5.
Boston Scientific Corporation. Hot AXIOSTM Stent and Electrocautery-Enhanced Delivery System. Ordering Information 2023. https://www.bostonscientific.com/en-EU/products/stents-gastrointestinal/axios-stent-and-electrocautery-enhanced-delivery-system/axios-ordering-information.html (accessed January 23, 2023).
TaeWoong. Niti-S Hot SPAXUSTM Stent & Electrocautery Stent Delivery System 2019. http://www.taewoongmedical.com/in/product/product_view.php?part1_idx=1&part2_idx=2&part_idx=11&idx=54 (accessed January 23, 2023).
Sharma C, Eltawil KM, Renfrew PD, Walsh MJ, Molinari M. Advances in diagnosis, treatment and palliation of pancreatic carcinoma: 1990–2010. World J Gastroenterol. 2011;17:867–97. https://doi.org/10.3748/wjg.v17.i7.867.
Vanella G, Bronswijk M, van Wanrooij RL, Dell’Anna G, Laleman W, van Malenstein H, et al. Combined endoscopic management of biliary and gastric outlet obstruction (CABRIOLET Study): a multicenter retrospective analysis. DEN Open. 2023;3. https://doi.org/10.1002/deo2.132. Retrospective study focusing on the optimal management of concomitant biliary and gastric outlet obstruction.
Bednarsch J, Czigany Z, Heise D, Zimmermann H, Boecker J, Ulmer TF, et al. Influence of peritoneal carcinomatosis on perioperative outcome in palliative gastric bypass for malignant gastric outlet obstruction - a retrospective cohort study. World J Surg Oncol. 2020;18:25. https://doi.org/10.1186/s12957-020-1803-5. Retrospective study assessing patients with gastric outlet obstruction and ascites who underwent EUS-GE.
Basha J, Lakhtakia S, Yarlagadda R, Nabi Z, Gupta R, Ramchandani M, et al. Gastric outlet obstruction with ascites: EUS-guided gastro-enterostomy is feasible. Endosc Int Open. 2021;9:E1918–23. https://doi.org/10.1055/a-1642-7892.
Fabbri C, Binda C, Fugazzola P, Sbrancia M, Tomasoni M, Coluccio C, et al. Hybrid gastroenterostomy using a lumen-apposing metal stent: a case report focusing on misdeployment and systematic review of the current literature. World J Emerg Surg. 2022;17:1–10. https://doi.org/10.1186/s13017-022-00409-z.
Tyberg A, Saumoy M, Kahaleh M. Using NOTES to salvage a misdeployed lumen-apposing metal stent during an endoscopic ultrasound-guided gastroenterostomy. Endoscopy. 2017;49:1007–8. https://doi.org/10.1055/s-0043-113551.
Chen Y-I, James TW, Agarwal A, Baron TH, Itoi T, Kunda R, et al. EUS-guided gastroenterostomy in management of benign gastric outlet obstruction. Endosc Int Open. 2018;06:E363–9. https://doi.org/10.1055/s-0043-123468.
ClinicalTrials.gov. Identifier NCT03259763, EUS-GE vs ES for palliation of gastric outlet obstruction. Bethesda (MD): National Library of Medicine (US) 2022. https://clinicaltrials.gov/ct2/show/NCT03259763 (accessed January 27, 2023).
ClinicalTrials.gov. Identifier NCT03823690, EPASS versus uncovered duodenal stent for unresectable malignant gastric outlet obstruction. Bethesda (MD): National Library of Medicine (US) 2022. https://clinicaltrials.gov/ct2/show/NCT03823690?recrs=ab&cond=gastric+outlet+obstruction&draw=2&rank=5 (accessed January 27, 2023).
ClinicalTrials.gov. Identifier NCT05605327, EUS-guided versus laparoscopic gastrojejunostomy for malignant gastric outlet obstruction (EATING). Bethesda (MD): National Library of Medicine (US) 2022. https://clinicaltrials.gov/ct2/show/NCT05605327 (accessed January 28, 2023).
ClinicalTrials.gov. Identifier NCT05548114, Randomized trial of EUS-guided gastrojejunostomy and surgical gastrojejunostomy in gastric outlet obstruction. Bethesda (MD): National Library of Medicine (US) 2022. https://clinicaltrials.gov/ct2/show/NCT05548114?cond=%22Gastric+Outlet+Obstruction%22&draw=2&rank=3 (accessed January 27, 2023).
ClinicalTrials.gov. Identifier NCT05561907, Enteral anastomosis for the treatment of gastric outlet obstruction: a randomized controlled study comparing endoscopic versus surgical gastrojejunostomy (EAT-GO). Bethesda (MD): National Library of Medicine (US) 2022. https://clinicaltrials.gov/ct2/show/NCT05561907?cond=%22Gastric+Outlet+Obstruction%22&draw=2&rank=1 (accessed January 27, 2023).
ClinicalTrials.gov. Identifier NCT05564143, Endoscopic ultrasound-guided versus surgical gastroenterostomy for malignant gastric outlet obstruction. Bethesda (MD): National Library of Medicine (US) 2022. https://clinicaltrials.gov/ct2/show/NCT05564143?cond=%22Gastric+Outlet+Obstruction%22&draw=2&rank=5 (accessed January 27, 2023).
International Clinical Trials Registry Platform. Identifier NL9592, Endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for palliation of malignant gastric outlet obstruction (ENDURO-study). World Health Organisation 2021. https://trialsearch.who.int/Trial2.aspx?TrialID=NL9592 (accessed February 21, 2023).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Yorick van de Pavert reports no conflicts of interest. Leon Moons is a consultant for Boston Scientific. Auke Bogte reports no conflicts of interest. Frank Vleggaar is a consultant for Boston Scientific.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van de Pavert, Y.L., Moons, L.M.G., Bogte, A. et al. Innovations in the Treatment of Gastric Outlet Obstruction: Is This the Era of Endoscopic Ultrasonography-Guided Gastroenterostomy?. Curr Treat Options Gastro (2023). https://doi.org/10.1007/s11938-023-00417-1
Accepted:
Published:
DOI: https://doi.org/10.1007/s11938-023-00417-1